
Abstract
Objective:
Racial discrimination is a social determinant of health for First Nations people. Cultural resilience has been regarded as a potentially positive resource for social outcomes. Using a compensatory model of resilience, this study sought to determine if cultural resilience (compensatory factor) neutralized or offset the detrimental effect of racial discrimination (social risk factor) on stress (outcome).
Methods:
Data were collected from October 2012 to February 2013 (N = 340) from adult members of the Kettle and Stony Point First Nation community in Ontario, Canada. The outcome was perceived stress; risk factor, racial discrimination; and compensatory factor, cultural resilience. Control variables included individual (education, sociability) and family (marital status, socioeconomic status) resilience resources and demographics (age and gender). The model was tested using sequential regression.
Results:
The risk factor, racial discrimination, increased stress across steps of the sequential model, while cultural resilience had an opposite modest effect on stress levels. In the final model with all variables, age and gender were significant, with the former having a negative effect on stress and women reporting higher levels of stress than males. Education, marital status, and socioeconomic status (household income) were not significant in the model. The model had R2 = 0.21 and adjusted R2 = 0.18 and semipartial correlation (squared) of 0.04 and 0.01 for racial discrimination and cultural resilience, respectively.
Conclusions:
In this study, cultural resilience compensated for the detrimental effect of racial discrimination on stress in a modest manner. These findings may support the development of programs and services fostering First Nations culture, pending further study.
Clinical Implications
As a social determinant of health, racial discrimination experienced by First Nations people has a detrimental effect on stress. First Nations cultural resilience may play a modest role in compensating for the negative effects of racial discrimination on stress, but it must be understood alongside other key social factors. Strategies aimed at building cultural resilience could modestly reduce stress and improve health outcomes given the experience of racial discrimination.
Limitations
The nonvalidated measure of cultural resilience must be interpreted with caution as it captured individual perceptions of cultural community strengths and did not assess personal engagement in cultural activities. This study design was cross-sectional and cannot distinguish temporality of relationships in the model. Data captured one level of analysis (individual) despite cultural resilience and racial discrimination being multilevel concepts. The sample was from one First Nation community and not applicable to all Aboriginal peoples (e.g., First Nations off-reserve, Métis, Inuit).
The social determinants of health are emphasized in understanding health inequality. 1 There remain decisive gaps in our understanding of health inequality founded on race: previous research has been unable to explain away effects, taking into account factors, such as gender, age, poverty, residential locale, and health risk behaviours. 2 –6 The effect of racial discrimination is likely an integral part of the process driving racial inequality, with evidence linking it to manifold outcomes, such as poor self-rated health, immune dysregulation, hypertension, obesity, sleep difficulty, preterm birth, frequent colds, mental health, and substance use disorders. 7 –19
A social construction, the concept of race is premised on the erroneous belief of meaningful genetic or biological differences of groups in the population based on arbitrary physical markers, such as skin color. 20,21 Racism is an ideology using race to frame social relations; it often results in prejudice or negative attitudes, beliefs, and opinions, directed at racialized groups, as well as discrimination or differential treatment of group members to accord rights, privileges, and resources at multiple levels in society. 21 –24 Racialization emphasizes the social and historical mechanisms underlying how groups come to be defined based on supposed biological differences (race), the power dynamics and oppression inherent in the process across time and space, institutionalization of this ideology in society, and ways it contributes to a system of social inequality. 22,24,25
Racial discrimination is an upstream or fundamental determinant of health, causing proximate health risk factors, health ailments, and diseases, across time, through a number of pathways. 1,26 –28 One mechanism driving the adverse effect of racial discrimination on health is the experience of acute and chronic stress. 29 –37
Nevertheless, internationally, there is limited work on racial discrimination, health outcomes, and determinants, such as stress, using representative quantitative data at the population level. 10,28,38 This includes Indigenous (Aboriginal) peoples globally, a heterogeneous group, yet sharing many common experiences, such as racial discrimination, historical trauma, poor health, and low socioeconomic outcomes. 39 –42 Recent contributions have attempted to address this gap in Canada among Aboriginal peoples, with limitations including the non-Aboriginal-specific measure of racial discrimination, paucity of quantitative approaches, small nonrandom samples, or focus on the off-reserve population. 43 –45 Advancing research in this area requires the analysis of inter- and intraracial group experiences of racial discrimination, 46 including the unique historical circumstances of Aboriginal peoples in Canada, a diverse, young, rapidly growing population, with subgroups, First Nations (on/off-reserve), Métis, and Inuit. 40,47
