
Abstract
Objective:
Women with intellectual and developmental disabilities (IDD) have high rates of adverse perinatal outcomes. However, the perinatal health of women with co-occurring IDD and mental illness (dual diagnosis) is largely unknown. Our objectives were to 1) describe a cohort of women with dual diagnosis in terms of their social and health characteristics and 2) compare their risks for adverse maternal and neonatal outcomes to those of women with IDD only.
Method:
We conducted a population-based study using linked Ontario (Canada) health and social services administrative data to identify singleton obstetric deliveries to women with dual diagnosis (n = 2080) and women with IDD only (n = 1852; 2002–2012). Primary maternal outcomes were gestational diabetes, gestational hypertension, preeclampsia/eclampsia, and venous thromboembolism. Primary neonatal outcomes were preterm birth, small for gestational age, and large for gestational age. We also examined several secondary outcomes.
Results:
Women with dual diagnosis were more likely than women with IDD only to live in poor neighborhoods and to have prepregnancy health conditions; however, they had more frequent prenatal care. Infants born to women with dual diagnosis had increased risks for preterm birth (adjusted relative risk [aRR] 1.31, 95% confidence interval [CI] 1.08 to 1.59) and neonatal morbidity (aRR 1.35, 95% CI 1.03 to 1.76) compared with infants born to women with IDD only. All other primary and secondary outcomes were nonsignificant.
Conclusions:
Comorbid mental illness contributes little additional risk for adverse perinatal outcomes among women with IDD. Women with dual diagnosis and women with IDD alone require increased surveillance for maternal and neonatal complications.
Intellectual and developmental disabilities (IDD) are neurodevelopmental disorders that are characterized by cognitive limitations and difficulties in practical, social, and conceptual domains. 1 Affecting 1 in every 100 adults, 2 IDD include fetal alcohol syndrome, autism, Down syndrome, and Fragile X syndrome. 1 Historically, childbearing among women with IDD has been uncommon, likely because of sterilization and institutionalization practices of the early to mid-20th century. 3 Recently, there has been an increase in the number of women with IDD receiving maternity services, suggesting a rising fertility rate. 4 In Ontario in 2009, there were 20.3 live births for every 1000 women with IDD. 5
Studies have shown that women with IDD, compared with those without IDD, are at increased risk for adverse maternal and neonatal outcomes. 6 –12 An Australian prospective cohort study found that women with IDD (N = 54) were at increased risk for preeclampsia. 6 Retrospective cohort studies from the United States 8,9 found that women with IDD (N = 340, N = 703) were at increased risk for caesarean delivery, preterm birth, and perinatal mortality. A Swedish retrospective cohort study 10,11 found that women with IDD (N = 326) were at increased risk for perinatal mortality, preterm birth, and small for gestational age. In the largest population-based cohort study on this topic to date, we found that Ontario women with IDD (N = 3932) were at increased risk for preeclampsia, venous thromboembolism, peripartum hemorrhage, severe obstetric morbidity, systemic maternal complications, preterm birth, small for gestational age, stillbirth, neonatal mortality, and neonatal morbidity. 12
Nearly half of women with IDD have a mental illness. 13 The co-occurrence of IDD and mental illness is sometimes labeled “dual diagnosis,” with the most common mental illness comorbidities being schizophrenia, depression, and anxiety. 13 Health outcomes of adults with dual diagnosis are worse than those of adults with IDD only; for example, they are more likely to have diabetes mellitus and cardiovascular disease. 14,15 Reasons include higher rates of poverty, substance use, and smoking among adults with dual diagnosis. 13,16,17 No previous studies have examined the perinatal health of women with dual diagnosis. We hypothesized that they would have higher rates of social and health risk factors and increased risk for adverse maternal and neonatal outcomes compared with women with IDD only.
The objectives of our study were to 1) describe a cohort of women with dual diagnosis in terms of their social and health characteristics and 2) compare their risks for adverse maternal and neonatal outcomes to those of women with IDD only.
Methods
Study Design and Setting
We undertook a population-based cohort study in Ontario, Canada. Ontario has 140 000 births each year and is Canada’s most populous province. 18 All prenatal and obstetric services delivered in and outside of hospitals are free of charge to Ontario residents. The current study included obstetric deliveries with a conception date between April 1, 2002, and March 31, 2012.
We obtained data from the Institute for Clinical Evaluative Sciences (ICES), a nonprofit, independent organization that holds data resulting from health care encounters of Ontario residents. ICES databases were linked using unique encoded identifiers and were analyzed at ICES. To identify study groups, we used the Canadian Institute for Health Information Discharge Abstract Database (hospitalizations), the Ontario Mental Health Reporting System (psychiatric hospitalizations), the National Ambulatory Care Reporting System (emergency department visits), the Ontario Health Insurance Plan database (primary care visits), and disability support information from the Ministry of Community and Social Services. 19 The MOMBABY data set, which is derived from the Canadian Institute for Health Information Discharge Abstract Database, was used to identify obstetric deliveries and to estimate conception date based on gestational age at delivery. 20 The Registered Persons Database (birth date, postal code) and ICES databases described above were used to create outcomes and covariates.
