
Abstract
Objective:
Attention-deficit hyperactivity disorder is one of the most frequent neurodevelopmental disorders. Its diagnosis requires reference questionnaires such as the Conners’ Parent Rating Scale (CPRS). Presently, in French-speaking countries, a few translations of the revised short CPRS have been put to use without previous formal validation. We sought here for the validation of a French version (Lausanne, Switzerland) of the revised short CPRS regarding construct validity, internal consistency, and item reliability in a sample of French schoolchildren.
Method:
The study involved 795 children and adolescents aged 9 to 19 years from a single school. The factorial structure and item reliability were assessed with a confirmatory factor analysis for ordered categorical variables. The dimension internal consistency was assessed with Guttman’s lambda 6 coefficient.
Results:
The results confirmed the original and strong 3-dimensional factorial structure (Oppositional, Cognitive Problems/Inattention, and Hyperactivity), showed satisfactory item reliability, and indicated a good dimension internal consistency (Guttman’s lambda 6 coefficient: 0.87, 0.90, and 0.82, respectively, to the 3 dimensions).
Conclusions:
Thus, the Lausanne French version of the revised short CPRS may be considered validated regarding construct validity and item and dimension reliability; it can be now more confidently used in clinical practice.
Attention-deficit hyperactivity disorder (ADHD) is one of the most frequent neurodevelopmental disorders. It affects 1% to 20% of school-aged children, and its global prevalence is 5.3% (95% CI, 5.0 to 5.6). 1
The current knowledge is orienting the understanding of this disorder toward a multifactorial cause: genetic, biological, environmental, and psychosocial. 2 The main clinical presentations are difficulties with concentration, organization, and planning; impulsivity; and, very often, motor hyperactivity. 3 –5
For ADHD diagnosis, the international guidelines recommend first a clinical examination, then the use of reference questionnaires 4,5 (Conners’ Parent Rating Scale [CPRS] 6 or ADHD Rating Scale 7 ). These questionnaires have been scientifically validated and investigate the overall functioning of a given subject in various environments (school, family, etc.).
The long form of the revised CPRS (CPRS-R: L) includes 48 items divided into 7 dimensions. The short form of the CPRS-R (the CPRS-R: S) includes 27 items, of which 18 quantify 3 dimensions: Oppositional, Cognitive Problems/Inattention, and Hyperactivity. The 9 remaining items and 3 items from the Cognitive Problems/Inattention dimension provide an ADHD index.
A number of studies have demonstrated the relevance of the various CPRSs and underlined the advantages of the CPRS-R in investigating ADHD. 8 Some Conners’ scales have been already translated and validated in various languages (Turkish, 9 Swedish, 10 Spanish, 11 or rural Bengali 12 ). A few French versions of the CPRS-R: S are also available; however, to our knowledge, although widely used, none has been validated yet. In 2006, the American CPRS-R: S6 was translated into French and then back-translated in Lausanne, Switzerland 13 (Table 1) in collaboration with Multi-Health Systems (New York, NY, and Toronto, Canada).
French Version of the Conners’ Parent Rating Scale,a Short Form (CPRS-R: S) Used for the Study (Lausanne Translation).
