
Abstract
Evolutionary approaches to medicine can shed light on the origins and etiology of disease. Such an approach may be especially useful in psychiatry, which frequently addresses conditions with heterogeneous presentation and unknown causes. We review several previous applications of evolutionary theory that highlight the ways in which psychiatric conditions may persist despite and because of natural selection. One lesson from the evolutionary approach is that some conditions currently classified as disorders (because they cause distress and impairment) may actually be caused by functioning adaptations operating “normally” (as designed by natural selection). Such conditions suggest an alternative illness model that may generate alternative intervention strategies. Thus, the evolutionary approach suggests that psychiatry should sometimes think differently about distress and impairment. The complexity of the human brain, including normal functioning and potential for dysfunctions, has developed over evolutionary time and has been shaped by natural selection. Understanding the evolutionary origins of psychiatric conditions is therefore a crucial component to a complete understanding of etiology.
Clinical Implications
Functioning adaptations can cause distress and meet current criteria for “disorder.” Functioning adaptations that lead to psychiatric conditions may require alternative treatments. Evolution is critical for a complete understanding of any condition’s etiology.
Limitations
Many researchers and clinicians have not been trained in evolutionary theory. Most evolutionary hypotheses in mental health have not yet been rigorously tested.
Evolutionary theory is the most fundamental organizing principle of biology and can inform research across all areas of health.
1
–3
An evolutionary understanding of why we get sick is a framework that generates explicit, testable predictions to better direct mechanistic research regarding how we get sick. This approach has improved our understanding of many conditions (e.g., infection, cancer, morning sickness, pain, fever, genetic disorders
2,3
) and may be especially useful for psychiatry because the precise etiology of mental illness is often unclear.
4
–10
Indeed, because the brain is a complex integration of adaptations designed by natural selection,
11
the evolutionary perspective is essential to completely understand the origin and etiology of mental illness.
Most researchers and clinicians accept that natural selection has played some role in shaping “normal” behaviour, but they are not trained to study abnormal behaviour from an evolutionary perspective. 12 This article briefly summarizes evolutionary accounts of psychiatric disorders as they are currently defined. Examples are typically theoretical and remain to be rigorously tested. We then discuss the implications of the evolutionary perspective for the conceptualization of psychiatric disorder generally.
Why Do Mental Disorders Exist and Persist?
The etiology of mental disorders can be addressed at multiple interacting levels. 13 Ecological and social factors certainly play a causal role, and many disorders can be triggered solely by environmental stressors or injuries. Nevertheless, estimates suggest a moderate to high degree of heritable risk (e.g., 90% of trait variation for autism can be accounted for with genetics; bipolar disorder, 85%; schizophrenia, 81%; unipolar depression, 37% 14 –16 ). This indicates strong genetic components underlying vulnerability to mental disorder. Over evolutionary time, heritable risk would have been responsive to pressures of natural selection removing alleles associated with disorder from the population. In addition, age of onset is often prior to or during peak reproductive years, 16 further increasing fitness costs associated with many disorders (e.g., reduced number of offspring). These facts have led some to question the so-called paradox of psychiatric disorders 16 –20 : given that these disorders are considered maladaptive and have heritable risk, why do they still exist? Explanations fall into 2 categories: despite and because of natural selection (Table 1).
