
Abstract
Objective:
Neuropsychiatric symptoms (NPS) may be the first manifestation of an underlying neurocognitive disorder. We undertook a review to provide an update on the epidemiology and etiological mechanisms of NPS that occur in mild cognitive impairment (MCI) and just before the onset of MCI. We discuss common clinical presentations and the implications for diagnosis and care.
Method:
The authors conducted a selective review of the literature regarding the emergence of NPS in late life, before and after the onset of MCI. We discuss recent publications that explore the epidemiology and etiological mechanisms of NPS in the earliest clinical stages of these disorders.
Results:
NPS have been reported in 35% to 85% of adults with MCI and also occur in advance of cognitive decline. The occurrence of NPS for the first time in later life should increase suspicion for an underlying neurocognitive disorder. The presenting symptom may provide a clue regarding the etiology of the underlying disorder, and the co-occurrence of NPS may herald a more accelerated cognitive decline.
Conclusions:
NPS are prevalent in the early clinical stages of neurocognitive disorders and can serve as both useful diagnostic and prognostic indicators. Recognition of NPS as early manifestations of neurocognitive disorders will become increasingly important as we move towards preventative strategies and disease-modifying treatments that may be most effective when deployed in the earliest stages of disease.
In Canada, the number of people living with dementia is projected to increase from 747,000 in 2011 to 1.4 million by 2031. 1 The associated costs could increase from $33 billion to $293 billion annually by 2040 unless novel therapeutic and preventative approaches are developed. 1 Symptomatic treatments for neurocognitive disorders such as Alzheimer disease (AD), although helpful, have had a limited impact on disease progression. Novel therapeutic agents, designed to act on underlying neuropathological processes, have had limited success in established disease. It appears that earlier intervention, before the disease has become truly established, may be necessary to prevent further progression. 2 Mild cognitive impairment (MCI) or mild neurocognitive disorder is defined by a decrement in cognitive functioning that goes beyond normal aging but does not yet meet criteria for dementia or major neurocognitive disorder. 3 This represents an early clinical stage during which there may be an opportunity to preserve function and prevent further cognitive decline.
In this context, there has been increased interest in neuropsychiatric symptoms (NPS) and how they may facilitate early diagnosis and prevention of cognitive decline. NPS have been described in 35% to 85% of adults with MCI 4,5 and typically increase in frequency and severity with disease progression. 6 However, NPS are often present in the earliest clinical stages of disease and may precede the onset of measurable cognitive decline. 4,7 Individuals in these early clinical stages may present to psychiatric services, and it is not uncommon for individuals subsequently diagnosed with a neurodegenerative disorder to have initially received a psychiatric diagnosis. 8 In one retrospective review of 252 patients diagnosed with neurodegenerative disease, 28.2% had initially received a psychiatric diagnosis of which depression was the most common. Individuals with the behavioural variant of frontotemporal dementia (bvFTD) (50.7%), which is characterized by early changes in behaviour such as apathy, loss of empathy, and disinhibition, were at greatest risk of initial misdiagnosis, followed by those who were ultimately diagnosed with AD (23.1%). 8 A number of studies have noted that NPS are associated with accelerated cognitive decline, raising the possibility that effective treatment might not only reduce psychiatric morbidity but also delay cognitive and functional decline. 9,10
In view of the potential significance of NPS both before and during MCI, we undertook a selective review of the literature on this topic. We review the recent literature regarding the prevalence of NPS, with a focus on the symptoms of apathy, depression, anxiety, psychosis, agitation, and disinhibition and their association with evolving neurocognitive disorders. Finally, we discuss the implications of early detection for treatment and clinical care.
Methods
The authors conducted a selective review of publications in English until November 2, 2015, using the Medline database. Search terms included neuropsychiatric symptoms, behavioural/behavioral symptoms, and noncognitive symptoms, combined alternately with mild cognitive impairment, mild neurocognitive disorder, Alzheimer’s disease, vascular cognitive impairment, Lewy body disease, and frontotemporal lobar disease. The authors focused particularly on publications that described NPS in the context of “prodromal,” “preclinical,” “presymptomatic,” or mild cognitive impairment. Mild neurocognitive disorder as described in the DSM-5 is closely aligned to previous definitions of MCI. We categorize findings according to symptom domains within the Neuropsychiatric Inventory. 11 Factor analyses of the Neuropsychiatric Inventory have described symptom clusters that commonly co-occur and may therefore have a common neurobiological basis. 12 We have not included all NPS as this is a brief review and note that symptom clusters may vary according to underlying neuropathology and stage of disease.
