
Abstract
Objective:
Depression is usually treated with antidepressants, psychotherapy, or both. In this study, we examined the extent to which individuals with depression receive minimally adequate treatment with regard to the use of antidepressants and psychotherapy.
Method:
Using population-based administrative data, we identified individuals with inpatient or outpatient diagnoses of depression and tracked their use of publicly funded mental health services within a 12-month period. We used mixed-effects logistic regression to assess the influence of patient-level characteristics and physician-level variations on the receipt of minimally adequate treatment.
Results:
A total of 108 101 individuals, predominantly women (65%) and urban residents (89%), were diagnosed with depression in 2010–2011. Of these, 13% received minimally adequate counseling/psychotherapy with higher proportions observed among men, younger individuals, and urban residents. In contrast, there were more who received minimally adequate antidepressant therapy (48%), with women, older individuals, and rural residents having the highest proportions. Overall, about 53% received either type of treatment, and the pattern of use was similar to that of antidepressant therapy. Mixed-effects logistic regression results indicate that these factors remain independent predictors of the receipt of minimally adequate depression care. Significant practice variations also exist, which determine patients’ receipt of minimally adequate care, particularly with respect to counseling or psychotherapy.
Conclusions:
Only about half of those with depression receive either minimally adequate counseling/psychotherapy or minimally adequate antidepressant therapy. Disparities also persist, affecting mostly men and younger individuals. A multifactorial approach is needed to improve access to and reduce variations in receipt of minimally adequate depression care.
Clinical Implications
Existing structures, policies, and practices need to be evaluated to further understand why almost half of the individuals diagnosed with depression do not receive minimally adequate treatment.
Additional supports and alternative modes of accessing depression treatment are needed for younger individuals who are most at risk of not receiving minimally adequate care.
Practice variations need to be reduced to minimize their impact on patients’ odds of receiving minimally adequate treatment for depression.
Limitations
Services that are not publicly covered were not included in the analyses. Study results may have understated income-related disparities. Use of antidepressant therapy was examined using prescription fills; study results may have underestimated prescribing practices and overestimated actual use.
One in 20 individuals, each year, experience major depressive disorders (MDDs). 1,2 Many remain untreated, even though evidence-based treatments, such as psychological and antidepressant therapies, 3,4 exist. Contrary to popular belief, most of those with depression actually receive treatment exclusively from general practitioners (GPs). 5
Estimates of the percentage of people with untreated depression vary widely, ranging from 16% to 84% (median, 56%). 6 The treatment gap is high even in largely developed regions such as Europe (45%) and the Americas (57%). 6 In Canada, analysis of recent data indicates that 28% (95% CI 24% to 32%) of the population with probable MDD self-reported not receiving any help for their condition. 7 The gap increases to 37% (95% CI 33% to 41%) if we count only those with probable MDD who self-reported not receiving mental health care from hospitals or other health care professionals such as psychiatrists, GPs, psychologists, nurses, social workers, and counselors. 7
Some of the treatment gap is due to personal circumstances, such as not knowing how to get help or not having confidence in the health care system, and to health system factors, such as services being unavailable or inaccessible. 8 There are individuals, however, who overcome these challenges and manage to put their feet within the door of the formal health care system, only to contend with another issue—poor or undertreatment by any published standard.
Studies in North America 9 –21 suggest that 30% to 79% (median, 52%) of individuals with MDD or mood disorders who undergo treatment receive treatment that does not meet the minimum threshold for adequacy. In Europe, recent studies 22 –28 estimate the proportion of those who receive poor treatment to be between 24% and 75% (median, 60%).
The variation in these estimates is likely due to differences in definitions, population characteristics, sample size, and methods. Despite the variations, however, the overall evidence still highlights that a large number of people receive inadequate treatment for depression. Addressing this gap is important, given the huge societal impact of mental illness 29 in general and MDD in particular. Most importantly, closing the gap will improve patient outcomes. 30,31
An essential step toward addressing the gap is understanding its magnitude. Canada, in this respect, does not appear to be at par with other developed countries. At the time of writing, we are aware of only 2 published studies that quantified the extent of the gap; one based on data from a 2002 national survey 14 and another based on a more recent provincial survey. 19 Both used self-reported data, which are susceptible to social desirability 32 and recall biases. 33 Studies comparing survey and administrative data show that self-reported data substantially undercount people with mental health conditions 34 while at the same time overcount the frequency of health care use, 35 particularly among individuals experiencing severe symptoms. 36,37
In this population-based data linkage study, we aim to contribute to the current understanding of the gaps and disparities in depression care in publicly funded health systems. Specifically, we address the following questions: How often do individuals receive minimally adequate care for MDD? Does receipt of minimally adequate care for depression differ by variables such as age, sex, income, geographic location, and practising physicians?