Diagnostic codes follow the Canadian Coding Standards for the International Statistical Classification of Diseases and Related Health Problems 10th Revision for hospital databases and physician billing claim codes for the Ontario Health Insurance Plan database. Procedural codes follow the Canadian Classification of Health Interventions. Sociodemographic information, primary diagnosis, physician billing claims, and procedures are reliable and valid. 21
Study Sample
We derived our sample of women with IDD from a cohort created using linked health and social services administrative data, in which all individuals aged 18 to 64 years with IDD in Ontario were identified as of April 1, 2009. 19 Individuals were classified as having IDD if they had a relevant diagnostic code recorded in health administrative data since inception of each database (≥2 physician visits or ≥1 emergency department visit or hospitalization) or in disability support program documentation. 19 Diagnoses included fetal alcohol syndrome, pervasive developmental disorders (e.g., autism), and chromosomal and autosomal anomalies (e.g., Down syndrome, Fragile X syndrome); a list of diagnostic codes is available elsewhere. 22 The underlying conceptual definition of IDD, covering neurodevelopmental disorders marked by common limitations in cognitive and adaptive functioning, is consistent with policy 23 and clinical 1 definitions. For the current study, we identified, among women with IDD aged 18 to 49 years, all singleton obstetric deliveries of live-born or stillborn infants (>20 weeks’ gestational age) whose estimated conception date was between April 1, 2002, and March 31, 2012.
This group was then divided into women with IDD only and women with IDD and a comorbid mental illness (“dual diagnosis”). Mental illness was determined by the presence of relevant diagnostic codes recorded in health administrative data (i.e., physician visits, emergency department visits, hospitalizations) in the 2 years preceding the estimated date of conception. Diagnoses included in the primary definition were schizophrenia or other psychotic disorders, bipolar disorder or major depression, other depression, anxiety disorders, personality disorders, adjustment disorders, and disorders of conduct or impulsivity (Supplementary Table S1). 24,25 We also considered a more specific definition including only major mental illness (i.e., schizophrenia or other psychotic disorders, bipolar disorder, or major depression). 26
We also had access to a cohort of women without IDD. They were divided into women with mental illness only (using the above definition) and women with neither IDD nor mental illness. We used these data for a sensitivity analysis.
Study Outcomes
Primary outcomes were adverse maternal and neonatal outcomes that are elevated among women with IDD 6 –12 and women with mental illness 27,28 and were hypothesized to be more common among women with dual diagnosis. Primary maternal outcomes were gestational diabetes, gestational hypertension, preeclampsia/eclampsia, and venous thromboembolism. Primary neonatal outcomes were preterm birth (<37 weeks’ gestational age), small for gestational age (sex-specific birth weight <10th percentile for gestational age), and large for gestational age (sex-specific birth weight >90th percentile for gestational age). Diagnostic codes for these outcomes have good sensitivity and specificity relative to clinical data. 29,30
Secondary outcomes were additional markers of adverse outcomes monitored by the Canadian Perinatal Surveillance System. 31 Secondary maternal outcomes were peripartum hemorrhage (i.e., antepartum, intrapartum, or postpartum hemorrhage), severe obstetric morbidity (i.e., placental infarction, placental abruption, obstetric embolism, uterine rupture, or septic shock), systemic maternal complications (i.e., cardiomyopathy, cardiac arrest, cardiac failure, myocardial infarction, pulmonary edema, cerebrovascular disease, acute respiratory distress syndrome, acute renal failure, hepatic failure, complications of anesthesia, disseminated intravascular coagulation, or status epilepticus), labour induction, caesarean delivery, and operative vaginal delivery. Secondary neonatal outcomes were perinatal mortality (i.e., stillbirth or neonatal mortality at less than 28 days), major congenital anomalies, and neonatal morbidity (i.e., respiratory distress syndrome, seizures, intraventricular hemorrhage, persistent fetal circulation, neonatal abstinence syndrome, sepsis, or congenital/neonatal infection).