Results
Apathy
Apathy is one of the most commonly observed symptoms and has been described in approximately 30% to 40% of individuals with MCI. 4,5 In the Mayo Clinic Study of Aging, apathy was prevalent at baseline in cognitively normal older adults and predicted onset of both amnestic and nonamnestic MCI after a median duration of 5 years. 13 Apathy typically occurs following disruption of circuits linking subregions of the prefrontal cortex and subcortical structures, such as the basal ganglia, implicated in reward processing and complex planning. 14 Clinical definitions of apathy have distinguished between cognitive and emotional aspects of goal-directed behaviour. 15 Atrophy of the anterior cingulate has been associated with reduced initiation while executive dysfunction has been associated with pathology of the dorsolateral prefrontal cortex and reduced reward sensitivity with underactivation of the orbitofrontal cortex. 16 The underlying neuropathology may include AD, Lewy body spectrum disorders, and frontotemporal disease. In fact, apathy is one of the key features of bvFTD and, together with other behavioural or cognitive symptoms, may satisfy criteria for possible bvFTD. 17 Apathy also occurs in the context of vascular cognitive impairment, and it has been associated with “vascular depression” and depression with executive dysfunction. 18,19 It is important to differentiate apathy from depression as apathy may occur independently from depression. In such cases, there is typically a relative absence of distress and negative cognitions so commonly observed in depression.
Apathy in the context of MCI has been associated with accelerated cognitive decline, and its effects can operate independently from depression. In one prospective analysis of patients with MCI, comorbid apathy alone was associated with greater risk of conversion to dementia than comorbid depression. 20 Apathy is associated with a number of adverse consequences, including physical inactivity, functional decline, poor self-care, social isolation, and caregiver distress. 21 Given these adverse consequences, there is increased interest in targeting apathy with arguably more specific treatments. These include neurostimulants, which aim to boost dopaminergic neurotransmission. Methylphenidate is one such agent that has demonstrated promise in the context of AD, and further confirmatory studies are under way. 22 There is some evidence that cholinesterase inhibitors may improve apathy in AD, but the same cognitive and behavioural benefits have not generally been observed in undifferentiated MCI. 23,24 Therapeutic activation and exercise may be helpful in individuals with mild to moderate apathy, although these effects may be diminished or nonexistent in those with severe apathy. 25,26 When apathy occurs in the context of depression, successful treatment of both the motivational and affective aspects of the depressive syndrome will be critical, while in the absence of depression, antidepressants have been found to be largely ineffective. 27 It remains to be determined whether interventions targeting apathy may delay cognitive decline and improve quality of life in the early stages of disease. Interventions to increase cognitive and physical activity have demonstrated promise in at-risk groups, providing a rational basis why apathy should be an important therapeutic target. 28,29
Depression and Anxiety
Depressive and anxiety symptoms have been reported to occur in approximately 40% to 50% of adults with MCI, with some variation according to the population studied and measure used. 4,5 Recent data indicate that depressive symptoms in cognitively normal community-dwelling older adults predict the onset of MCI, while late-life depression in community cohort studies has previously been associated with an approximate 2-fold risk of both AD and vascular dementia. 7,13 In a prospective observational study of 4517 cognitively normal volunteers aged ≥60 years from the National Alzheimer Coordinating Center data set, anxiety and depression were 2 of the most prevalent NPS in symptom clusters, which increased risk of new-onset MCI and dementia independently of baseline cognitive measures. 30 Depression with first onset in later life has been particularly associated with cognitive impairment. 31 In clinic-attending samples of nondemented older adults with depression, approximately 50% have been found to have MCI. 32 In 1 study, almost 25% of older adults presenting with depression and without cognitive impairment at baseline were found to have significant cognitive impairment after 1 year. 33 Cognitive impairment that persists following treatment has been associated with residual depressive symptoms and functional decline. 34 When depression or anxiety co-occurs with MCI, it has been associated with accelerated cognitive decline. 9,35 In certain instances, this effect operates independently of baseline cognitive status, suggesting that depression may independently predict cognitive decline. In others, depression and anxiety increased with increasing severity of cognitive decline, suggesting a bidirectional relationship between cognitive impairment and NPS. 35