Methods
Data Sources
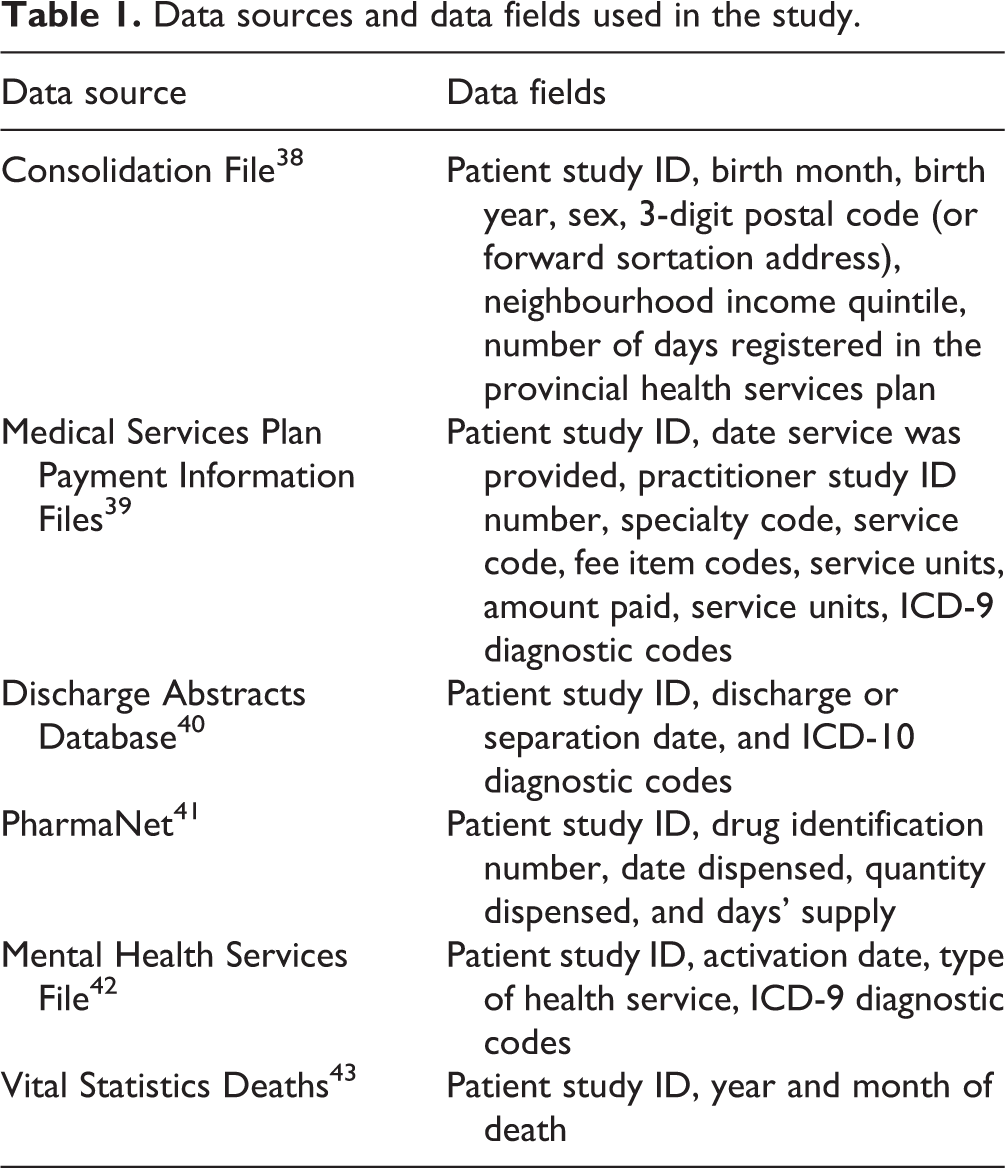
We examined individual-level health administrative data from virtually everyone in the province of British Columbia (BC). Anonymized data were extracted from multiple databases (Table 1) linked by unique study identifiers.
Data sources and data fields used in the study.
The BC Ministry of Health, Data Stewardship Committee, and Vital Statistics Agency granted data access permissions. The University of British Columbia Behavioral Research Ethics Board provided ethics approval.