In addition to assessing the link between racial discrimination and stress, understanding the ways people are able to be resilient in light of such circumstances has research, clinical, and policy significance. The history and debates surrounding resilience have been detailed in the literature, 48,49 but most agree that it is the ability to thrive, succeed, or return back to an original state in the face of exposure to risk, adversity, challenges, or demands. 50,51
Resilience has been conceptualized in many ways, but the traditional focus has been on personal qualities or traits, with recent work emphasizing not only the individual but the role of family, community, physical, and social ecology as well. 52 –55 For example, resilience resources at different levels can include the following: individual (constitutional resilience, sociability, intelligence, communication skills, and personal attributes), family (supportive families and socioeconomic status), and community (school experiences, supportive communities, and cultural resilience). 52,56
Beyond the traditional constructs in resilience research, the body of work on Aboriginal resiliency has begun to receive consideration, emphasizing Aboriginal-specific constructs (traditional activities and lands, environment, spiritual factors, degree of integration within Aboriginal culture, or enculturation) and their contribution to a host of outcomes, both positive and negative. 44,56 –72 Resilience centred on culture highlights the value of having a shared set of common beliefs and values, with core elements such as language, conventions, socialization, social institutions, enhancing survival, comfort, and psychological needs for meaning and significance. 70,71,73 The loss of culture associated with colonialism and assimilation policies among Aboriginal peoples in Canada have been the subject of great focus. 40,74,75
Given the well-documented gap in well-being across a number of indicators for the Aboriginal population, 40 identifying the sources of cultural resiliency that enable success in the face of specific adverse conditions is particularly useful. This process requires strict attention to the idea that Aboriginal enculturation and cultural orientation are far from fixed; in fact, despite commonalities, culturally distinctive strategies of resilience reflect the diversity of Aboriginal peoples given their varied histories, environments, and lifeways. 58,76 In this respect, the development and application of universal, standardized measures of cultural resilience across Aboriginal communities is not the way to proceed. 70,71,77 Moreover, resiliency does not necessarily apply to all aspects of life and in positive ways 78,79 ; for example, some evidence has found higher enculturation is associated with more racial discrimination. 44,69 Therefore, theoretical models must be tested empirically to identify those contexts or domains in which resiliency factors operate to assist and protect people and which ones they do not. This work contributes to the body of research in this regard using the compensatory model of resilience within the scope of racial discrimination.
Well established in the resilience literature, the compensatory model of resilience captures the manner in which resilience resources may neutralize exposure to a social risk factor given a specific outcome. 80 In other words, a social risk factor has a detrimental effect on the outcome, and the compensatory factor has a positive effect on the outcome, with the 2 effects relatively independent of one another. Statistically, in this framework, both social risk factor and compensatory factor combine additively in a regression model, with independent effects on the outcome of interest but in opposite ways.
In sum, using a compensatory model of resilience, this theoretically driven study aimed to examine racial discrimination (risk factor) and cultural resilience (compensatory factor) as predictors of stress (outcome). It was hypothesized that in the First Nations population, cultural resilience compensates for the detrimental, independent effect of racism on stress, taking into account non-cultural-specific resilience resources and demographic characteristics.
Methods
Sample
The sample was collected as part of Researching Health in Ontario Communities (RHOC), funded by the Canadian Institutes of Health Research, seeking to improve understanding of mental health, substance use, and violence in Ontario communities, including First Nations. 81 Data were collected from October 2012 to February 2013 (N = 340) from adult (18 years and older) members of the Kettle and Stony Point First Nation community, with a response rate of 57.3%.
The study was approved by the Research Ethics Board of the Centre for Addiction and Mental Health and the Band Chief and Council. Research protocols address the Tri-Council Policy Statement on Ethics of Research Involving First Nations, Inuit, and Métis Peoples of Canada and the principles of Ownership, Control, Access, and Possession. 82,83 Kettle and Stony Point First Nation screened this research article for potential impact on the community and the interests of its members.
Measures
As a highly engaged community-partnered project with the Kettle and Stony Point First Nation, tailored, community-specific questions and measures were developed.
