
Abstract
Objectives:
To extract the themes pertaining to prudent psychiatric practice from written court judgments in Canada.
Methods:
We searched the medical and legal literature for cases involving civil litigation against Canadian psychiatrist and reviewed all available written judgments. We completed a thematic analysis of the civil actions against psychiatrists as conveyed by those written court judgments. We classified the cases according to the disposal status and the essential lessons from the decisions on standard of care and practice by Canadian psychiatrists.
Results:
Forty such cases were identified as involving psychiatrists over a 45-year period. A subgroup included those dealing with limitation periods and disclosure applications. Thirty of the 40 cases (75%) were decided in favour of the defendant psychiatrists, including 2 dismissed for running over the limitation period. The cases that actually went to trial suggest that documentation and obtaining second opinions are protective against claims of negligence. Inpatient cases resulting in successful litigation against psychiatrists involved fatal outcomes, but not all fatal outcomes led to successful litigation.
Conclusions:
The key lessons from these cases are the importance and relevance of regular best clinical practices, such as documentation, obtaining second opinions, following guidelines, and balancing competencies in the expert and manager or advocate roles. Incorporating these practices should allay concerns about litigation against psychiatrists.
Introduction
Defensive psychiatric practice, which realistically defends no one, may stem from many factors: anxiety about bad clinical outcomes (death or injury); exaggerated ideas about risk; and the like. Inescapably, adverse outcomes are not uncommon in both medical and psychiatric practice. The problem of assessing actual risk is heightened by the absence of a review of psychiatric malpractice cases in Canada. 1
In addition, the role of litigation on, and the purpose of, the liability system continue to be debated. 2 During a 5-year study period, the average physician incurred twice the claims, compared with a previous 5-year period, with greater claims against surgeons and gynecologists. 3 Although the Canadian medical liability system, like others, is conceptualized as a pathway for ultimately improving health care, the physician going through a malpractice suit can experience significant financial, emotional, and professional distress. 4 Litigants themselves are not spared the negative emotional consequences of civil litigation. 5 Litigation, it has been said, is not for the faint hearted.
In fact, compared with all medical specialties, psychiatric malpractice claims, compensatory damages, and payout rates are among the lowest. 6 However, the rates of claims brought against psychiatrists in the United States increased from a mere 0.3% of all 71 788 claims in the 1960s to 6% of cases in the 1990s. 7,8 Comparable figures are not currently available in Canada. Canadian psychiatrists are affected by the rising trend in litigation especially related to psychiatric pharmacotherapy and inpatient suicides. 9 –12 By seemingly providing the standard by which a colleague’s practice can be judged, proliferation of clinical practice guidelines, by setting high standards, may increase fears of litigation without a sound basis; in the Canadian context especially, psychiatrists have been labelled as running scared. 1,13 Psychiatrists also seem at increased risk of disciplinary actions, 14 with a 2-fold higher rate among disciplined psychiatrists compared with other specialists. 15
We undertook to study the lessons to be gleaned from the Canadian courts on the subject of psychiatric malpractice. By reviewing the cases through the eyes of the courts, we hoped to gain an understanding of how the Canadian legal system views the roles of psychiatrists and their practice.
Methods
We conducted a search of the legal literature and online resources including the Google search engine using the term “psychiatric malpractice,” “defendant psychiatrist,” “litigation against psychiatrists,” “Canada,” and “Canadian.” We attempted to get access to the list of cases with the Canadian Medical Protective Agency (CMPA), but to no avail. Access to the limited cases over the last 45 years was primarily gained through Westlaw, Quicklaw (LexisNexis), and the Canadian Legal Information Institute (CanLII) search engines. The criteria for inclusion of the decisions were: having a written judgment from the courts (lower and upper), and a psychiatrist as a defendant in a civil case. By consensus of the authors, judgments that failed to meet the criteria were excluded. Written judgments were reviewed as to portrayal of negligence based on the standard of care. Factors—including case identifying information, material facts and issues, level of court decision, whether the patient was in or out of hospital, and the final decision rendered (liable, successfully defended, or dismissed)—were compiled in table form for analysis. The table of all the cases is available online or on request from the authors. The decisions were placed into 2 categories: 1) cases concerned with interim applications; these included breach of limitation periods, where cases were not filed in a timely manner, and applications for summary judgment, that is, judgment for one side without a full trial; 2) cases in which trials and appeals were completed with findings.
Results
Forty civil cases between 1966 and 2012 with written judgments were identified from the search results. This cohort excludes jury-only decisions that were not appealed and an unknown number of cases that were settled before trial especially under the auspices of the CMPA. The trend resembles a dome-shaped curve with a spike in the 90s and decreasing numbers on either side of the peak. Eighteen cases (45%) formed the peak identified between 1990 and 2000. The rate of successful suits against psychiatrists was 17.5% of all cases (Figure 1). The size of damage awards settlements published in the judgments ranged from Can$20 000 to $187 000. These results average to about 1 malpractice claim per year and 1 successful case every 6.5 years.