Several mechanisms might link depression, anxiety, and cognitive decline. 36 Depression has long been associated with hypercortisolaemia, and recurrent depression has previously been associated with reduced hippocampal volume. 37 Cerebrovascular disease has been particularly associated with depression in later life and may precipitate and perpetuate depression via disruption of corticostriatal tracts necessary for cognitive and emotional regulation. 38 With the advent of molecular neuroimaging, a significant proportion of older adults with depression and MCI has demonstrated increased deposition of beta-amyloid protein, the pathologic hallmark of AD. In animal models, stress and exogenous glucocorticoids have been associated with increased beta-amyloid protein. 39 Increased inflammation, decreased secretion of trophic factors, and increased oxidative stress are mechanisms that may link depression and cognitive decline at a molecular level, while at a behavioural level, physical inactivity and other adverse health behaviours have been associated with accelerated cognitive decline. 40
These observations have therapeutic implications for the treatment of depression and prevention of cognitive decline. First, if neurocognitive impairment so commonly accompanies depression in both younger and older adults, then treatments targeting underlying neuropathological changes may more definitively affect illness severity and course than symptomatic treatments alone. Executive dysfunction has been associated with reduced response to antidepressants in older adults, and persistent functional impairment increases vulnerability to recurrent depressive episodes. 41 Second, effective treatment of depression and anxiety in these early stages may reduce risk of further cognitive decline, thereby disrupting the toxic self-reinforcing cycle of cognitive and functional decline so commonly seen in patients with recurrent depression. Finally, depression is associated with a range of behavioural and physiological risk factors, including physical inactivity, inflammation, and vascular risks, which, if effectively addressed, may help prevent further cognitive decline. 40
Delusions and Hallucinations
The prevalence of psychosis in MCI is 3% to 14%. 5 Psychosis is more common in dementia and is seen in one-third of patients with a major neurocognitive disorder due to AD 42 and 50% of those due to Lewy body or Parkinson disease. 43 The presence of psychosis raises the possibility of neurodegenerative disease, but other conditions, such as delirium and primary psychiatric illnesses, such as delusional disorder or late-onset schizophrenia, must also be considered. The emergence of psychosis in late life, including transient psychosis, is associated with an 8 to 11 times increased risk of conversion to dementia. 44
While psychosis may be observed in patients with MCI, it occurs with much greater frequency in established dementia. This is in contrast to other neuropsychiatric symptoms, such as apathy and depression, which may occur in MCI. Thus, much of what we know about dementia and psychosis has been derived from studies of patients with established dementia. In dementia, psychotic symptoms tend to be simplistic and revolve around certain themes. 45 Delusions tend to be either persecutory (such as the delusions of theft) or related to misidentification. 46 Psychotic symptoms in some cases may be hard to differentiate from other cognitive symptoms such as disorientation or confabulation. Such cognitive symptoms tend to fluctuate while psychotic symptoms are often fixed. Delusions tend to precede the development of hallucinations, which are usually a marker of more advanced disease and are more commonly visual in nature. 47 One notable exception is the visual hallucinations observed in patients with Lewy body disease. These visual hallucinations can occur early in the course of the disease, are often very vivid, and are associated with significant distress. 48,49 Similarly, visual hallucinations are a risk factor for cognitive decline in patients with Parkinson disease and MCI. 50
The etiopathology of psychotic symptoms in neurocognitive disorders remains unclear. Numerous imaging studies have suggested that psychotic symptoms in AD tend to be associated with grey matter volume loss in the frontal lobes, 51 –54 and there is some suggestion that the findings may be more prominent on the right. 51,53 There is evidence that psychosis in AD may be heritable as rates of psychosis double from 30% to 60% when examining relatives of AD patients with psychosis. 55 There is also some evidence to suggest an association with APOE4, although other studies have proven negative. 56 There is putative evidence for linkage with nicotinic receptor and serotonin transporter genes. 56 Neuropathologic findings are variable, with some studies showing a strong correlation between psychosis and Alzheimer load 57 –59 and other studies showing no such association. 60 –62 Fischer et al. 62 recently demonstrated a link between cardiovascular risk factors, cerebrovascular disease, and onset of psychosis in AD, suggesting a potential preventive strategy. Finally, visual hallucinations have been demonstrated to be associated with a more marked cholinergic deficit based on their prominence in Lewy body disease 63 and their response to cholinesterase inhibitors in this and related conditions. 64 While the evidence is modest, Cummings et al. 64 conducted a secondary analyses of a 3-phase study examining the effectiveness of donepezil in AD patients with moderate to severe behavioural symptoms, noting a significant improvement in the NPI psychosis subscore.