In the compensatory model of resilience, the outcome variable, stress, was measured using the Perceived Stress Scale (Cronbach’s α [sample] = 0.76), asking respondents how often they felt or thought a certain way across a series of situations in one’s life over the past month, using 10 items scored as never (0), almost never (1), sometimes (2), fairly often (3), or very often (4), ranging from 0 to 40. 84 One of the most widely used measures for psychological stress, its psychometric properties have been evaluated cross-culturally and in numerous countries. 85
The risk factor, perceived racial discrimination, was indicated by the Measure of Indigenous Racism Experience (MIRE) Interpersonal Racism Scale (Cronbach’s α [sample] = 0.89), using 10 items addressing respondent perceptions about the frequency of experiencing racism across different contexts, with no restriction of the time period in which it occurred, scored as never (0), almost never (1), sometimes (2), fairly often (3), or very often (4), ranging from 0 to 40. 86 Created in Australia, this is the first validated instrument to capture the unique experience and multiple facets of racism among Indigenous peoples. As a comprehensive measure of the various settings where interpersonal racism may occur, its relevance is high for all individuals. 86 Self-reported experiences of racial discrimination have been the subject of greatest study in racism research, with members of racialized groups aware of at least some of the experiences of discrimination, resulting in elevated stress levels. 23,87 The traumatic experience of racial discrimination can have long-lasting effects over time. 23,86,87
The compensatory variable was a measure of individual Aboriginal cultural resilience. Across research foci, theoretical approaches, levels of analysis, ages of respondents, outcome measures, and social/geographical contexts, there are a wide range of ways Aboriginal cultural resilience has been defined and measured across studies, with the majority of measures not validated. 71 While this diversity limits generalizability, one advantage is that the assorted nature of this construct can be captured, as it varies with respect to geographic, economic, social, and historical context. 71 This article and the larger project were not specifically designed to assess the validity of a cultural resilience measure; it was created for this study based on the availability of cultural measures, but as noted earlier, as a community-partnered project, the questions were tailored, community specific, and the analysis developed with, and screened by, the community. In this study, the measure was based on a question that asked community members to identify perceived strengths of the community: “What are the main strengths of Kettle & Stony Point First Nation?” followed by a list of response options, including 4 items of cultural relevance (traditional language, traditional ceremonial activities and awareness of First Nations culture, elders, and the natural environment), 55,58,75 scored as no (0) and yes (1), with the scale ranging from 0 to 4. Internal consistency was acceptable (Cronbach’s α [sample] = 0.66). 88 Individuals who perceive different aspects of Aboriginal culture as strengths of the community may be more likely to be racially socialized, culturally aware, and have higher levels of cultural pride and enculturation as evidenced in other contexts. 89 Note that the level of measurement and unit of analysis is the individual.
Individual resilience resources included education (less than high school, completed high school, or any postsecondary education) and sociability, measured by the Social Support Scale (Cronbach’s α [sample] = 0.81), using 5 items scored as strongly disagree (1), disagree (2), agree (3), or agree strongly (4), ranging from 5 to 20. 90,91
Family resilience resources were marital status (married or living with partner; widowed, divorced, or separated; or single) and socioeconomic status, operationalized as household income (less than $20,000, $20,000-$39,999, $40,000-$59,999, or $60,000 and over).
Finally, the demographic variables were age and gender.
Statistical Analysis
Analyses were conducted using SPSS Statistics 21 (SPSS, Inc., an IBM Company, Chicago, IL). Missing data were handled using multiple imputation. 92 –95 The amount of missing data was relatively low, with household income (24%) the highest followed by perceived stress (14%) and the remaining variables less than 2%. Descriptive statistics were followed by a sequential linear regression to assess the compensatory model of resilience hypothesized. 80 First, the risk factor, MIRE Interpersonal Racism Scale, was added to the model to provide an unadjusted estimate of its effect on stress. Second, the compensatory factor, Aboriginal cultural resilience, was added to the model to assess its unique additive effect on stress. Last, the effects of the risk factor and compensatory factor were examined in the full model, with other resilience resources and demographic variables. The significance level was set at P < 0.05.
Results
Descriptive statistics are provided in Table 1. The sequential regression analysis presented in Table 2 shows that the MIRE Interpersonal Racism Scale increased stress levels in a relatively consistent manner across all 3 steps of the model while cultural resilience had the opposite effect on stress levels. With all variables in the model, the MIRE Interpersonal Racism Scale had about a 2.0% increase in stress for every 5-point increase on the 40-point scale. The effect of cultural resilience was a 1.5% decrease in stress for a 1-point increase on the 4-point scale.