Covariates
Based on models of social and health risk factors for adverse perinatal outcomes, 32 we measured covariates to 1) describe women with dual diagnosis and 2) adjust for differences between groups in multivariable models. We used validated algorithms where available: maternal age, parity, neighbourhood income quintile and region of residence (measured by maternal postal code 33 ), prepregnancy diabetes mellitus, 34 chronic hypertension, 35 thyroid disease, epilepsy, 36 substance-related disorders, and infant sex. We also measured early prenatal ultrasound receipt, adequacy of prenatal care (i.e., timing of prenatal care initiation and proportion of recommended visits received, as measured by the Kotelchuck Index), 37 and type of prenatal care provider, since the health care that a woman receives may also affect her pregnancy outcomes. 38
Statistical Analysis
We used frequencies and percentages to describe the sample. Standardized differences (SD), which are not influenced by sample size, were used to determine which characteristics were more common among women with dual diagnosis. To directly estimate risks of adverse maternal and neonatal outcomes among women with dual diagnosis compared with women with IDD only, we used modified Poisson regression 39 with generalized estimation equations to adjust the variance for clustering of deliveries to the same mother during the study period. 40 Adjusted relative risks (aRR) controlled for maternal age, parity, and other covariates which changed the unadjusted exposure-outcome association by more than 5%. 