Why do mental disorders exist and persist?a
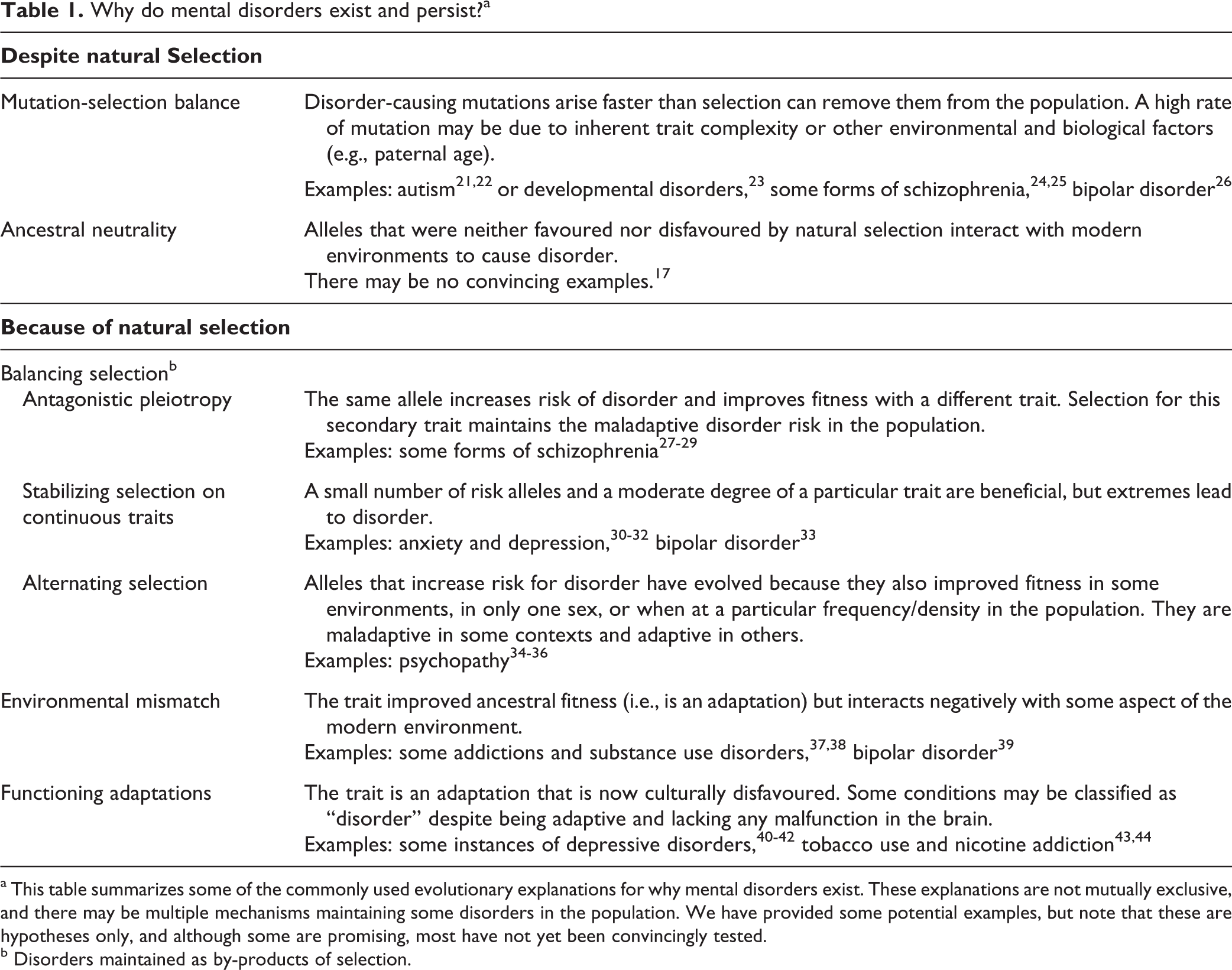
a This table summarizes some of the commonly used evolutionary explanations for why mental disorders exist. These explanations are not mutually exclusive, and there may be multiple mechanisms maintaining some disorders in the population. We have provided some potential examples, but note that these are hypotheses only, and although some are promising, most have not yet been convincingly tested.
b Disorders maintained as by-products of selection.
Disorder despite Natural Selection
Heritable risk for mental disorders may persist in populations despite the pressures of natural selection. First, mental and behavioural traits are complex and polygenic. With so many potential sources of error, new deleterious mutations may arise as fast or faster than natural selection can remove them (mutation-selection balance). 17 –19,45 A greater mutation load, for example, because of inbreeding, 46 maternal famine, 47 or older paternal age, 48 may increase an individual’s risk of schizophrenia, 24,25,46 autism, 21,22 other developmental disorders, 23 and bipolar disorder. 26
Second, preexisting genetic variation may have only recently have started contributing to disorder. Ancestral neutrality explanations propose that modern humans exist in environments critically different from those in which we evolved. In this view, ancient alleles interact with novel environmental factors to cause disorder, and too few generations have passed for natural selection to remove these alleles from the population. 17,49 Theorists may cite such changes as modern diets, pollution, or decreased social connectedness. This explanation is congruent with the greater prevalence of some disorders in industrialized nations 50 and among individuals using evolutionarily novel substances (e.g., cannabis and psychosis 51 ). However, ancestral neutrality may be unlikely to solely account for the high heritability and prevalence of most disorders. 17 Because successive generations consist of only a sample of prior alleles, over time random genetic drift will tend to fix or eliminate neutral alleles from the population, reducing neutral variation. Furthermore, modern fitness costs are typically great enough to remove risk alleles from the population in only a few dozen generations. 17,20 Thus, if a disorder had originated because of ancestral neutrality alone, its prevalence should now be declining rapidly.