Study Cohort
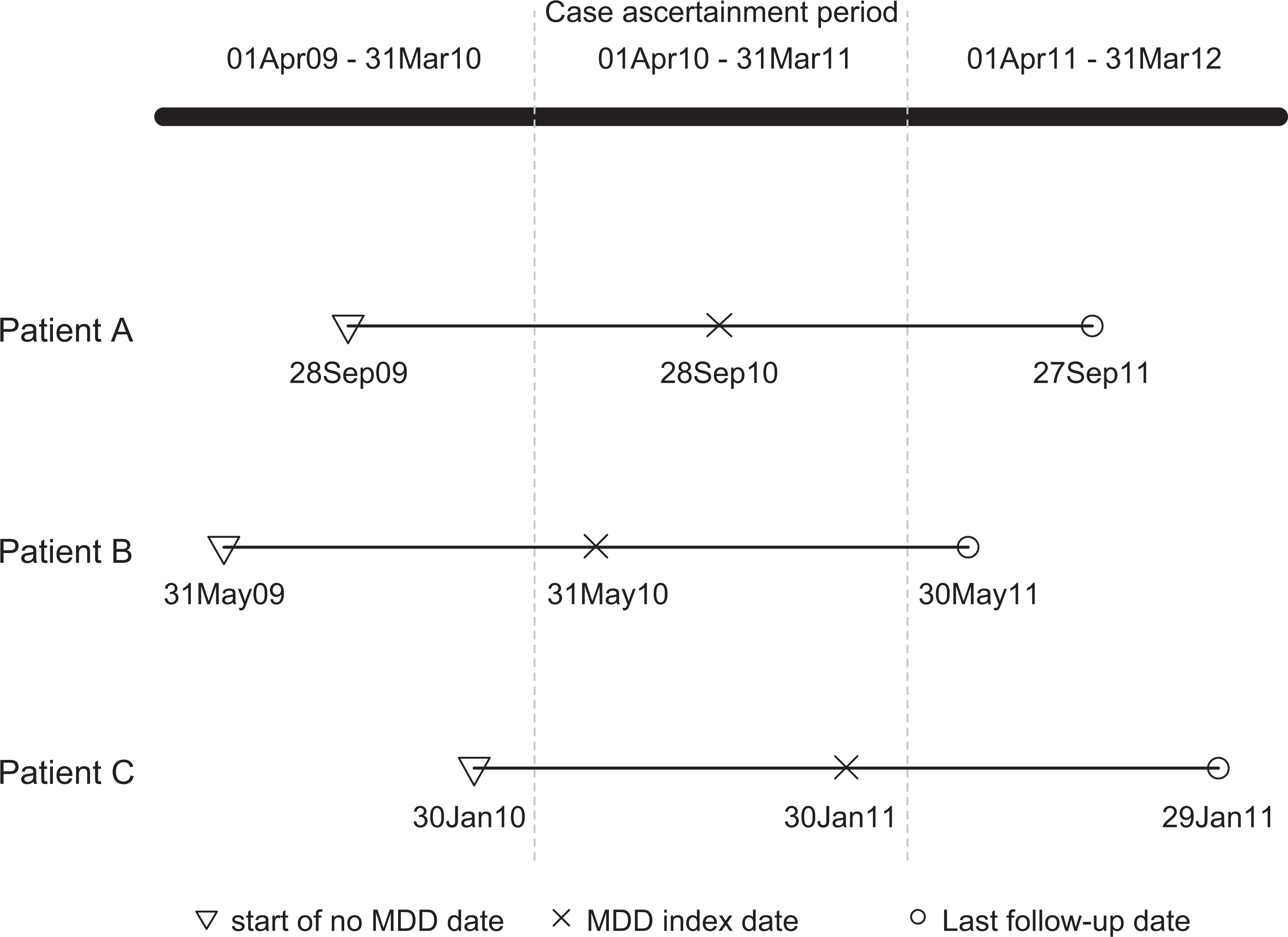
We examined data from 3 fiscal years (FYs) to ensure that each individual in our cohort had 12 months of health service history and 12 months of follow-up. We ascertained cases in FY2010/11 and used FY2009/10 and FY2011/12 as look-back and follow-up periods. This configuration enabled us to determine whether those first diagnosed on 31 May 2010, for example, had a 12-month history (31 May 2009 to 30 May 2010) of any of the diagnoses listed in our exclusion criteria and also if they received treatment within 12 months (31 May 2010 to 30 May 2011) following initial diagnosis (Figure 1).
Timeline for cohort selection and follow-up.
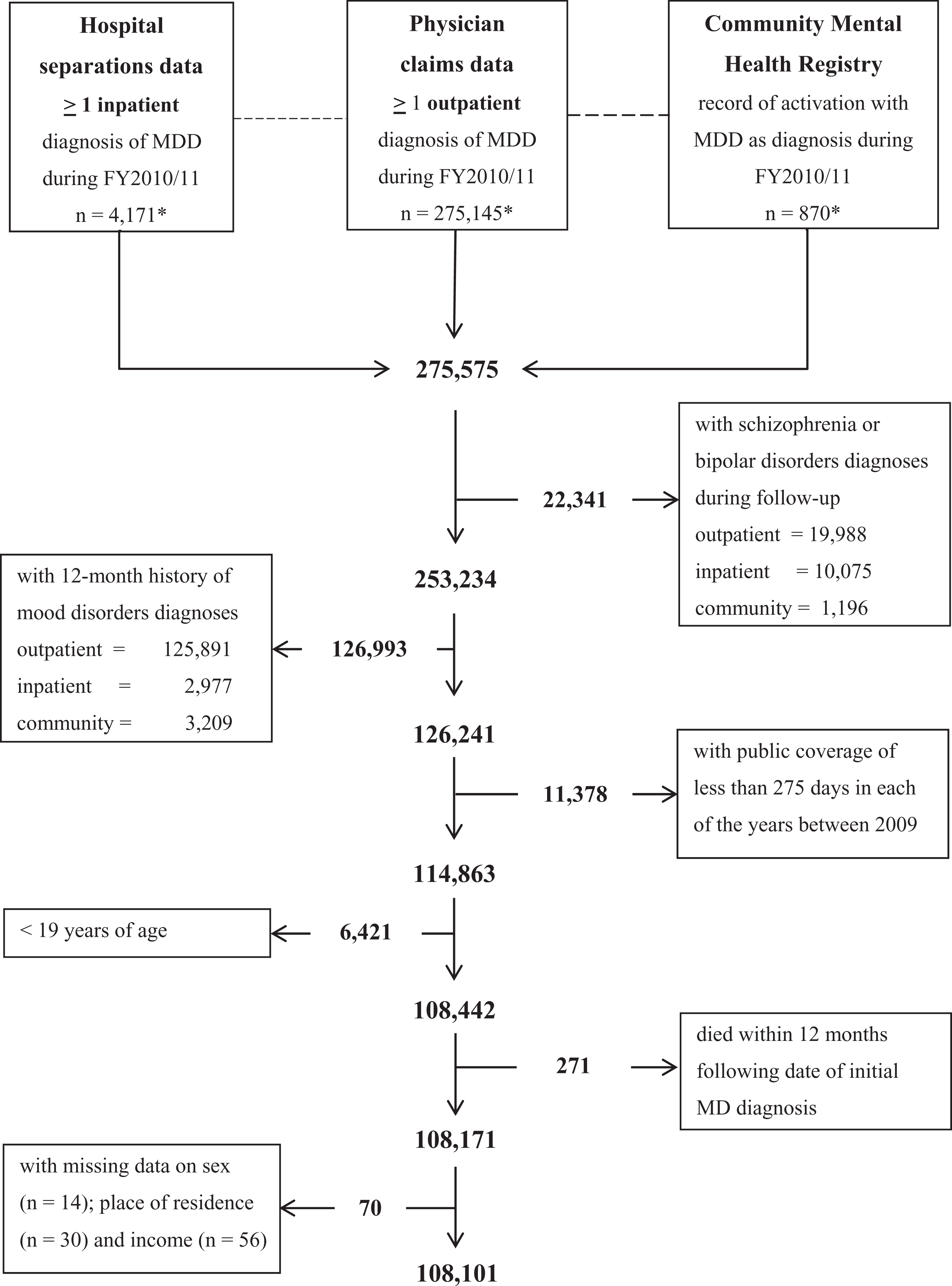
To identify study cohort members, we first extracted records of individuals with MDD (ICD-9 296, 296.2, 296.3, and 311 and ICD-10 F32, F33, and F39) from physician claims, hospital separations, and community mental health service data files in FY2010/11. We considered only the most responsible diagnosis. When individuals showed up in more than one database, we retrieved the earliest record and marked that as the index date. We removed those with diagnoses of schizophrenia or bipolar disorders (ICD-9 295 and 296.4 to 296.7, ICD-10 F25 and F29 to F31) between FY2009/10 and 2011/12.
As we were interested only in individuals who initiated treatment during FY2010/11, we excluded those who had a 12-month history of any mood disorder diagnoses (ICD-9 296 and 311 and code 50B, ICD-10 F3x). In addition, we ensured that the cohort consisted only of those eligible to receive publicly funded health services by removing anyone with yearly registration in the provincial health services plan of less than 275 days between 2009 and 2011. Last, we excluded those who were younger than 19 years, died during the 12-month follow-up, or had missing data on sex, place of residence, and income (Figure 2).
Cohort. *Count of individuals who have a recorded diagnosis of depression (multiple listings are possible) in physician claims, hospital data, and community mental health treatment registries during fiscal year 2010/11.