Characteristics of the Study Sample (N = 340).a
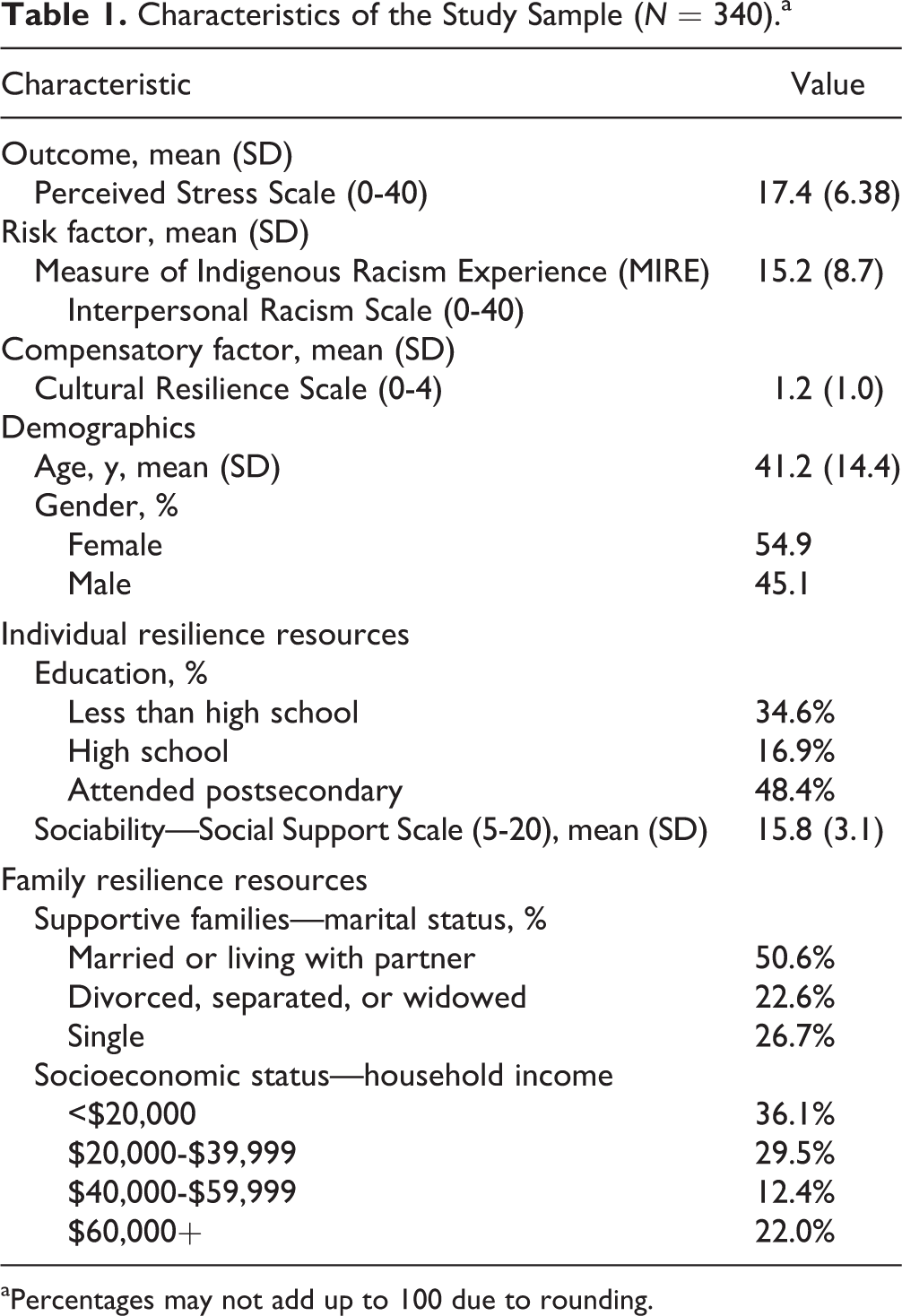
aPercentages may not add up to 100 due to rounding.
Sequential Linear Regression Model Predicting Stress (Perceived Stress Scale) Scores (N = 340).