41 We considered prenatal care variables to be pathway variables (i.e., potentially explaining the association between dual diagnosis and adverse outcomes). We did not control for these variables in the main multivariable models but added them to the models in a second step to examine their impact on results. For analyses of gestational diabetes and gestational hypertension, women with prepregnancy diabetes mellitus and chronic hypertension, respectively, were excluded from these models. By definition, these women are not at risk for these outcomes. 42
In sensitivity analyses, we reran multivariable models including only major mental illness in the dual diagnosis group; women with other psychiatric diagnoses were excluded from the analysis.
To place our findings in a broader context, we conducted a sensitivity analysis in which we examined maternal and neonatal outcomes among women with dual diagnosis, women with IDD only, women with mental illness only, and women with neither condition.
SAS 9.2 (SAS Institute Inc., Cary, NC) was used for statistical analyses. Ethics approval for this study was obtained from the Sunnybrook Health Sciences Centre Research Ethics Board (Institute for Clinical Evaluative Sciences logged study 2014-0900-522-000).
Results
Social and Health Characteristics
Between 2002 and 2012, there were 2080 deliveries to 1369 women with dual diagnosis and 1852 deliveries to 1215 women with IDD only. When considering our 2 definitions of mental illness, 52.9% of women with IDD had a comorbid mental illness and 9.5% of women with IDD had a comorbid major mental illness.
Women with dual diagnosis were more likely than women with IDD only to live in the lowest neighbourhood income quintile (42.3% vs. 36.8%; SD 0.11) and to have preexisting diabetes mellitus (3.8% vs. 2.1%; SD 0.10), thyroid disease (8.9% vs. 6.1%; SD 0.11), and substance-related disorders (12.6% vs. 4.4%; SD 0.30; Table 1). Women with dual diagnosis