The use of algorithms based on ICD9/10 diagnoses for MDD case detection is common in health administrative data analyses. 44 In our study, we used diagnostic codes similar to those used by a Canadian surveillance system, 45 which shows good validity (sensitivity, 81.1%; specificity, 94.8%; positive predictive value, 79.6%; negative predictive value, 95.2%) based on validation work conducted in several Canadian provinces. 46 Analysis of BC data from the validation study 46 yielded comparable validity indices. 47
Outcome Measures
We constructed indicators to measure minimally adequate counseling/psychotherapy (MACP), minimally adequate antidepressant therapy (MAAT), and minimally adequate treatment.
MACP assesses receipt of ≥4 counseling or psychotherapy sessions in individual or group settings. The cutpoint was adapted from similar studies that analyzed administrative databases 15,48 and reflects a realistic threshold in BC, where the publicly funded health system easily allows up to 4 counseling claims per patient, annually. 49 Only paid claims specifically designated as counseling or psychotherapy, regardless of duration, were counted in creating MACP.
MAAT measures whether antidepressant prescriptions were filled with ≥84 supply days. We used the World Health Organization’s Anatomical Therapeutic Chemical classification code (N06Axxx) to identify antidepressant fills. The cutpoint was adapted from previous studies 15,48 and corresponds to the 12-week acute treatment phase 50 during which individuals initiating antidepressant therapy are expected to be on medication. Because the 84-day period is covered in many cases by single fills (such as a prescription for 90 days), MAAT was created by counting only the supply days, which is considered sufficient for investigating medication use in shorter time frames. 51
The last indicator measures receipt of either MACP or MAAT.
These indicators were previously examined within the acute treatment period. 15,48 In our study, we used a 12-month period to capture services that take longer to access in BC (such as publicly covered psychotherapy/counseling).