Patients with dementia and psychosis have worse outcomes in terms of functional impairment, 65 disease progression, 66,67 cognitive impairment, 68 aggression, 69 institutionalization, and caregiver burden. 70 Despite the association of psychosis with worse clinical outcomes and the increased risk of conversion to dementia, there are no data as yet to suggest that early treatment of psychosis with antipsychotic medication delays cognitive decline. In fact, the use of antipsychotic medication has been associated with greater cognitive decline, and adverse effects limit their use to circumstances where there is significant distress or increased risk to the patient and others. 71
Agitation and Disinhibition
Agitation is often an expression of emotional distress and may manifest itself in excessive motor activity or verbal or physical aggression. 72 Variability in the definition and assessment of agitation results in a wide range of prevalence, from 4% to 35% of individuals diagnosed with MCI. 5 Nonetheless, agitated behaviours are a risk factor for both incident MCI 13 and progression from MCI to dementia. 30 Agitation has been linked to structural and functional changes in the frontal cortex, amygdala, and anterior cingulate cortex and can be thought of as a deficit in the ability to appraise threat and regulate fear and affect. 73 Disinhibition has been associated with degradation of fronto-subcortical circuits critical to appraisal of risk and social judgement. This can occur with several pathologies, including AD and cerebrovascular disease, but has been particularly associated with bvFTD. 17
Prospective, longitudinal studies of populations genetically at risk for neurodegenerative conditions, such as those with autosomal dominant mutations, have provided some insight into changes in behaviour that can precede the onset of cognitive decline. One example is the Dominantly Inherited Alzheimer’s Network study, which found that mutation carriers with very mild or questionable symptoms of cognitive decline, on average 5 years before expected onset of a major neurocognitive disorder, had changes in behaviour, including increased agitation, disinhibition, and irritability. 74 This study did not find any behavioural changes in mutation carriers without cognitive symptoms, although this group was substantially younger (on average 13 years before expected onset of dementia), and the measures used may not have been sufficiently sensitive to detect subtle changes.
Changes in behaviour are a key feature of bvFTD. The diagnostic criteria include symptoms of social disinhibition, apathy, loss of empathy, perseverative or ritualistic behaviours, and hyperorality that may precede the onset of cognitive decline. 17 The Genetic Frontotemporal Dementia Initiative, which has been following families with autosomal dominant mutations for frontotemporal lobar degeneration, found that mutation carriers showed more behavioural symptoms than noncarriers 5 years prior to predicted onset of disease. 75 Older adults who exhibit clinically significant behavioural changes without cognitive symptoms have an increased risk of progressing to nonamnestic MCI. 13 They are also at risk of bvFTD, with more than two-thirds developing this disorder within 5 years of follow-up. 76
Nonpharmacological interventions such as addressing unmet needs and modifying environmental triggers may be helpful in the management of agitated behaviours and disinhibition in MCI. Cholinesterase inhibitors have not been demonstrated to have a meaningful impact on agitation in AD, and their impact on NPS in MCI has not been well studied. 77 Antidepressants have some efficacy in reducing agitation in dementia but have similarly not been well studied for NPS in MCI. 78 In circumstances where there is a risk to the individual or others, antipsychotic medications have demonstrated efficacy in dementia. However, the associated morbidity and risk of cognitive decline with these medications must be weighed against the potential benefits.