were more likely than women with IDD only to begin prenatal care before the fourth month of pregnancy and to receive 110% or more of recommended prenatal care visits (i.e., “adequate plus” prenatal care; 54.6% vs. 36.1%; SD 0.38). They were also more likely than women with IDD only to have prenatal care shared by a family physician and obstetrician (48.6% vs. 38.9%; SD 0.20; also Table 1).
Baseline characteristics of study groups, Ontario, Canada, 2002–2012.
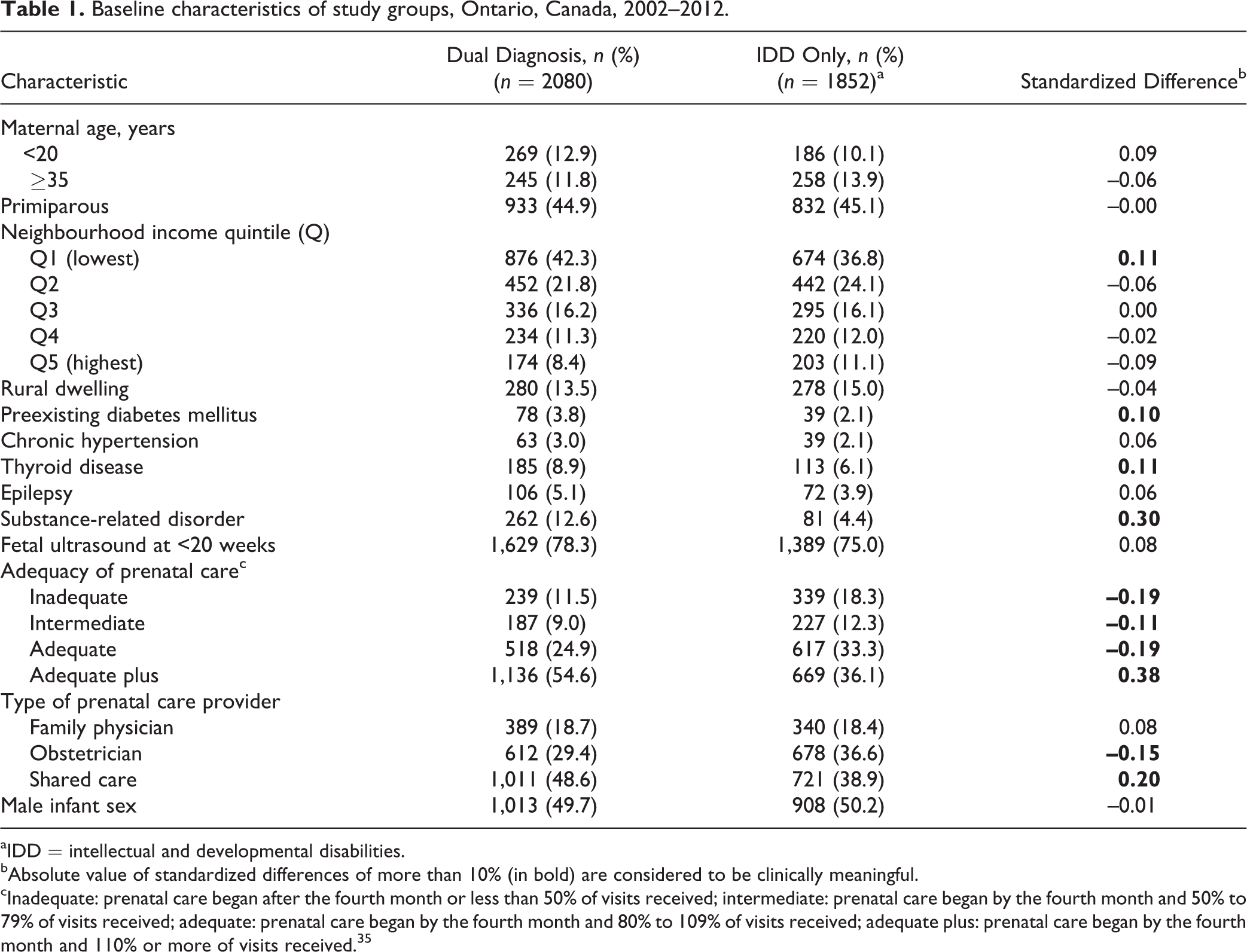
aIDD = intellectual and developmental disabilities.
bAbsolute value of standardized differences of more than 10% (in bold) are considered to be clinically meaningful.
cInadequate: prenatal care began after the fourth month or less than 50% of visits received; intermediate: prenatal care began by the fourth month and 50% to 79% of visits received; adequate: prenatal care began by the fourth month and 80% to 109% of visits received; adequate plus: prenatal care began by the fourth month and 110% or more of visits received. 35
Maternal and Neonatal Outcomes
In unadjusted analyses, women with dual diagnosis, compared with women with IDD only, had similar rates of gestational diabetes (3.1% vs. 3.2%), gestational hypertension (1.7% vs. 1.5%), preeclampsia/eclampsia (1.8% vs. 1.6%), and venous thromboembolism (1.2% vs. 1.1%). After controlling for confounding variables, aRRs were nonsignificant (Table 2). Adding prenatal care variables to the multivariable model did not change results.
Unadjusted and adjusted risks for primary maternal outcomes.a
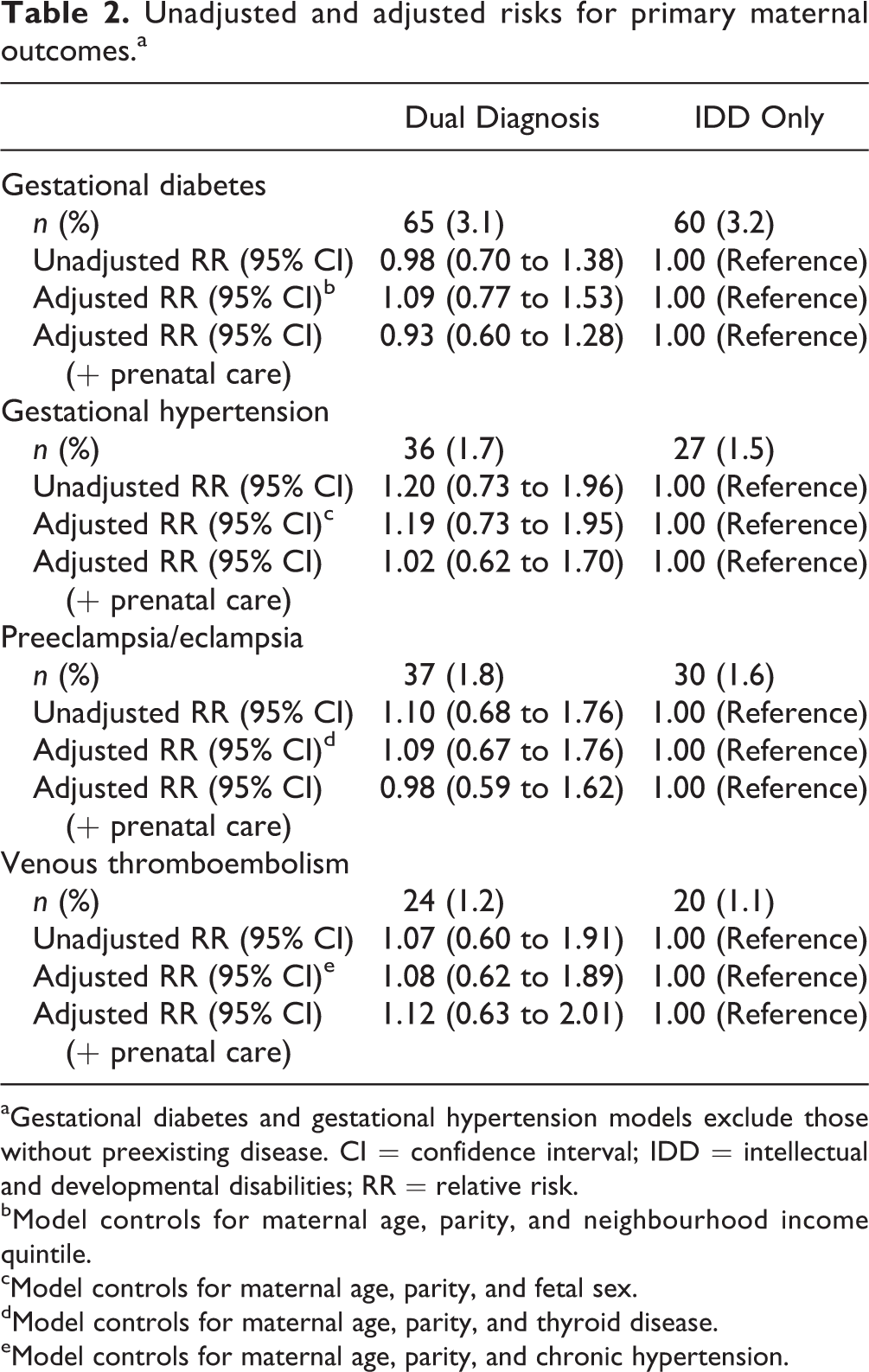
aGestational diabetes and gestational hypertension models exclude those without preexisting disease. CI = confidence interval; IDD = intellectual and developmental disabilities; RR = relative risk.