Explanatory Variables
Our explanatory variables include age, sex, income, and place of residence. As more recent household-level income data are not available, we used Statistics Canada’s neighbourhood income quintiles. We coded the patient’s place of residence as rural if the second character of their postal code was zero and urban for everyone else.
We created aggregated diagnostic groups (ADGs) following the Johns Hopkins adjusted clinical groups case-mix system. 52 We used counts of major ADGs (mADGs) as a measure of health status, with higher counts signifying greater morbidity and clinical complexity. 52
Because BC does not have a formal rostering of patients with physicians, we adapted a method of linking individual patients to a major source of care (MSOC). 53 First, patients were assigned to physicians who charged the annual mental health planning (MHP) fee code. When MHP was claimed more than once in a year, we assigned the patient to the physician with the earliest MHP claim. Then, we designated as MSOCs those physicians who were visited exclusively by patients during follow-up. Failing these 2 approaches, we assigned patients to physicians who provided at least two-thirds of the follow-up care. The remaining patients who could not be assigned were given the same 5-digit MSOC number.
Statistical Analysis
We used descriptive statistics to summarize the cohort’s characteristics. We also provided counts and proportions for the 3 indicators (MACP, MAAT, minimally adequate treatment), broken down by demographic and clinical characteristics. To determine if the indicators were associated with the explanatory variables and physician-level variations, we ran mixed-effects logistic regression, with patient demographic and clinical characteristics entered as fixed factors and physician study identifiers as random effects. We used the adjusted odds ratios from the models as measures of the magnitude of association between the indicators and explanatory variables. Physician-level variations, on the other hand, were quantified using intracluster correlation coefficients (ICC). Higher ICCs were interpreted as indicative of greater physician variations. We also calculated median odds ratios (MORs) to complement the ICCs, which have a limited interpretation in a mixed-effects logistic regression. 54 In the context of our study, MOR refers to the median of the distribution of all ORs formed when a physician with higher odds is compared with another who has lower odds of providing care. When the odds of providing care vary substantially across physicians, the OR distribution will be wider and its median further from the value of 1. An MOR = 1 could thus mean that all physicians are equally likely to provide a particular type of service, whereas an MOR >1 implies that some physicians are more likely than other physicians to provide a specific type of care. This intuitive interpretation of the MOR along with its being in the same scale as the other model ORs facilitates comparison of the various factors that influence receipt of minimally adequate care. Further details on the MOR can be found elsewhere. 55
We used SAS/SQL software V 9.4 to link and manage multiple databases. We used xtmixed (with 30 integration points) and xtmrho routines running under Stata Version 13.1 to generate the model results.
Results