Disorder because of Natural Selection
More nuanced applications of evolutionary theory suggest many non–mutually exclusive ways that heritable risk for disorder can persist because of natural selection 16 –18 (Table 1). A common misconception is that natural selection leads to perfectly designed traits. 12 In fact, natural selection responds to trade-offs to find the best compromise for the propagation of genetic material. Selection for one trait can maintain risk for disorder as a by-product. Explanations of this kind fall under balancing selection, named for the balancing of positive and negative selective forces that maintains allelic variation. One mechanism is antagonistic pleiotropy, when a single allele increases susceptibility to disorder but also confers some benefit. Positive selection for the beneficial trait cancels out negative selection against increased disorder risk. Another mechanism of balancing selection is heterozygote advantage. In this case, individuals with one risk allele and one healthy allele have greater fitness than both homozygotes. Commonly cited examples of single-gene heterozygote advantage are sickle-cell anemia 52 and cystic fibrosis, 53 wherein heterozygous individuals may benefit from increased resistance to malaria and tuberculosis, respectively. For polygenic psychological traits, a moderate number of risk alleles may increase fitness while too many leads to disorder. Anxiety, depression, and bipolar disorders may all be examples in which trait extremes are maladaptive yet intermediate phenotypes are beneficial. 30 –33 Genetic evidence suggests that there may also have been benefits to alleles that increase risk for schizophrenia, 27 such as higher IQ, increased creativity, and improved mathematical reasoning. 28,29 Future research should rigorously test these ideas.
Fitness benefits need not exist at all times or for all individuals. Under alternating selection, natural selection vacillates between favouring and disfavouring an allele. A special case is sexual antagonism, in which alleles confer fitness benefits in one sex but costs in the other. Some possible evidence for this exists for schizophrenia and autism, in which estimated fitness costs are greater among affected males than females, and sisters of affected individuals may have increased fitness. 20 Other cases of alternating selection are frequency- or density-dependent selection, in which the strength and direction of selection depend on the relative frequency of the allele or population density. For example, some personality traits may be alternative ecological strategies that conferred fitness benefits depending on the environment and strategies expressed by others. 9,34,54,55 For example, antisociality and psychopathy may represent biases toward selfishness that pay off when most others are eager to cooperate. 54,34,56,57 If true, natural selection would maintain heritable variation such that a small proportion of the population expresses such traits. This perspective has generated some debate, 35,58 although empirical research has largely supported the hypothesis that psychopathy is an adaptation. 36,59
These examples highlight the fact that some current disorders may be the direct result of evolved adaptations interacting negatively with modern environments: environmental mismatches between modern environments and the environments for which we are designed. It has been suggested that bipolar disorder may be one example. 39 The reward system of the brain is an adaptation that may be particularly susceptible to environmental mismatches, leading to addictions and substance use disorders. 37,38 Furthermore, research suggests that humans may have evolved to exploit neurotoxic properties of some plant secondary compounds (e.g., nicotine) to fight parasites such as helminthic worms. 43,44,60 Although it remains to be seen whether similar adaptationist accounts apply to the use of other plant-derived substances, the heritable genetic variation underlying such substance use would have been directly maintained by natural selection because of its historical adaptive value. Indeed, the “normal” functioning (as designed by natural selection) of some adaptations may still be adaptive in modern environments but nevertheless classified as “disorder” because it causes distress or is culturally disfavoured. For example, anxiety may prevent accidental death in early life, 61 and depression may be due to adaptive mechanisms that reduce interest in otherwise pleasurable pursuits to conserve energy, signal social defeat, or promote focus on solving complex problems. 40 –42,62 Indeed, controlling for comorbidities, depressive disorders may increase fitness in women. 20 The implications of this perspective to our current understanding of disorder are the subject of the next section.