bModel controls for maternal age, parity, and neighbourhood income quintile.
cModel controls for maternal age, parity, and fetal sex.
dModel controls for maternal age, parity, and thyroid disease.
eModel controls for maternal age, parity, and chronic hypertension.
In unadjusted analyses, infants born to women with dual diagnosis, compared with those born to women with IDD only, had higher rates of preterm birth (12.2% vs. 9.4%). They had similar rates of small for gestational age (17.7% vs. 17.2%) and large for gestational age (7.7% vs. 8.8%). In adjusted analyses, they remained at increased risk for preterm birth (aRR 1.31, 95% confidence interval [CI] 1.08 to 1.59); aRRs for small and large for gestational age were nonsignificant (Table 3). Adding prenatal care variables to multivariable models completely attenuated the aRR for preterm birth.
Unadjusted and adjusted risks for primary neonatal outcomes.a
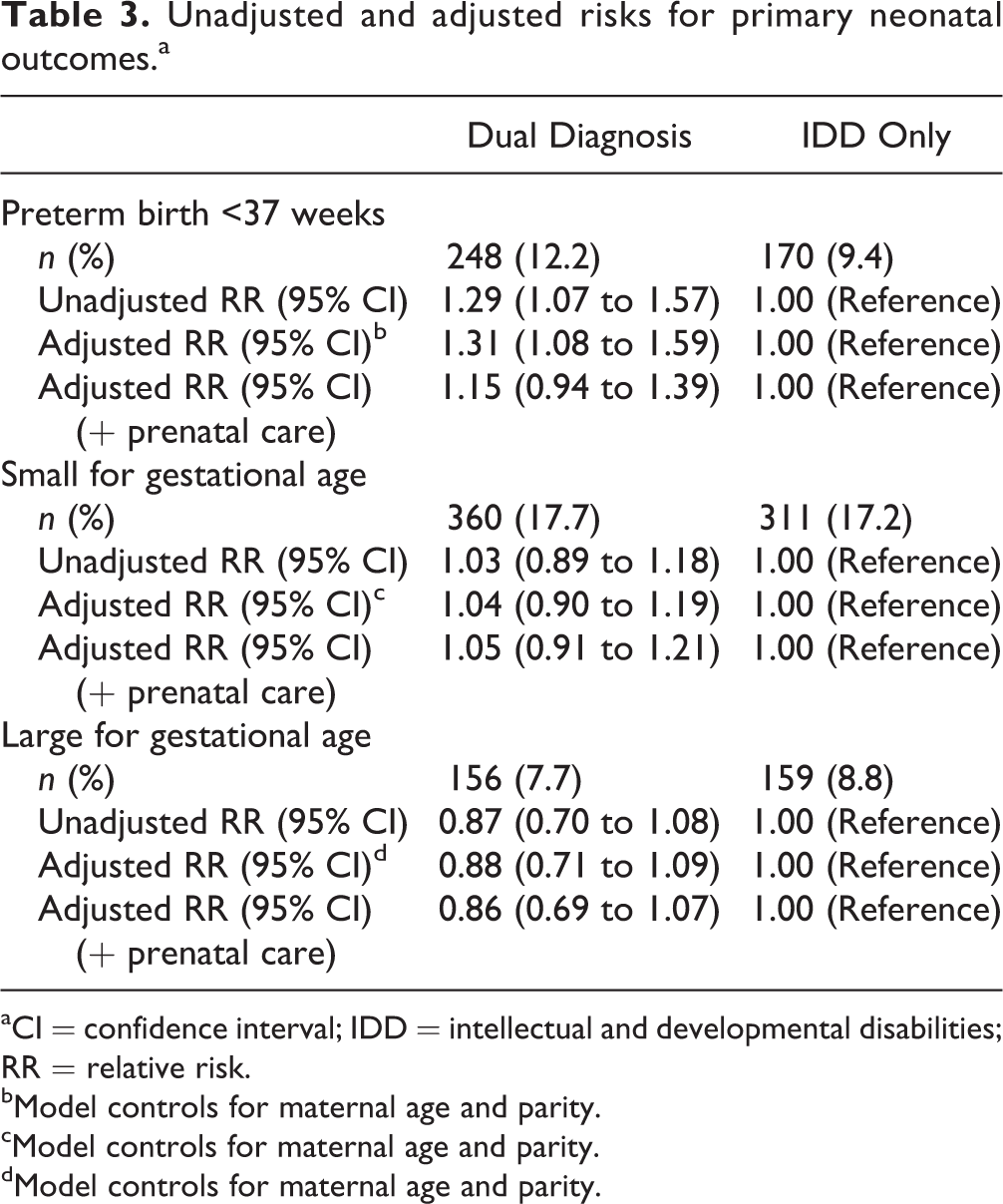
aCI = confidence interval; IDD = intellectual and developmental disabilities; RR = relative risk.
bModel controls for maternal age and parity.
cModel controls for maternal age and parity.
dModel controls for maternal age and parity.
For secondary outcomes, in both unadjusted and adjusted analyses, women with dual diagnosis were not at increased risk, compared with women with IDD only, for adverse maternal outcomes (Figure 1). Their infants were at increased risk only for neonatal morbidity (aRR 1.35, 95% CI 1.03 to 1.76; also Figure 1). Adding prenatal care variables to multivariable models completely attenuated the aRR for neonatal morbidity.
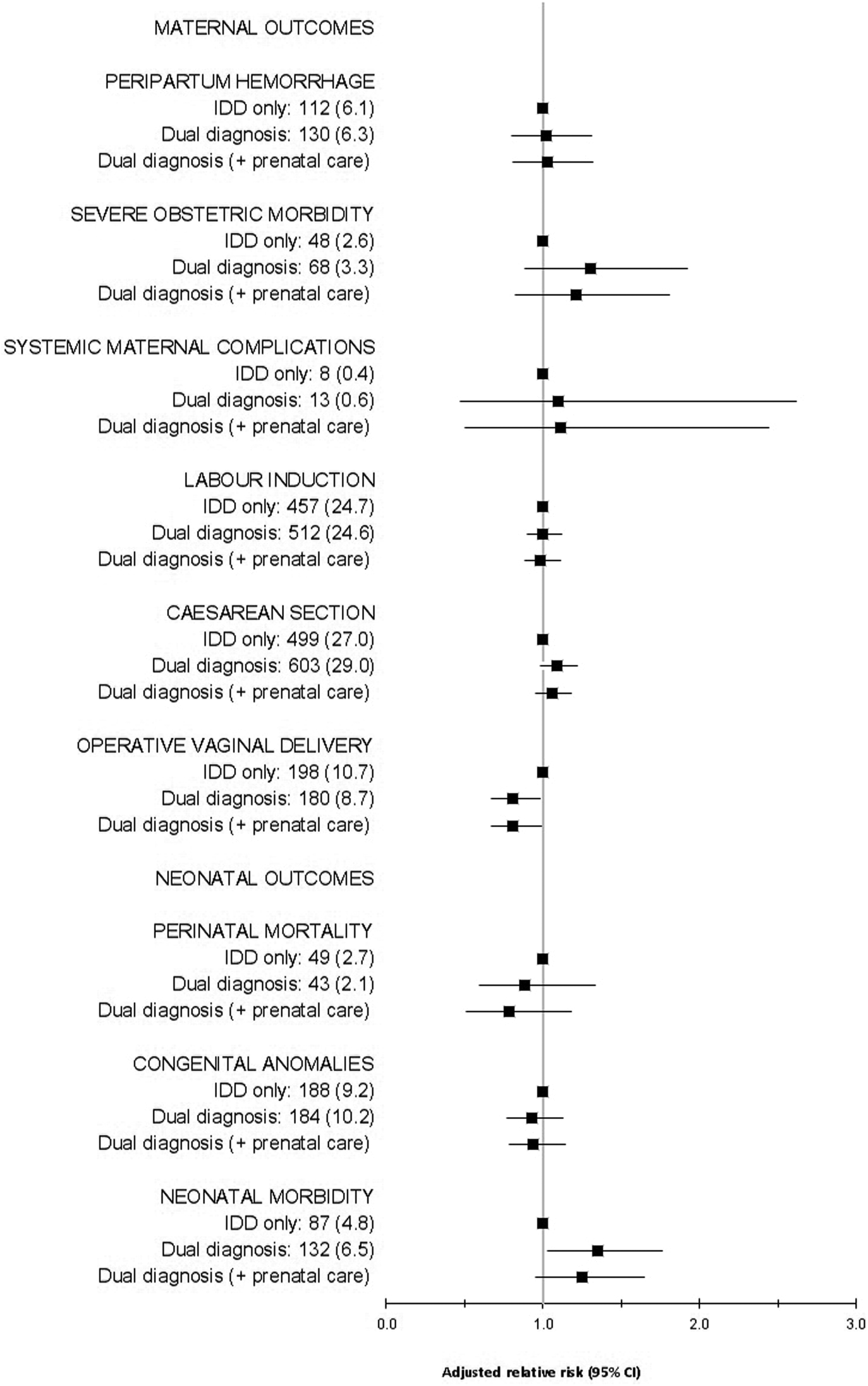
Frequency (n [%]) and adjusted risks for secondary maternal and neonatal outcomes.