The number of individuals who received treatment for mood disorders in FY2010/11 was 275 575, representing 6% of the total population in BC, based on a 2011 population estimate of 4 576 000. 56 The majority of these individuals received mental health care only from GPs (77%). The rest visited psychiatrists exclusively (8%), GPs or specialists (including psychiatrists; 14.5%), and other specialists (excluding psychiatrists; 0.5%).
The final cohort included 108 101 individuals, representing 3% of the BC population who were older than 19 years in 2011. These individuals who initiated some form of treatment for depression in 2011 were predominantly women between the ages of 36 and 55 years (41%) and urban residents. Higher concentrations were found in the lower income groups, particularly in the lowest quintile.
Close to half of the cohort members had no mADGs, while a smaller proportion had 3 or more mADGs. Less than 1% (n = 1003) were hospitalized with a mental health reason as the most responsible diagnosis. About 57.7% received ≥1 counseling/psychotherapy session, 58.4% filled ≥1 antidepressant prescription, and up to 82.5% received either treatment.
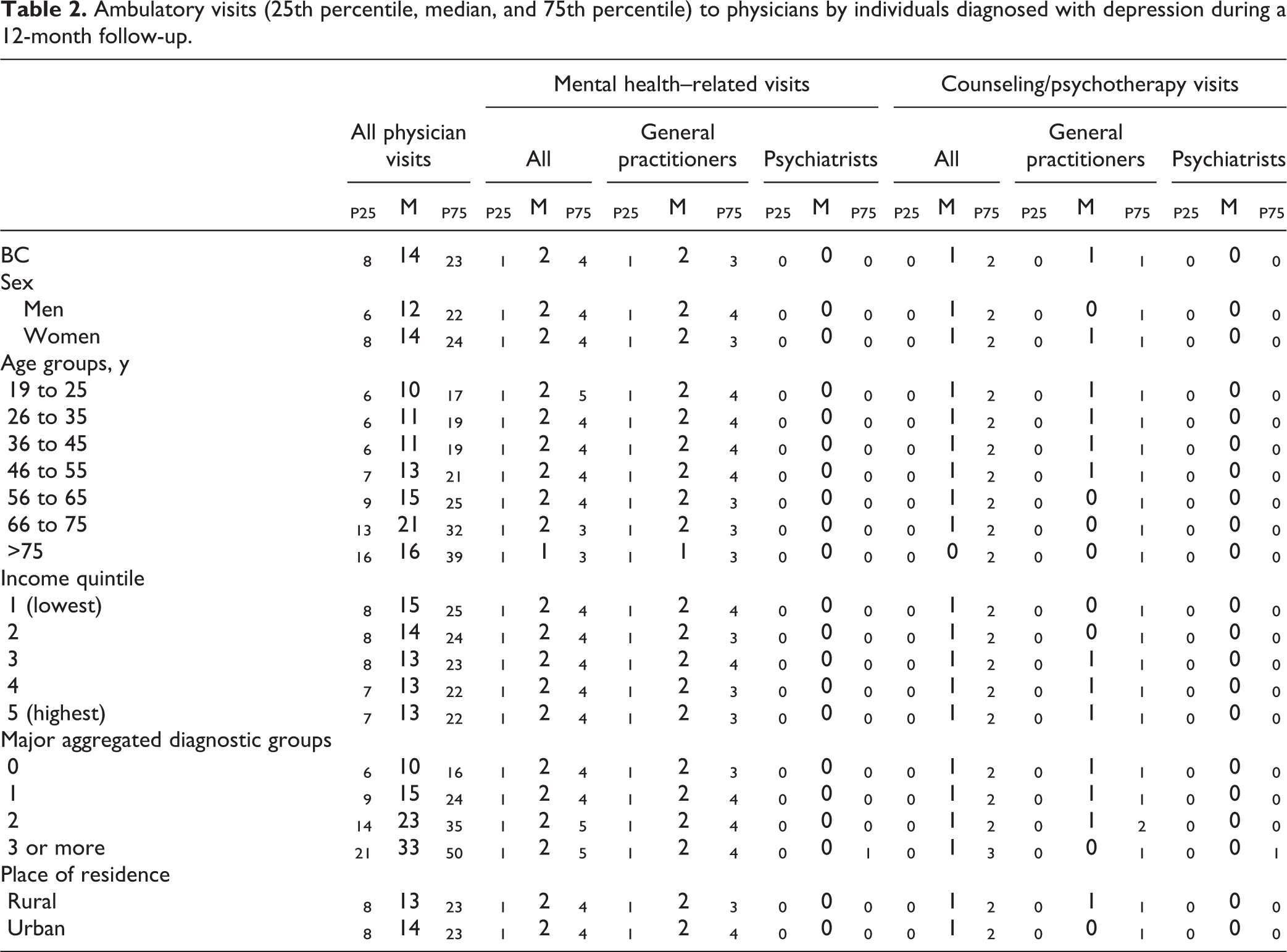
The median number of mental health–related physician visits was 2, and they were mostly visits to GPs; the majority (P75) had no psychiatry visits. The median number of counseling/psychotherapy visits was 1, provided mostly by GPs; the majority (P75) had no counseling/psychotherapy visits to psychiatrists (Table 2).
Ambulatory visits (25th percentile, median, and 75th percentile) to physicians by individuals diagnosed with depression during a 12-month follow-up.
MACP
A small percentage (13%) of the cohort received MACP. Differences by sex, age, residence, and health status were present and persisted even after adjustment for other factors in a multivariable regression model. Men had slightly higher odds than women of receiving MACP. Individuals between the ages of 19 and 35 years had greater odds of receiving MACP compared with older adults (46–55 years), whose odds were considerably greater than those older than 75 years. Rural residents had lower odds of MACP than those living in urban areas. Patients with higher mADG counts had greater odds of receiving MACP.
The provision of MACP appeared to vary substantially by physicians. Model results suggest that about 33% of the variation that cannot be explained by any of the fixed factors were due to practice variations. The MOR also indicates that some physicians had about 3 times the odds of other physicians (MOR = 3.36) in providing MACP. Furthermore, MOR suggests that the odds of receiving MACP was contingent more on which physicians were visited than on patient characteristics such as age, sex, and so forth.
MAAT
A little less than half of the cohort (48%) received MAAT. Differences by sociodemographic and health factors were present (Table 3), which also persisted even after adjusting for other factors in a multivariable regression model. Men seemed less likely than women to receive MAAT. Individuals between the ages of 19 and 35 years had substantially lower odds than older adults (46 years and older). Rural residents had higher odds of receiving MAAT than those living in urban areas, and patients with greater mADGs had greater odds of receiving MAAT. The residual variation that could be attributed to variations in physician practice was remarkably lower (9%) than that observed for MACP.
Treatment adequacy for depression: prevalence (%) and adjusted odds ratio (AOR).