Psychiatric Nosology and an Evolutionary Understanding of Disorder
Some conditions or behavioural syndromes currently classified as mental disorders may have originated as adaptations (i.e., traits that historically served a particular function to increase fitness) and thus may occur as the result of “normal” functioning rather than any biological malfunction (e.g., mutation, developmental aberration, or failure of underlying mechanism). In the Diagnostic and Statistical Manual of Mental Disorders (DSM) system (III, IV, and 5), distress and impairment are required to define disorders that warrant intervention. The DSM-5 defines mental disorder as “dysfunction in the psychological, biological, or developmental processes underlying mental functioning.” 63(p20) and operationalizes this dysfunction with proxies such as the inability to work, maintain interpersonal relations, and take care of one’s self. Several authors have pointed out the difficulty this approach can have in distinguishing between normal and abnormal behaviour. 5,64 –67
Distress, impairment, and inability to function in everyday life are not necessarily indicative of biological malfunction. 2,62,64,68 –70 The normal functioning of the body’s evolved systems can at times be unpleasant and cause suffering. Examples include feeling nauseated or having diarrhea after ingesting rotten food, running a fever when infected, and the physical pain associated with a broken limb or childbirth. The inappropriate or indiscriminate disruption of these adaptations in an attempt to relieve suffering can have negative consequences. 71 –73 Conversely, the absence of distress can indicate disorder. For example, individuals with a congenital inability to feel pain are much more likely to suffer injury and early death. 74 These insights suggest that distress is a faulty criterion, and the DSM system must therefore erroneously categorize some “normal” states as disorders and miss some instances of psychological malfunction that are not distressing.
Incorporating an evolutionary perspective may clarify the distinction between normal and disordered and improve psychiatric nosology.
5,62,68,69,75
Jerome Wakefield
75,76
has proposed that we consider as disorders only such conditions caused by “harmful dysfunctions:” A condition is a disorder if and only if (a) the condition causes some harm or deprivation of benefit to the person [or others] as judged by the standards of the person’s culture (the value criterion), and (b) the condition results from the inability of some internal mechanism to perform its natural function, wherein a natural function is an effect that is part of the evolutionary explanation of the existence and structure of the mechanism.76(p384)
Applying this approach to human behaviour has been criticized for relying too heavily on speculations of adaptation (i.e., “just-so” stories). 66,79 It is true that accurately identifying adaptations may require decades of research, and hypotheses may abound in the interim. However, hypotheses guide research, and such a framework allows the distinction between conditions caused by biological malfunction (true “disorder,” errors of mechanism) and those due to undesirable or out-of-context adaptations. For each supposed instance of disorder, we must propose the normal function that has gone awry. Until known and convincingly tested, the classification of a condition as disorder or nondisorder should remain tentative. This is more than semantics. Knowing whether a harmful condition is caused by the natural functioning of an adaptation or the breakdown of an adaptation leads to different models of illness, different directions of research, and, most importantly, different approaches to treatment. For the example of fever, there are very different treatments for a fever caused by the normal functioning of the immune system in response to infection and for a fever caused by hypothalamic tumor. The current approach to psychiatric nosology does not differentiate between “functional” and “dysfunctional” routes to distress and impairment. 62 The incorrect assumption of brain malfunction may lead to improper and ineffective treatments that do more harm than good. 80,81
As research from this perspective progresses, it leads to an ever-increasing understanding of the brain’s many adaptations. A list of brain adaptations is, in effect, a list of ways the brain may malfunction. This can improve disorder nosology by categorizing conditions according to etiology (which adaptation has malfunctioned) instead of behavioural symptoms. There may be many pathways to the same behavioural syndrome, and clustering categories of disorder based solely on observable symptoms combines cases with unique etiologies that ought to be treated by different means. Alternatively, a single underlying malfunction may present with different symptoms that can be erroneously classified as comorbid disorders. Currently, comorbidity is common. In one study, 61.8% of patients receiving a diagnosis of depressive disorder were also diagnosed with at least one other comorbid psychiatric disorder (e.g., anxiety, posttraumatic stress disorder, eating disorders, or obsessive-compulsive disorder). 82 Frequent overlap between conditions may suggest that the two can in fact be caused by one underlying mechanism. 5 Understanding comorbidity and parsing apart different conditions according to etiology will require more fully understanding the underlying adaptations that have gone awry.
Conclusion
Natural selection is the only scientific explanation for the origin of the brain
Footnotes
Acknowledgements
We thank Dr. Skye Barbic and 3 anonymous reviewers for comments on the manuscript.
Author Note
Dr. Durisko wrote the first draft of this article, and Dr. Mulsant, Dr. Andrews, and Dr. McKenzie provided critical revisions.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.