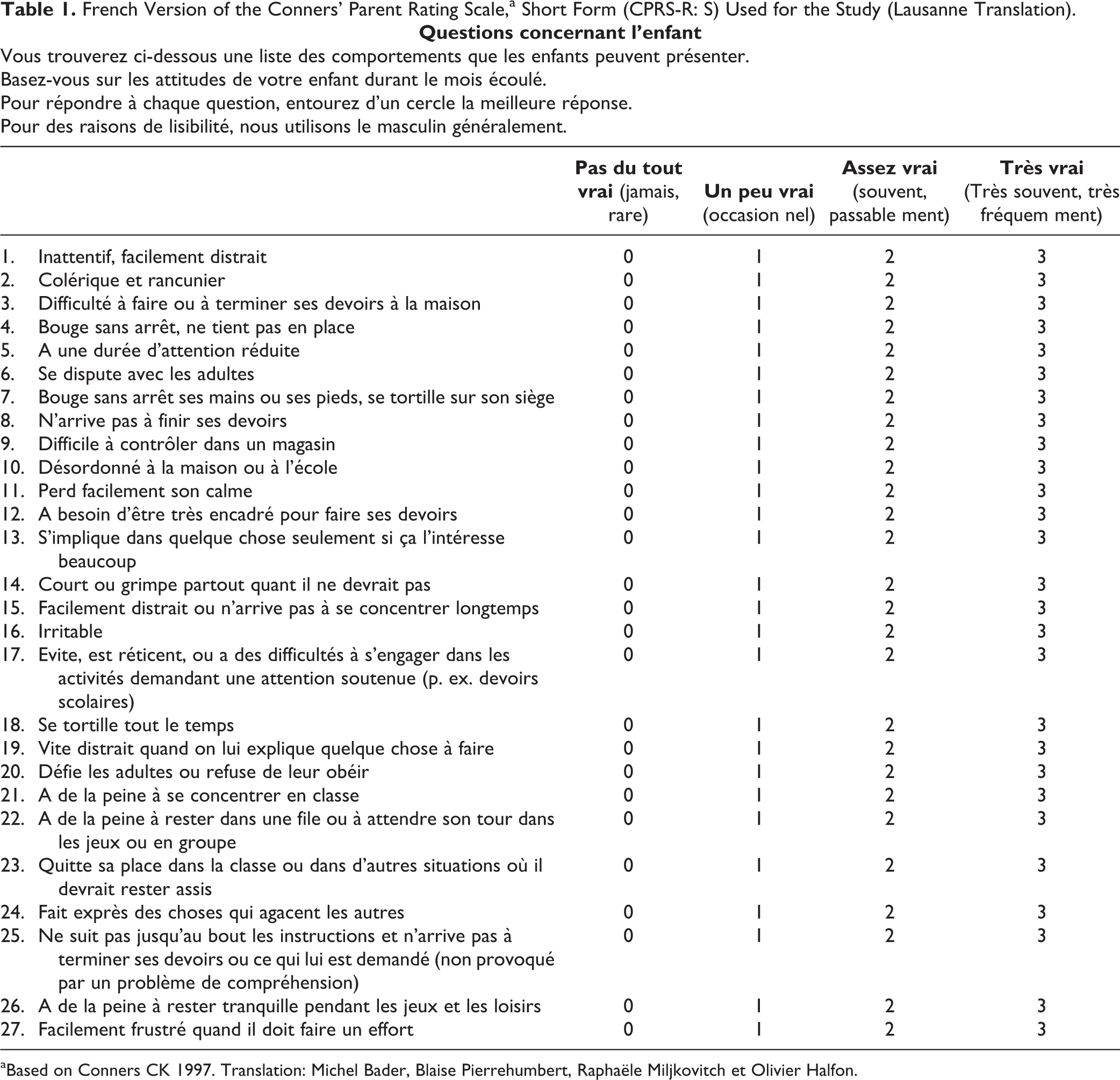
aBased on Conners CK 1997. Translation: Michel Bader, Blaise Pierrehumbert, Raphaële Miljkovitch et Olivier Halfon.
The present article reports the validation of this French version regarding its construct validity, internal consistency of the dimensions, and reliability of the items.
Methods
Study Population
By the end of 2011, the study team solicited the parents of 1218 schoolchildren (40 mid-level classes of a private school in Lyon, France) via the school principal and then the head teachers. The approach included an explanatory note and a whole questionnaire (see the 27-item form in Table 1) to fill out freely and anonymously.
Among the 901 returned questionnaires (74% of those sent), 106 were left blank; thus, the response rate was 65% (795 of 1218). The responses corresponded to 366 boys and 374 girls; the sex was not mentioned in 55 forms. The mean ± SD age of the children was 12.7 ± 1.3 years (range: 9-19). Data on all 795 children/adolescents were kept for statistical analysis. The parents of the children under study belonged to the rather well-educated French middle class. In other words, 79% of the children had at least one parent with higher education (nearly 70% of the mothers and 60% of the fathers), and 87% of the mothers and 97% of the fathers were in paid full-time or part-time employment.