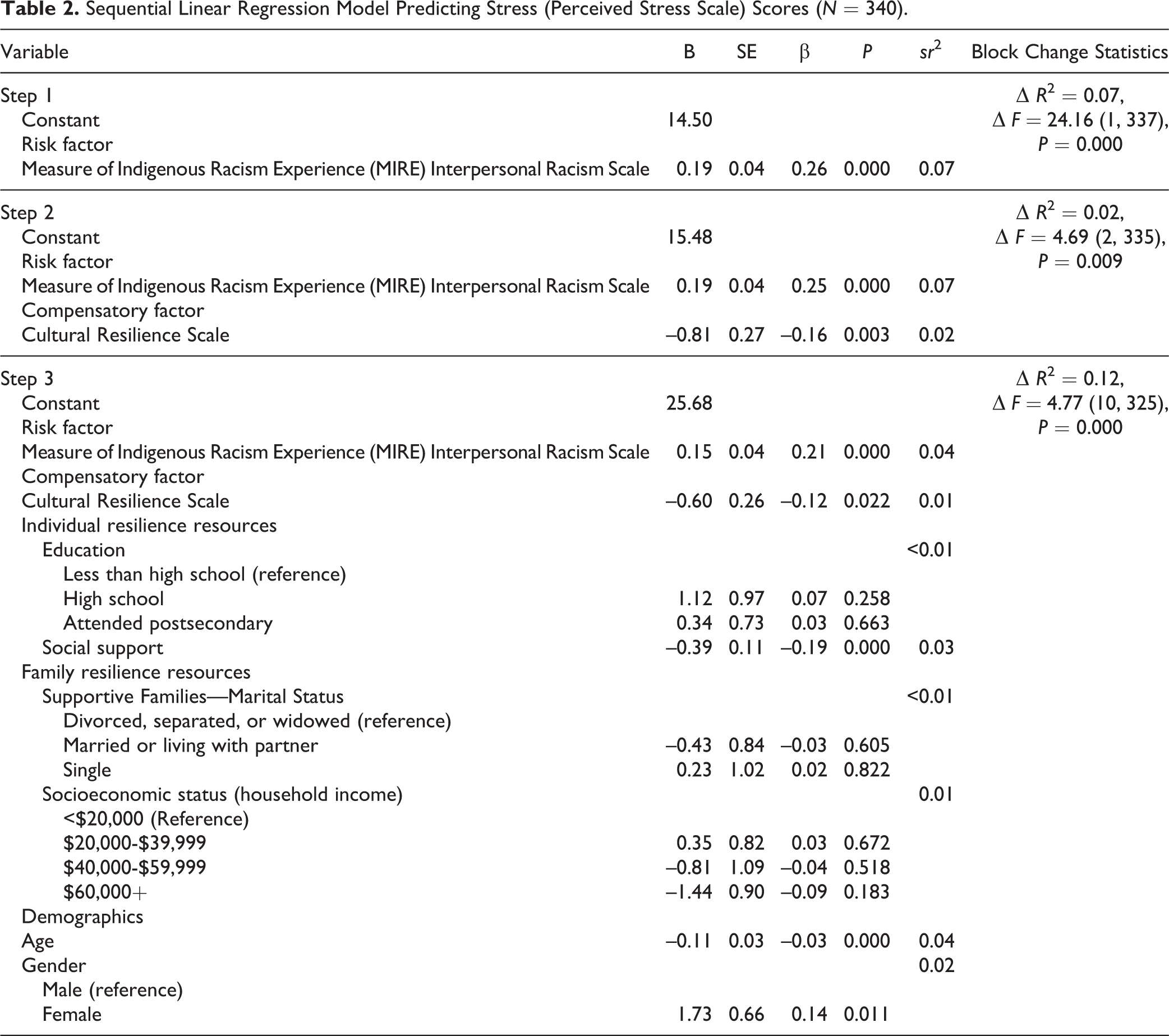
As well, in the final adjusted model with all variables, both demographic variables, age and gender, were significant, with the former having a negative effect on stress or a 2.7% decrease in stress for every 10 years and women reporting a 4.3% higher level of stress than men. Social support was significant in the model and decreased stress by about 1% for a 1-point increase on the 15-point scale. The individual resilience resource, education, and none of the family resilience resources, marital status and socioeconomic status (household income), were significant in the model.
The standardized regression coefficients in the final model illustrated that among the continuous variables, MIRE Interpersonal Racism had the strongest impact on stress, followed by social support and cultural resilience.