Sensitivity Analyses
We reran multivariable models including only major mental illness. In unadjusted and adjusted analyses, women with dual diagnosis, compared with women with IDD only, were not at increased risk for adverse maternal outcomes (Supplementary Table S2). In unadjusted analyses, their infants were not at increased risk for primary neonatal outcomes or for perinatal mortality or congenital anomalies; they were at increased risk for neonatal morbidity (RR 1.83, 95% CI 1.22 to 2.75). All neonatal outcomes were nonsignificant in adjusted analyses (Supplementary Table S3).
To contextualize findings, we reran multivariable models for maternal and neonatal outcomes in women with dual diagnosis, women with IDD only, women with mental illness only, and women with neither condition. Characteristics of each group are shown in Supplementary Table S4. In general, risks for adverse maternal and neonatal outcomes among women with dual diagnosis and women with IDD only were increased compared with women with neither condition. Women with mental illness only had increased risks for adverse maternal and neonatal outcomes compared with women with neither condition, but the magnitude of these risks was smaller than that for women with dual diagnosis and women with IDD only (Supplementary Table S5).
Discussion
This is the first population-based analysis of the perinatal health of women with dual diagnosis. In our cohort of women with IDD, more than half had a comorbid mental illness, and nearly 1 in 10 had a comorbid major mental illness. Compared with women with IDD only, women with dual diagnosis were more likely to experience low income and high rates of prepregnancy health conditions. However, they received earlier and more frequent prenatal care and were more likely to receive care from both a family physician and obstetrician. Overall, women with dual diagnosis did not appear to have increased risks for adverse maternal outcomes. Their infants were at increased risk only for preterm birth and neonatal morbidity; these risks remained statistically significant after controlling for social and health risk factors but were attenuated after controlling for prenatal care variables.
The rate of mental illness in our cohort is slightly higher than that reported in women with IDD in general 13 ; this could be explained by the younger age range covered by our obstetric population. Our finding of higher rates of social and health risk factors among women with dual diagnosis is consistent with previous studies. These studies have shown high rates of poverty, chronic health conditions, and substance-related disorders among adults with dual diagnosis. 13,16,17 Our study is the first to confirm these risk factors among pregnant women with dual diagnosis. In a pregnant population, these factors carry particular importance, given their established associations with adverse perinatal outcomes. 43,44
There is no literature on dual diagnosis and pregnancy to which to compare our results regarding maternal and neonatal outcomes. In the general population, mental illness is associated with increased risk for adverse perinatal outcomes. 27,28 In our population of already vulnerable women with IDD, the presence of a comorbid mental illness did not contribute additional risk for adverse maternal outcomes but did have some effect on neonatal outcomes. Our finding that infants born to women with dual diagnosis were at increased risk for preterm birth and neonatal morbidity is consistent with previous research showing the impact of mental illness on risk for premature labour and adverse neonatal outcomes in the general population. 27,28 It is important to note that nearly all the rates of adverse maternal and neonatal outcomes among women with dual diagnosis and women with IDD only were higher than those in the general population. 12,31
Strengths and Limitations
A strength of our study is the size and representativeness of our cohort. This large cohort allowed us to examine rare but serious perinatal outcomes. By using linked health and social services administrative data, we achieved more complete ascertainment of IDD status than previous studies relying on clinical samples or on health administrative data only.