Data
The data were the responses to the 18 items that quantify the 3 dimensions of the American version of the CPRS-R: S. 6,14,15 These dimensions were 1) Oppositional (items 2, 6, 11, 16, 20, and 24), 2) Cognitive Problems/Inattention (items 3, 8, 12, 17, 21, and 25), and 3) Hyperactivity (items 4, 9, 14, 18, 22, and 26). Each item is rated on a 4-point Likert scale (0 = not true at all/Pas du tout vrai to 3 = very much true/Très vrai; see Table 1).
Statistical Methods
Confirmatory factor analysis
A confirmatory factor analysis (CFA) 16 checked the 4 hypotheses of the baseline CFA model (or model 1) applied to the French CPRS-R: S: 1) ADHD responses can be explained by 3 factors (also called latent variables, or dimensions): Oppositional, Cognitive Problems/Inattention, and Hyperactivity; 2) each item has a nonnull coefficient of regression on the dimension it was designed to measure (loading factor) and null loading factors on the 2 other dimensions; 3) the 3 factors are correlated; and 4) the residual errors associated with each item are uncorrelated (Figure 1).
As the items are ordinal variables, the parameters of the CFA models were estimated from polychoric correlation matrices, 17 using mean- and variance-adjusted weighted least squares (WLSMV).
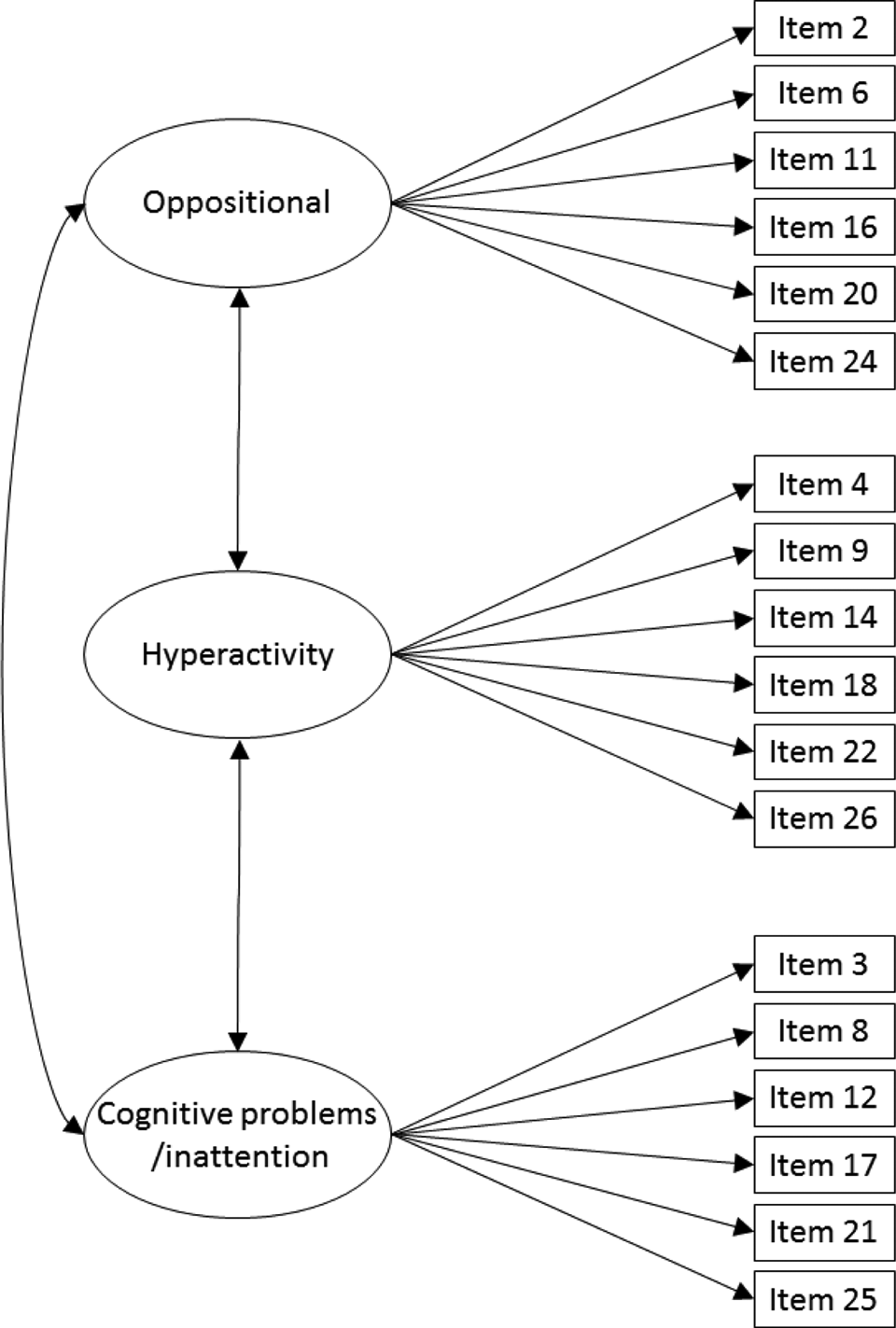
Baseline model (or model 1) for the French version of Conners’ Parent Rating Scale, Short Form (CPRS-R: S). In this diagram, each circle corresponds to a single dimension and each rectangle to a single item. The circles are linked to the rectangles by single-headed arrows only for items that reflect the dimension (i.e., items 2 and 6 for Oppositional and not for the other dimensions). The lack of arrows means that the loading factor is set at 0. The relationships between dimensions are represented by double-headed arrows between circles. This relationship is either a covariance or a correlation if the latent variables are standardized.