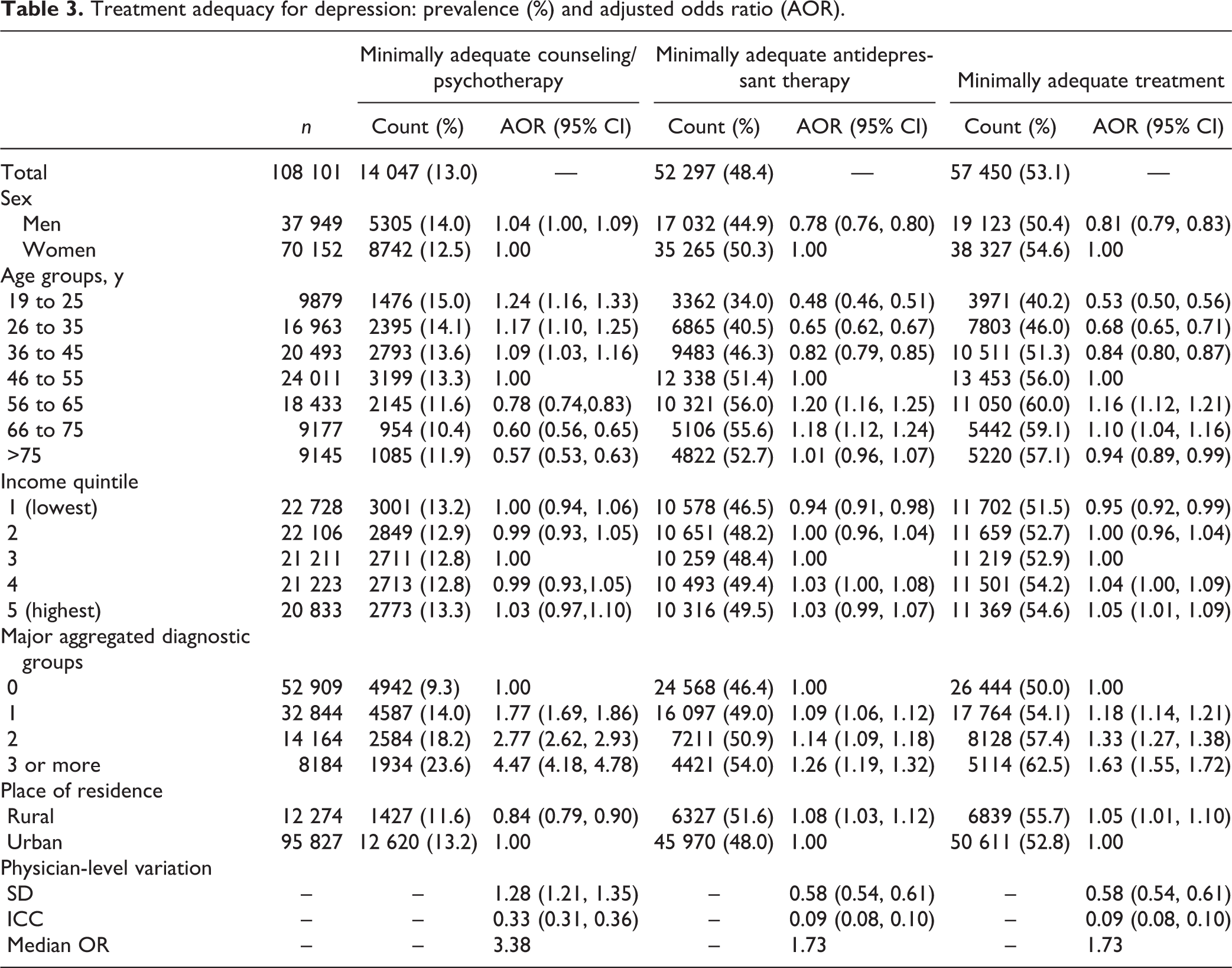
Minimally Adequate Treatment
A little more than half (53%) of the cohort received minimally adequate treatment. Higher proportions were observed in women, older individuals, higher income quintiles, and residents of rural areas (Table 3). These differences remained even after adjusting for other factors in a multivariable model. The odds of receiving minimally adequate treatment were lower in men than women. Individuals between the ages of 19 and 35 years had lower odds than older adults. The odds for patients in the lowest income quintile were lower than the odds for patients in the third quintile, whose odds, in turn, were lower than patients in the highest income quintile. The residual variation in the receipt of minimally adequate treatment that could be attributed to physician practice variations was similar to that of MAAT.
Discussion
We conducted a population-based, data linkage study to determine how often individuals diagnosed with MDD receive minimally adequate care and to measure disparities associated with various factors. We found that about half of the individuals diagnosed with depression receive minimally adequate care, mostly in the form of antidepressant therapy. Furthermore, whether patients receive these services depends, to varying degrees, on their sex, age, income level, health status, hospitalization for mental health reasons, place of residence, and the specific physicians they visit to seek care.
Our finding that 53% receive minimally adequate depression care appears low compared with a US study that reported a proportion of up 70% in a Medicaid-enrolled population. 15 The proportion of individuals who receive MACP (13%) in our study is also surprisingly low compared with 62% who receive similar care found in the US study. 15 However, our study found a higher proportion of individuals who receive MAAT (48% compared with 29.5% in the US study).
These contrasting numbers are explained partly by some methodological differences between our study and the US study. 15 For example, we used a 12-month period for ascertaining cases and for follow-up compared with 12-week look-back and 144-day follow-up periods used in the US study. We used population-based data in BC, where depression treatment is provided mostly in primary care, whereas the US study examined Medicaid-enrollees receiving treatment in mental health specialty care settings, where the frequency of receiving minimally adequate treatment tends to be high. 12 Our cohort also has fewer individuals who were hospitalized for mental health reasons (0.93% compared with 15.7% in the US study). It is unlikely, nevertheless, that the marked differences in the levels of use are entirely due to methodological differences.