Overall, the model was significant at each step of the sequential regression. R 2 = 0.21 and adjusted R 2 = 0.18, with about one-fifth of the variance in stress explained by the model. The semipartial correlation (squared) values in Table 2 indicate that MIRE Interpersonal Racism explained uniquely 4% of the variance in stress, and cultural resilience accounted for 1%. In addition, social support (3%), gender (2%), and age (4%) contributed uniquely a combined 9% of the variance in stress to the model.
Discussion
Using a compensatory model of resilience, this research examined the protective effect of Aboriginal cultural resilience on stress in the context of an important risk factor for Aboriginal peoples, racial discrimination. The link between racial discrimination and stress was supported in this study, which is congruent with work examining other racialized populations. 29 –34 The positive role of cultural resilience was not a unique finding, 64 –66 but its demonstrated compensatory role in protecting First Nations from stress in the presence of the social risk factor, racial discrimination, while taking into account a host of other resilience resources and demographic factors is a new contribution to the literature. That being said, it played a minor role in explaining stress relative to other factors, and its effect was modest.
The measure of cultural resilience used in this work reflected individual perceptions of cultural strengths of the community, including traditional language, traditional ceremonial activities and awareness of First Nations culture, elders, and the natural environment. While the data were not amendable to teasing out the way cultural resilience operates to protect against stress, we speculate that this may be a product of several direct and indirect processes associated with core elements of enculturation: transmitting cultural traditions; increasing bonding and racial socialization, including the development of racial pride, unity and heritage, culturally relevant adaptive coping strategies and skills, a stable and positive racial identity, personal continuity and agency, meaning, sense of purpose, and self-esteem; and enabling community members to actuate cultural resilience. 52,61,75,77,89,96 Moreover, Aboriginal culture cannot be understood in the absence of a people’s land and natural environment; the two are synonymous as there is a deep physical, spiritual, and emotional relationship with the land that is the foundation of the self and existence and lifeblood of Aboriginal well-being. 55,58,75 Despite the proposed mechanisms of the compensatory factor, we caution that the reduction in stress observed requires further efforts to clarify the protective role of cultural resilience in the presence of social risk factors, such as racial discrimination.
Although not of central interest in this study, the reduction in stress from social support was strong and consistent with earlier work examining its role in other contexts and populations. 97,98 In fact, this finding shows that as a resiliency resource, the reciprocal relationships characterizing Aboriginal cultures serve a protective role for health and well-being. 55,99
Family resilience resources were not important in this analysis. The measure of supportive families, marital status, did not assess the quality of family relationships, including partnerships (married or living with partner), which is a potential resilience resource. 100 Socioeconomic status (household income) had no effect in this study; in fact, this result contrasts with previous work on the general population finding more stressful events and less coping resources among individuals with decreasing levels of socioeconomic resources. 101,102
With respect to gender, similar to other research, the different social experiences of males and females contributed to varying amounts of stress with higher levels found among the latter. 101 The findings reflect evidence that First Nations females are particularly likely to be disadvantaged in numerous ways: poverty of subsistence, sexual and reproductive health, identity, safety and security, mental health, social participation, power, and knowledge. 103
Finally, consistent with previous studies, 101,104 improved coping mechanisms, higher self-efficacy, and positive outlook likely account for lower stress as individuals age.
Clinical Implications
Moving forward, facilitating cultural resilience for individuals in Aboriginal communities may be a somewhat helpful strategy in improving outcomes among people suffering from stress rooted in racial discrimination. This relationship, however, requires further clarification, but this level of intervention may mitigate stress-related effects on health and associated behaviours given the well-documented research on the poor health and well-being of First Nations people. 2,39,41,105,106 The utility of cultural resilience is tempered by the modest size of the effect and importance of understanding it within the context of other stronger determinants of stress, including racial discrimination, age, gender, and social support.
Failure to address adequately racial discrimination as a fundamental social determinant of health will leave us unable to reduce health inequalities founded on race. 28,87 The trans-generational consequences of racial discrimination and evidence of the effects of racial discrimination on maternal stress and preterm birth, 29,107 coupled with rapid growth of the Aboriginal population in Canada, 47 make this a particularly important social issue. The identification and fostering of resilience resources must not take away the spotlight from social structure, producing patterns of racial inequality and racial discrimination, to ultimately eliminate gaps in health outcomes.