Items and latent variables were standardized leading to standardized parameters, thus standardized loading factors. This enables interpreting and comparing these loading factors as correlations.
Several indexes (with their distinct rules for good fit) were used to assess the fit of the CFA models: 1) the comparative fit index (CFI) 18,19 and the Tucker-Lewis index (TLI), 20 with “good fit” if >0.95; 2) the root mean square error of approximation (RMSEA) and its 90% confidence interval (CI) with “close fit” if <0.05 and fair fit in the 0.05 to 0.08 range; 21 3) the weighted root mean square residual (WRMR), with “good fit” if ≤1.0; 22 and 4) the modification indices (MIs). 23
The MIs were used to select additional parameters to improve the fit. A high MI indicates an important improvement. Alternative models may thus be obtained by adding to the initial model (model 1) one parameter at a time, starting with the parameter with the highest MI. This purely statistical approach was associated with pragmatic fit-improvement criteria: 1) the completely standardized expected parameter change (CS-EPC) associated with each MI is ≥0.3 (an item cannot reflect a given dimension if its standardized loading factor is <0.30 24,25 or <0.40), 26 and 2) the modifications and parameters (loading factors or residual correlations between items) are clinically meaningful (the wordings of the items are consistent with knowledge behind the development of the scale).
Item reliability
Item reliability was estimated through R2, that is, the part of the item variance that may be explained by its underlying dimension. It is equal to the square of the standardized loading factor of the item. 16
Dimension internal consistency
The internal consistency of each dimension was estimated using Guttman’s lambda 6 reliability coefficient. 27 Usually, the items of each dimension are considered heterogeneous, consistent, or redundant at values <0.7, close to 0.8, or >0.9, respectively.
Software Programs
CFA and item reliability were estimated using Mplus, version 7.11. 28 All other analyses used R, version 3.0.1 (http://www.r-project.org/). All tests were 2-tailed, and P < 0.05 was considered for statistical significance.
Results
Validation of the Factorial Structure
The statistical indexes used for the fit of model 1 (Table 2) were heterogeneous: the CFI and the TLI indicated a good fit (>0.95; precisely, 0.972 and 0.968, respectively), the RMSEA indicated a fair fit (0.059 [90% CI, 0.053 to 0.064], RMSEA ≤0.05 was rejected, P = 0.004), and the WRMR indicated a poor fit (1.321, so >1). Thus, model 1 could be slightly improved using the MIs.
Model Fit on the Basis of the Statistical Indexes.