Indeed, similar levels of minimally adequate depression care have been reported in at least 1 Canadian province. A Quebec study, 57 for instance, found that up to 13% of its survey respondents meeting criteria for MDD receive MACP. In addition, the study reported that 46% of its respondents receive MAAT and that 52% receive either type of treatment. We note, however, that the Quebec study defined MACP as receipt of ≥12 consultations for mental health reasons in the previous year plus ≥1 recommended psychotherapy and MAAT as receipt of ≥1 prescription for antidepressants plus ≥3 medical visits.
It is also worth noting that the minimally adequate depression care received by the majority in our cohort is mainly through antidepressant therapy. Several reasons could account for this. First, most individuals with depression receive treatment in primary care, where antidepressant therapy is more available and appears to be the treatment of choice. 58 Second, services provided by physicians constitute the majority, if not all, of the publicly funded counseling/psychotherapy services, and accessing these services is challenging because of significant wait times. 59 Third, some fee-for-service physicians are predisposed to regard the dispensation of antidepressants as an opportunity to reduce time spent on patient counseling 60 and consequently increase the number of billable visits. BC instituted policies in 2008 to curb this propensity through financial incentives. 61 However, we are not aware of any studies, to date, that demonstrate its impact on the provision of counseling/psychotherapy.
Another notable finding is the lower odds of receiving minimally adequate treatment overall among younger individuals. This disparity, in addition to the large gap in minimally adequate care, underscores the need to enhance access to counseling/psychotherapy or other forms of treatment for this age group. Given existing concerns about the lack of efficacy of and the adverse events linked to antidepressant therapy in the younger population, 62 it is difficult to discuss the expanded role antidepressants could have in addressing the considerable gap and disparity in treatment adequacy.
We also would like to highlight results that indicate the presence of substantial practice variations in the provision of MACP. Much of these variations could be explained by differences between mental health specialists and family physicians in the inclination and ability to deliver these services. It could also be due to differences in familiarity with treatment algorithms for depression and amount of practice time devoted to mental health. 63 Notwithstanding all of these potential sources of variation, our results highlight the need for a higher level of consistency in providing these services since most patients with depression receive treatment from physicians and certain types of brief psychological therapies are known to be effective in primary care settings. 64 –66
Finally, our 6% estimate of the treated prevalence of mood disorders is slightly higher than the national estimate of 5.4% (95% CI 4.9 to 5.8). 1 This is partly because our estimate is based on the entire population, unlike the national survey, which drew samples from individuals who are at least 15 years of age. The slight discrepancy could also be due to physician coding error in the claims database or to residual social desirability bias 32 in the survey. 34
Our study adds to the body of knowledge on minimally adequate care for depression, especially in Canada where evidence is scarce. Our data sources do not share the same weaknesses as self-reported data, and as such, our results complement findings from existing literature currently dominated by survey studies. Like other studies, nevertheless, some limitations need to be kept in mind when considering our results.
First, case identification was done through ICD-9/10 codes, which, although accurate, are still associated with misclassification errors. 47 Second, we were unable to examine the appropriateness of counseling/psychotherapy provided by physicians as our data do not allow us to classify the type of counseling/psychotherapy provided. Third, we were unable to track counseling/psychotherapy services that are not publicly covered and not provided by physicians. These services, which are usually provided by professional counselors and psychologists, are not captured in the databases we examined. As a result, we may have underestimated the overall extent to which the population receives counseling/psychotherapy (particularly among high-income groups who could pay out-of-pocket costs for these services) and probably understated the degree of income-related disparity. Analysis of recent Canadian data indicates that some of those with probable MDD had visited psychologists either exclusively (3.4%, 95% CI 1.8 to 4.9) or in conjunction with physicians (14.8%, 95% CI 11.0 to 18.5). 7 Fourth, our pharmacotherapy results were based on filled prescriptions, which could overestimate actual use and underestimate prescribing practices. Fifth, because many of the individuals in our cohort could not be assigned to a specific major source of care, our models may have underestimated the magnitude of practice variations. Sixth, our results may not generalize to other jurisdictions because of the peculiarities of the BC health system. Last, our analyses are based only on individuals who receive a diagnosis from the formal health care system. If everyone with MDD could be accounted for, the magnitude of the gap in minimally adequate treatment for depression would be much higher than what our results show.
Conclusion
Only about half of those with depression receive either MACP or MAAT. Disparities also persist, affecting mostly men and younger individuals. A multifactorial approach is therefore needed to improve access to and reduce variations in the receipt of minimally adequate depression care.
Footnotes
Authors’ Note
The opinions expressed in this publication are those of the authors and do not necessarily reflect the official views of the Canadian Institutes of Health Research, University of British Columbia, BC Ministry of Health, Data Stewardship Committee, or Vital Statistics Agency. This article was presented as a Poster Presentation at the Canadian Association for Health Services and Policy Research Conference, Montreal, QC, 2015 May 26–28.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Mr. Puyat is supported by a Banting and Best CGS Doctoral Research Award from the Canadian Institutes of Health Research (CIHR) and a Four Year Doctoral Fellowship Award from the University of British Columbia (UBC).