Strengths and Limitations
This study has several strengths. It was a highly engaged community-partnered project in which community-specific issues were addressed as seen in all aspects of the research design and analysis. The study was quantitative from a representative random sample of one on-reserve First Nation community. Although the data were drawn from a single First Nation community, limiting generalizability nationwide, this eliminated the issue related to homogenization of resilience within this population by pooling together several communities. 58,70,71,77 The Kettle and Stony Point First Nation advisory committee provided guidance and screened this research article for potential impact on the community and the interests of its members. Finally, this research used 2 key validated measures: 1) the PSS, which is a powerful measure of stress associated with health and well-being, and 2) the MIRE Interpersonal Racism Scale that is specific to Indigenous peoples.
There are some key limitations associated with this work. The measure of cultural resilience was internally consistent but not psychometrically validated. This article and the larger project were not specifically designed to assess the validity of the cultural resilience measure. This is, however, an important focus moving forward. The scale was created for this study based on the availability of cultural measures for this specific community. Also, the measure of cultural resilience captured individual perceptions of Aboriginal community strengths but did not measure personal engagement in cultural activities. The assumption was that individuals who perceive different aspects of Aboriginal culture as strengths of the community may be more likely to be racially socialized, be culturally aware, and have higher levels of cultural pride and enculturation as evidenced in other contexts. 89 This, however, may or may not be the case; for example, individuals who are highly enculturated may be more likely to perceive the level of community cultural strengths as weak or individuals who are more likely to be stressed may also be the type of people who do not feel positive about their community and more likely to perceive racial discrimination. Next, the sample was from one First Nation community, limiting the generalizability beyond this specific group, and the data were not multilevel, disallowing us to disaggregate multiple levels of influence from one another, a central issue across studies in this area. Finally, the cross-sectional research design undermined causal inferences—longitudinal research is needed to distinguish relationships between social risk factors, protective factors, and outcomes, as well as the long-term impact of racial discrimination on stress. Thus, these findings should be interpreted within the context of these constraints.
Conclusion
As a driver of social and health inequality, this work showed a positive effect of racial discrimination on stress in the Aboriginal population. A compensatory model of resilience illustrated the unique but modest benefits of cultural resilience in offsetting the experience of stress resulting from racial discrimination. In addition, a non-Aboriginal-specific source of resilience, social support, figured prominently in reducing stress. However, the cross-sectional research design and measure of cultural resilience indicate that additional research is needed before developing large-scale recommendations for clinical practice or policy. Future research should look at specific pathways by which racial discrimination affects stress and health outcomes within the Aboriginal population (First Nations on/off-reserve, Métis, Inuit) and across racialized groups in Canada, given their varied histories and experiences, coupled with the contexts and manner in which resilience resources, both cultural and noncultural, play a fundamental role.
Footnotes
Acknowledgments
We extend our sincere appreciation and thanks to the many individuals and groups that have contributed to the development of this article. We are grateful to Kettle & Stony Point First Nation Chief & Council for allowing us to conduct the Researching Health in Ontario Communities (RHOC) project and the staff of Kettle & Stony Point Health Services, who helped recruit participants and promote the project. We also extend our sincere gratitude to the project’s Research Advisory Committee—Shirley Fowler, Tracey Williams, Vince George, Dianne George, Janet George, and Roxanne White. Your guidance and understanding taught us patience with a complex process—resulting in findings we are confident will make a valuable contribution to Kettle & Stony Point First Nation and beyond. Thank you to those individuals who served as research assistants for the project in Kettle & Stony Point—Margaret Pepper, Sara George, Leigh George, and Katie Big-Canoe. We also thank Barb Shipley for her logistical support and the staff of Chippewa Technical Services for setting up electrical requirements of the lab. We would also like to acknowledge Roseanne Pulford for preparing and processing research materials. We thank Peter Fewster for his assistance with Checkbox and Sharon Bernards for also assisting with Checkbox and her expertise in data management. Also, we are very grateful to all of the community members who participated in the project. Your experiences have and will continue to provide valuable insight that will improve programs and services. Finally, we thank the 3 anonymous reviewers for their thoughtful and insightful comments and suggestions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was made possible with funds from a Canadian Institutes of Health Research (CIHR) Emerging Team Grant: Co-morbidity of Brain Disorders and Other Health Problems (CBG—101926). All authors report no conflicts of interest..