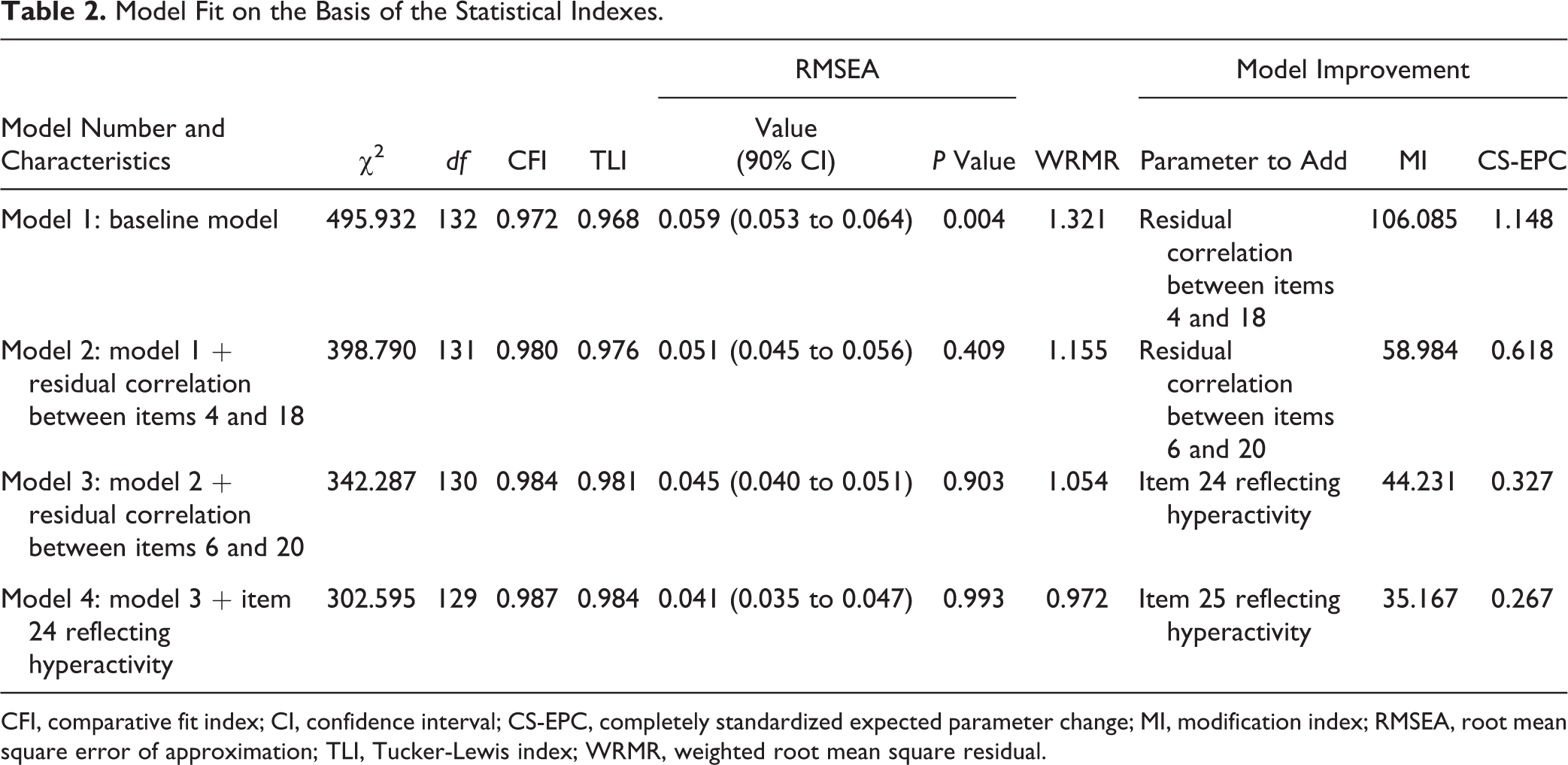
CFI, comparative fit index; CI, confidence interval; CS-EPC, completely standardized expected parameter change; MI, modification index; RMSEA, root mean square error of approximation; TLI, Tucker-Lewis index; WRMR, weighted root mean square residual.
The MIs suggested adding, in a first step, a residual correlation between items 4 and 18 of the Hyperactivity dimension and, in a second step, another residual correlation between items 6 and 20 of the Oppositional dimension. This led successively to models 2 and 3 (Table 2), with improved fit at each step. Model 3 was very well fitted according to the CFI, the TLI, and the RMSEA (0.045 [90% CI, 0.040 to 0.051], RMSEA ≤0.05 not rejected, P = 0.903), and the WRMR was much closer to 1 (1.054). No modification of model 3 was relevant regarding the statistical and pragmatic criteria: the MIs suggested that item 24 would also reflect the Hyperactivity dimension (model 3 in Table 2). This led to a weak improvement of the fit of model 4 (as per the WRMR) and did not satisfy the pragmatic fit-improvement criteria (standardized loading factor of item 24 <0.30).