Discussion
Recent studies indicate that NPS not only are prevalent in MCI and the early stages of cognitive decline but in many instances precede the onset of identifiable neurocognitive changes. 4,13 The co-occurrence of NPS with MCI has been associated with more accelerated cognitive decline in several studies. 10,67 In this regard, NPS may be considered integral manifestations of neurocognitive disorders that can facilitate early diagnosis and serve as useful prognostic indicators. The mechanisms of association may include 1) NPS arising secondary to degradation of neuronal tracts implicated in reasoning, perception, motivation, or affective regulation; 2) NPS as risk factors that promote the development of the neurodegenerative disease; 3) NPS occurring as a psychological reaction to losses arising from neurodegenerative disease; and 4) NPS co-occurring with neurocognitive disorders due to shared risk factors.
In view of the observation that NPS may precede cognitive decline, researchers have recently described an emerging term, mild behavioural impairment (MBI), which is defined as a behavioural syndrome arising for the first time in later life in the absence of dementia or another definable psychiatric disorder. 76 This may be considered the behavioural counterpart of MCI, and in one longitudinal study of patients with either MBI or MCI, MBI was associated with greater risk of developing dementia, supporting the proposition that it represents a transitional state between normal ageing and dementia. 76 The NPS professional interest group of the International Society to Advance Alzheimer’s Research and Treatment (ISTAART) has recently proposed provisional diagnostic criteria for MBI. 79 The criteria require at least minimal impairment in social, occupational, or interpersonal function secondary to changes in behaviour or personality, rather than cognitive decline, starting in later life (age ≥50 years) and persisting at least intermittently for ≥6 months to help distinguish it from an adjustment disorder. The changes cannot be attributable to another psychiatric disorder, and the patient cannot meet criteria for dementia or major neurocognitive disorder, although MCI may coexist. The authors acknowledge that these criteria will require validation and refinement over time with the expectation that they should facilitate earlier detection and treatment of neurodegenerative disease. 79
The clinical implications for all practicing clinicians are that a persistent change in behaviour or personality emerging for the first time in later life should increase suspicion for an underlying neurocognitive disorder. This should trigger further neuropsychological evaluation and careful collateral history to detect recent changes in cognition, function, or behaviour. Behavioural changes in later life may, of course, have a contextual or primarily psychiatric etiology, but serial neuropsychological evaluations should help to detect the emergence of a neurocognitive disorder at the earliest opportunity. Neuroimaging and investigation of underlying modifiable risk factors should be considered when necessary. The therapeutic approach will then necessarily address the underlying neuropathology as well as the symptomatic manifestations. General considerations include minimizing the use of anticholinergic or other medications known to exacerbate cognitive function and use of psychotherapeutic interventions that have been adapted to individuals with MCI and early dementia. 80 Certain psychotropic medications may be more effective than others in addressing cognitive changes associated with depression or other neuropsychiatric disorders, and this is an area for further investigation. 81 Multicomponent interventions that address vascular risks and physical and cognitive inactivity in older adults at risk of further cognitive decline have demonstrated promise and may be particularly applicable to patients with psychiatric comorbidity. 82 Finally, novel modifying approaches, which target the underlying neuropathological changes, hold the potential to delay disease progression, and studies in the early clinical and preclinical stages of disease are currently under way. 2 A suggested initial management approach to older adults with new-onset persistent changes in personality, behaviour, or cognition is outlined in Figure 1.