Our study has limitations that are inherent in studies relying on administrative data. Although we linked health and social services data in an effort to identify all adults with IDD in Ontario, some individuals may have been missed. This issue is not unique to our study, 45 and the prevalence of IDD in Ontario that our research group identified (0.8%) 22 is consistent with previous estimates. 2 Misclassification of mental illness may have occurred if symptoms were not recorded in the 2 years prior to pregnancy; however, we used this definition to capture active mental illness. Severity of mental illness was based on diagnosis and not limitations in daily functioning; our definitions may not fully capture the impact of mental illness. IDD and mental illness include a heterogeneous group of conditions; while it is possible that there could be variation in risk associated with different diagnoses within these groups, our broad definitions are consistent with clinical 1 and policy 23 definitions. We had no information on living situation, whether the pregnancy was planned, or whether the woman experienced abuse. Finally, it is possible that our sensitivity analysis of major mental illness was underpowered, particularly for rare maternal complications.
Interpretation
We chose primary outcomes based on the hypothesis that women with dual diagnosis would have increased risks for adverse maternal and neonatal outcomes because of their social and health risk factors. We observed that women with dual diagnosis had higher rates of poverty, prepregnancy health conditions, and substance-related disorders than women with IDD only. Multiple studies have demonstrated the bidirectional relationship between poverty and mental illness. 16,17 The high rate of preexisting diabetes mellitus among women with dual diagnosis may be explained by their use of psychotropic medications. 46 Substance-related disorders and mental illness often co-occur, contributing to high rates of “triple diagnosis” among individuals with IDD. 47 Earlier initiation of prenatal care, higher number of prenatal care visits, and greater likelihood of shared care between family physician and obstetrician among women with dual diagnosis may be explained by a recognition by health care professionals of the pregnancy risks associated with mental illness.
It is unclear why women with dual diagnosis were not at increased risk for adverse maternal outcomes compared with women with IDD only. One might speculate that their earlier and more frequent prenatal care compensated for their higher social and medical risks. However, when we added prenatal care variables as possible pathway variables to multivariable models, no differences in maternal outcomes between the groups were unmasked, suggesting that this is not the case. Timing and frequency of prenatal care, however, are only markers that may not fully reflect the adequacy of care received or the indications for care. It is possible that mental illness contributes little additional risk for maternal complications in a population that already has such high risks for poor outcomes. 6 –12 Although women with dual diagnosis were more likely to experience social and health risk factors than women with IDD only, these measured covariates may not fully capture adversities experienced by both groups. Higher rates of poverty, prepregnancy health conditions, and substance-related disorders in women with a comorbid mental illness may make little difference to maternal outcomes in a population with such a high baseline rate of these and other risk factors.
Consistent with our hypotheses, infants born to women with dual diagnosis, compared with those born to women with IDD only, were at increased risk for preterm birth and neonatal morbidity. However, they were not at increased risk for other adverse neonatal outcomes. Given the large number of comparisons, it is possible that statistically significant findings were due to chance. It is, however, likely that consistent with our hypotheses, high rates of poverty, poor maternal health, and substance use contribute to increased risk for preterm birth and neonatal morbidity among infants born to women with dual diagnosis. Risks remained statistically significant after controlling for these covariates. However, they were attenuated when prenatal care pathway variables were added to the models. Since women with dual diagnosis were more likely than women with IDD only to have “adequate plus” prenatal care, it is possible that this variable is, in fact, a proxy for a high-risk pregnancy. Such pregnancies would be expected to result in adverse neonatal outcomes. There are also other variables that could explain our findings. In particular, psychotropic medication use during pregnancy has been associated with premature labour, respiratory distress syndrome, and neonatal seizures 48,49 and could explain why infants born to women with dual diagnosis are more likely to be born preterm and experience neonatal morbidity.
Conclusion
Our findings suggest that comorbid mental illness contributes little additional risk for adverse maternal and neonatal outcomes in an already vulnerable population of women with IDD. However, absolute rates of adverse maternal and neonatal outcomes were higher in both groups compared with the general population. Therefore, women with IDD, regardless of whether or not they have a comorbid mental illness, require better prevention of social and health risk factors prior to pregnancy and increased surveillance for complications during pregnancy. Such efforts could reduce the rates of adverse maternal and neonatal outcomes among women with IDD only and women with dual diagnosis.
Footnotes
Authors’ Note
This article was presented as a poster presentation at the Second Biennial Perinatal Mental Health Meeting, Chicago, Illinois, November 4–6, 2015.
Acknowledgments
The opinions, results, and conclusions reported in this article are those of the authors and do not reflect that of the Province of Ontario or the data providers. No endorsement by the Province or the Institute for Clinical Evaluative Sciences is intended or should be inferred. Parts of this material are based on data and information compiled and provided by the Canadian Institute for Health Information (CIHI). However, the analyses, conclusions, opinions, and statements expressed herein are those of the author and not necessarily those of CIHI. The authors also acknowledge the support of the Health Care Access Research and Developmental Disabilities (H-CARDD) research program, of which this study is a part.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Simone Vigod was awarded a one-time consulting honorarium from MDH Consulting for continuing medical education activities related to perinatal mental health.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We gratefully acknowledge the Province of Ontario for their support of this article through their research grants program. The first author is funded by a Canadian Institutes of Health Research Postdoctoral Award (MFE-135409).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.