Model 3 was finally retained for the French version of the CPRS-R: S. The standardized parameter estimates are shown in Figure 2. The fit of this model was very good according to the pragmatic criteria: all 18 standardized loading factors were >0.70, of which 12 were even >0.80. The loading factors, the correlation coefficients between the 3 dimensions, and the residual correlations were all statistically significant. In addition, the correlations between the latent variables were not too high: 0.70 between Hyperactivity and Oppositional, 0.56 between Cognitive Problems/Inattention and Oppositional, and 0.71 between Cognitive Problems/Inattention and Hyperactivity. This indicates that the model with 3 dimensions is relevant.
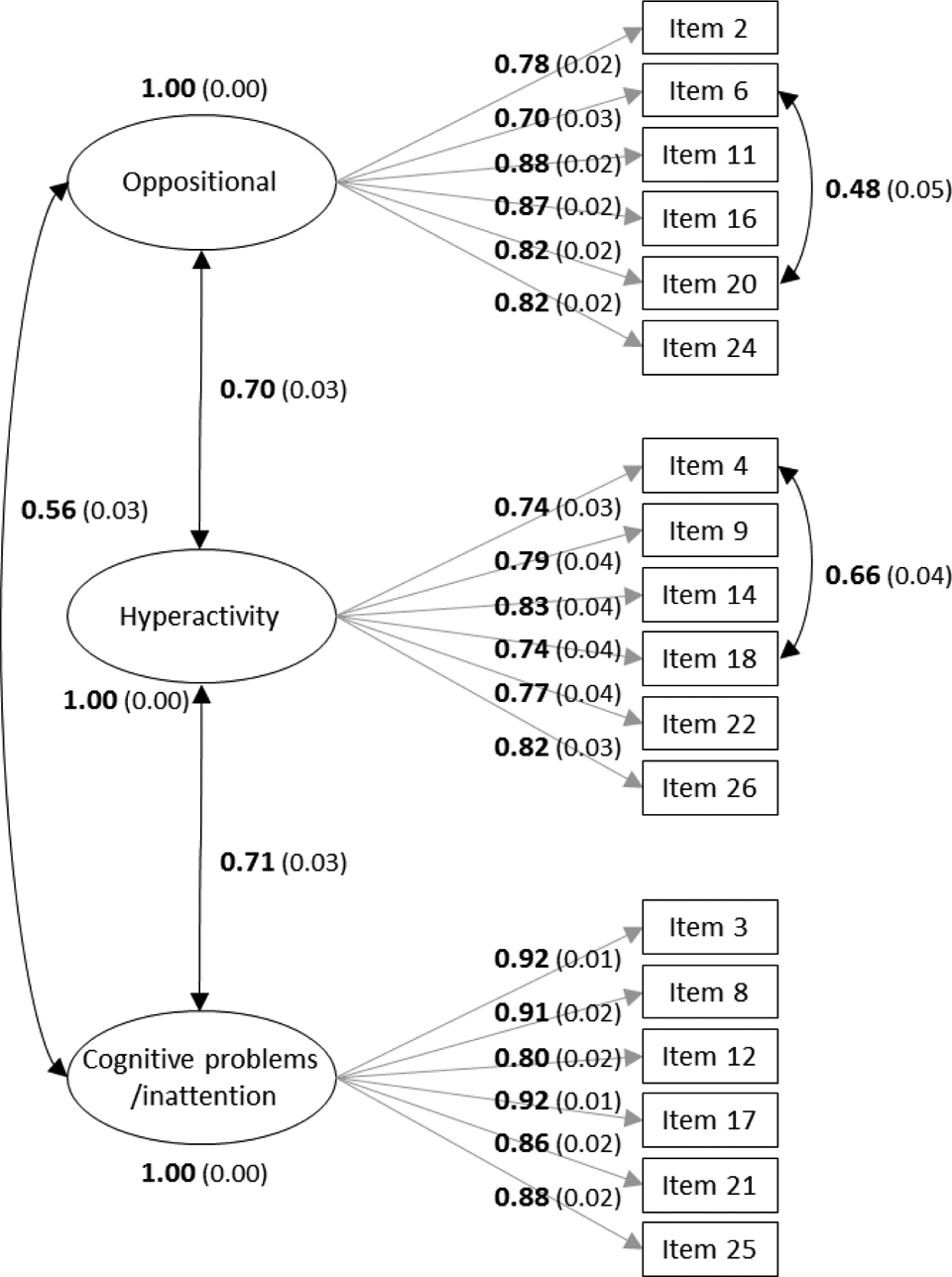
Final model for the French version of Conners’ Parent Rating Scale, Short Form (CPRS-R: S). Standardized parameter estimates and their standard errors.