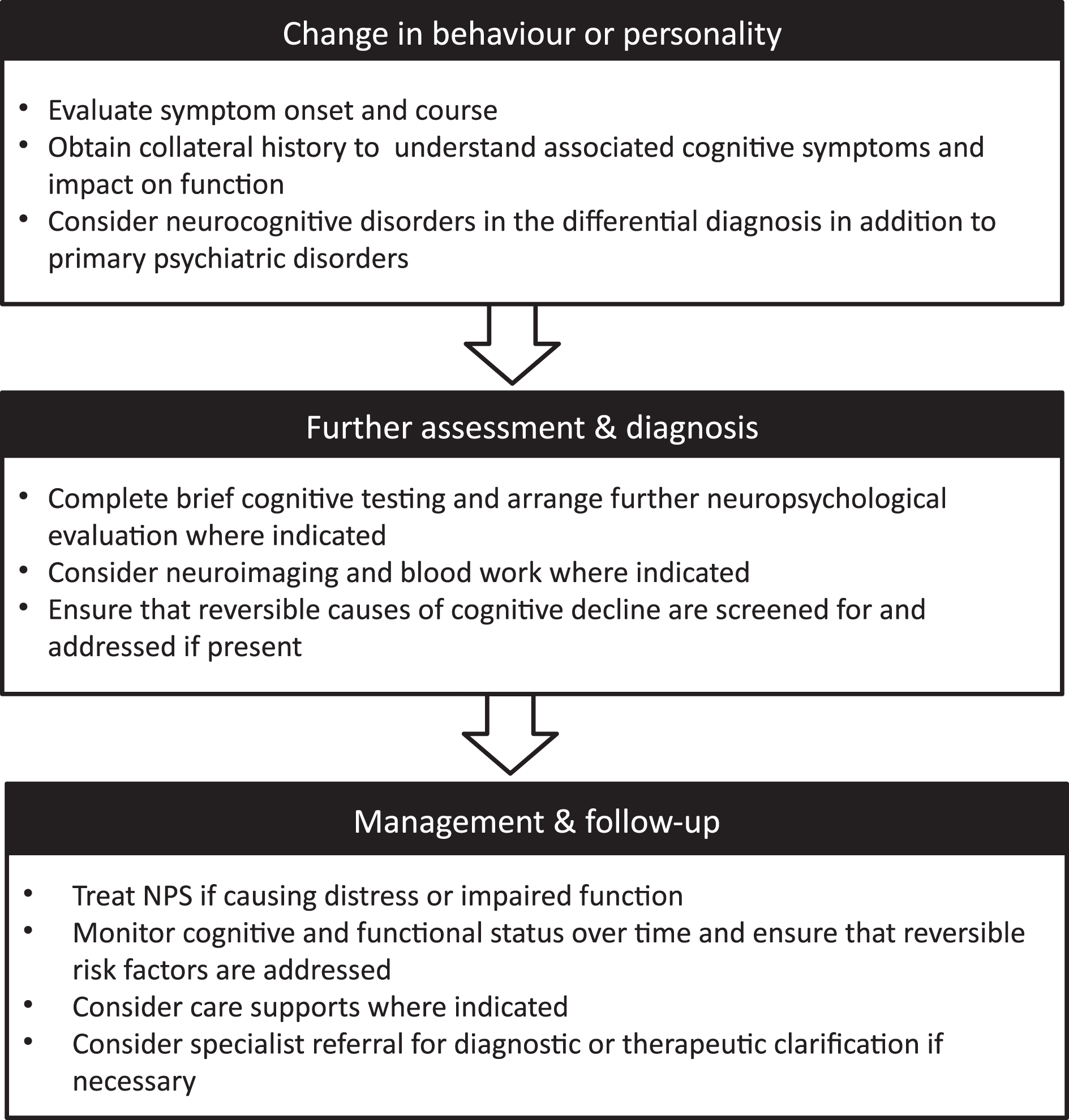
Suggested initial management approach for older adults with new changes in behaviour or personality. NPS, neuropsychiatric symptoms.
The repeated observation that individuals with NPS are at increased risk of further cognitive decline delineates this group as high risk and suitable for early interventions to prevent cognitive and functional loss. Effective treatment of NPS in the early stages of cognitive decline will be important for quality of life but may also help stabilize cognitive and functional status. In major depression, effective treatment may, in the short term at least, result in partial, if not complete, improvement in cognitive function and certain behavioural and physiological risk factors, such as physical inactivity or inflammation. 83,84 What is less clear is whether addressing milder symptoms of anxiety, apathy, or depression, which are clinically significant and potentially amenable to nonpharmacological or behavioural intervention, may reduce risk of cognitive decline or prevent development of more significant psychiatric syndromes driven by deteriorating cognitive function.
Conclusion
In conclusion, NPS are prevalent in MCI and may be the first symptom of an underlying neurocognitive disorder presenting even before onset of measurable cognitive decline. Increased awareness and appropriate evaluation of patients presenting with behavioural symptoms for the first time in later life should facilitate earlier detection of neurocognitive disorders. Future studies will determine whether effective treatment of NPS in these early stages may both relieve distress and modify the disease course. Early diagnosis will become increasingly important as we move towards preventive interventions designed to delay cognitive and functional decline and which may be most effective when deployed in the earliest stages of disease.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.