Item Reliability
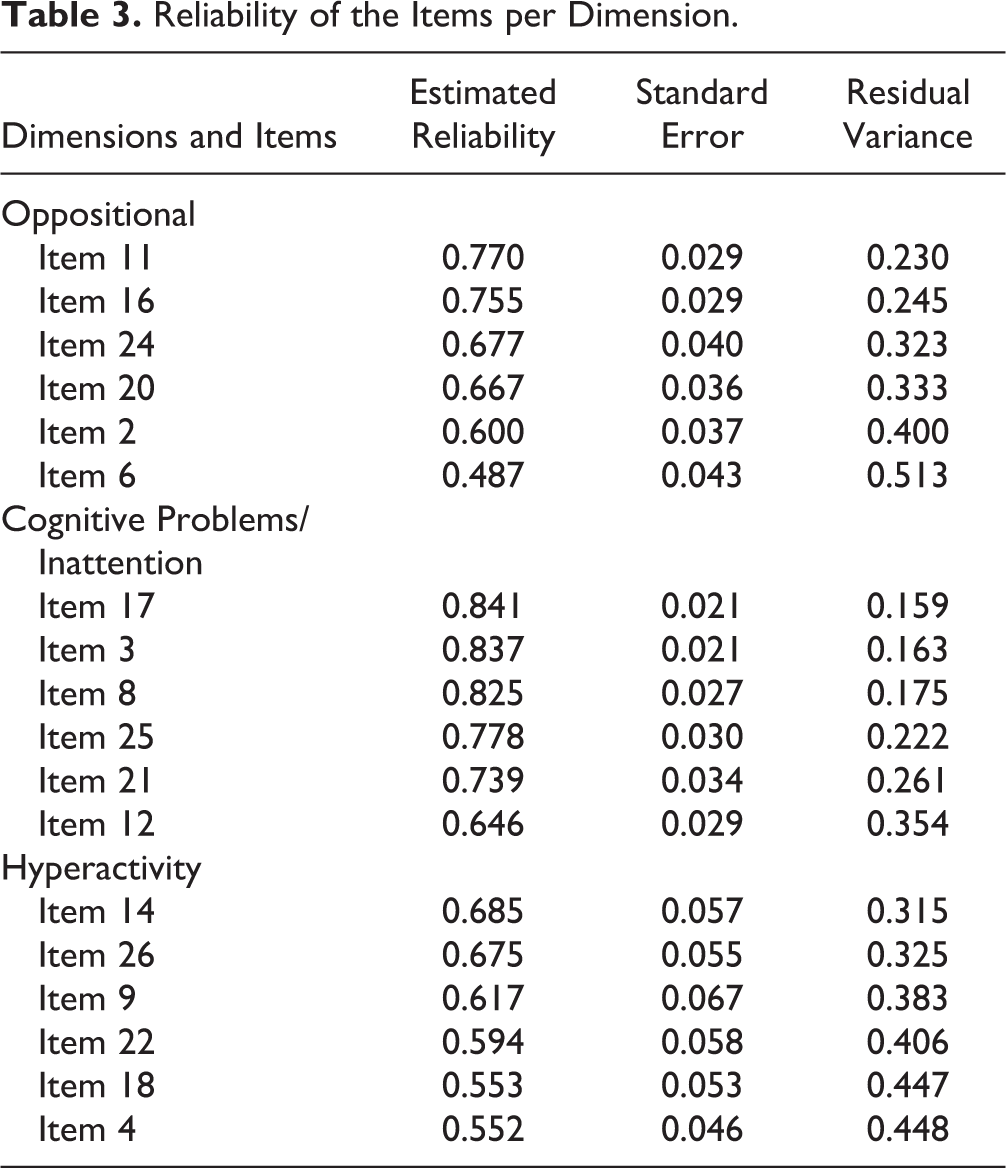
Table 3 shows the estimated reliabilities of all items in decreasing order within each dimension. These values ranged between 0.487 and 0.841 and were all, statistically speaking, significantly different from 0 (P < 0.0001). The lowest values belonged to items 18, 4, and 6 that had residual correlations.
Reliability of the Items per Dimension.
Internal Consistency
The coefficient of internal consistency was 0.87 for Oppositional, 0.90 for Cognitive Problems/Inattention, and 0.82 for Hyperactivity. The 3 dimensions are thus internally consistent.
Discussion
The existence of ADHD and its diagnosis and management are still the objects of lively debates. The tools recommended for the diagnostic approach are already widely used but sometimes inadequately or suboptimally. In testing the factorial validity of the Lausanne French version of the CPRS-R: S and in estimating item and dimension reliability, we wanted to provide French-speaking physicians and researchers a valid, reliable, and recognized tool.
The present results confirmed the 3 assumptions checked by the study: 1) a strong 3-dimensional factorial structure identical to that of the 1997 American version, 2) a satisfactory dimension internal consistency, and 3) a good item reliability. These properties make this rating scale a fairly objective behaviour assessment tool in ADHD.
One strength of the present study is that it takes into account the ordered categorical items into the CFAs. In a previous study, Kumar and Steer 29 did not use a robust categorical least squares estimator and thus could not confirm the 3-dimensional factorial structure stated by Conners et al. 6,14,15 Other explanations is that Kumar and Steer observed American psychiatric outpatients, whereas Conners et al. observed American and Canadian schoolchildren. This emphasizes the need for a study of the invariance of the scale between different populations using multigroup CFA for categorical data.
The present results showed that allowing for 2 residual correlations, one between items 6 and 20 and another between items 4 and 18, led to a better-fitted model but violated the fourth hypothesis of the baseline CFA model. This was not surprising because, in French, as in English, items 6 and 20 on one hand and items 4 and 18 on the other hand have very close meanings; however, to our knowledge, no residual correlations were considered in the models used with the American version. These residual correlations may stem from the specific feature of our sample (a single French school); they should be confirmed in other independent samples. Anyway, because each residual correlation belongs to items of the same dimension, this does not question the use of CFA models or the strong 3-dimensional factorial structure of the French version.
The suggested modification to model 3 (item 24 may reflect Oppositional as well as Hyperactivity) did not meet the pragmatic criteria (no evidence in French that item 24 does not suggest the Hyperactivity dimension). However, this suggestion was already present in childhood cancer survivors 30 ; this item should thus be carefully examined in further analyses.
Conclusions
To our knowledge, this is the first validation study on the French version of the CPRS-R: S. The next validation study will investigate the scale invariance, first by sex and age classes, then by clinical status (cases vs. controls). In case of invariance, scores by sex and age will be proposed that will allow reliable comparisons between same sex and age classes in similar populations. Other investigations such as test-retest reliability, interrater reliability, external validity, and, especially, sensitivity to change would be necessary. If these properties prove satisfactory, this French version of the CPRS-R: S will represent more than a complementary diagnostic tool; it will allow following children’s progress and using the version in international clinical trials.
Footnotes
Acknowledgments
Special thanks to Charles de Foucauld School Director for providing help and its students for their participation. Study conducted with financial support from Fonds de Perfectionnement du Centre Hospitalier Universitaire Vaudois, Société Académique Vaudoise, Fondation d’Entreprise Laboratoire Urgo, and Shire Pharmaceuticals Group.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics
Study carried out with agreements from 1) Comité de Protection des Personnes Lyon Sud Est II (France), obtained on January 5, 2012; 2) Comité Consultatif sur le Traitement de l’Information en matière de Recherche dans le domaine de la Santé (France), Agreement Nr. 12.185bis, issued on September 6, 2012; and 3) Commission Nationale de l’Informatique et des Libertés (France), Agreement Nr. DR-2012-524, issued on November 7, 2012.