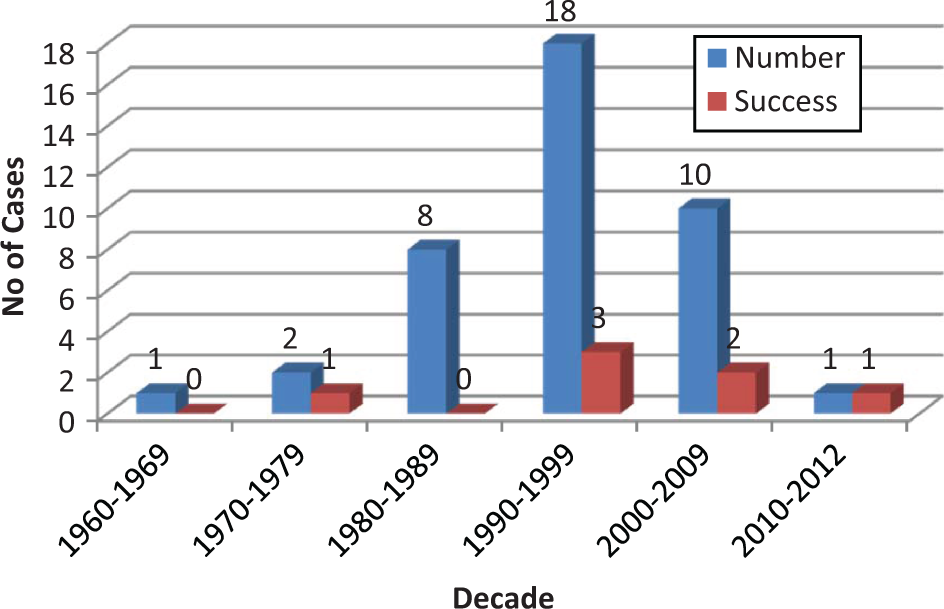
Number of litigation cases (with number of successful ones) involving psychiatrists per decade (1966 to 2012).
Successful and Unsuccessful Cases
Cases dismissed for breach of the limitation period were categorized as in favour of the defendant psychiatrist, as there was no finding of liability. Thirty of the 40 cases (75%) were judged as successful for the defendant psychiatrist. In the completed trial category, 23 of the 30 cases were again judged as successful for the defendant psychiatrist (Table 1). Among the successful 23 cases, 43.5% of the sued psychiatrists obtained another colleague’s opinion, compared with only 14% in the unsuccessful cases. Defendant psychiatrists were found liable on these bases: fraudulently concealing information, breach of fiduciary obligation by engaging in business dealings with a patient, a fatal outcome from suicide, dangerous driving under the withdrawal effect of medications, and abusive behaviour toward patients. A finding of liability involved the case of a homicide committed by a patient 51 days after being decertified.
Litigation cases divided according to the decision favouring the defendant psychiatrist or the plaintiff (1966 to 2012).
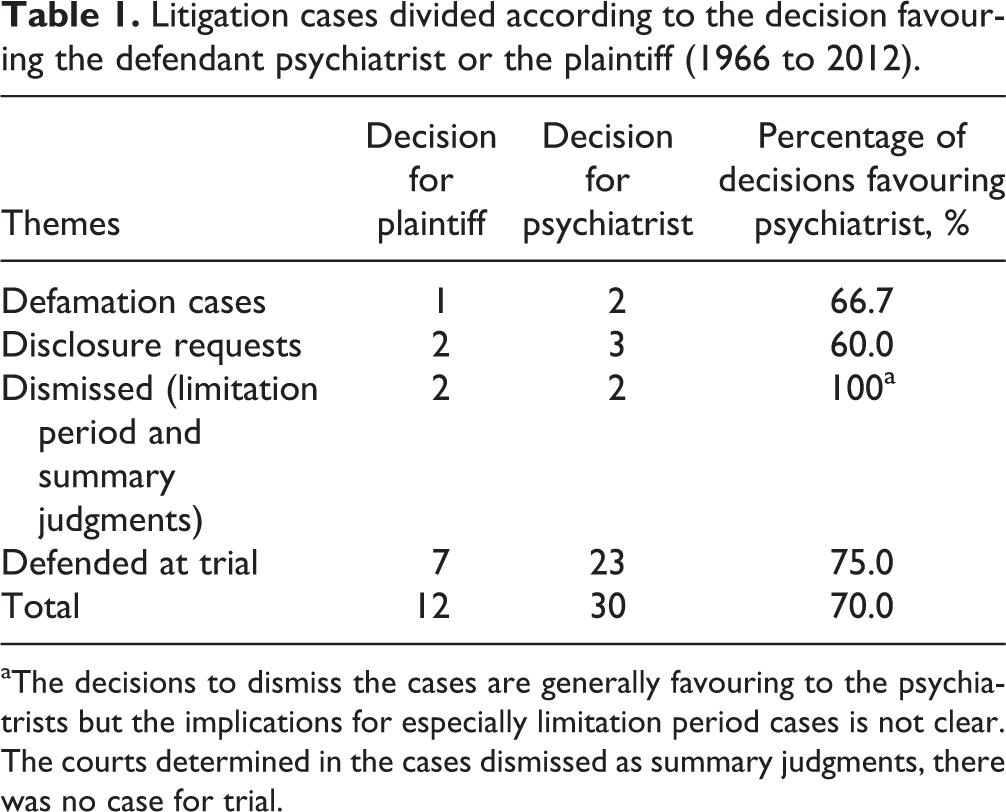
aThe decisions to dismiss the cases are generally favouring to the psychiatrists but the implications for especially limitation period cases is not clear. The courts determined in the cases dismissed as summary judgments, there was no case for trial.
Administrative Cases
Five of the total cases (12.5%) involved requests made to access information. In a 1997 case, AM v. Ryan (1997), a defendant in a civil suit with a patient sought disclosure of the patient’s treatment record with a second psychiatrist. Following several appeals on the matter, the Supreme Court of Canada (SCC) ruled that the application should be allowed, so that the information could be viewed in camera (in the judges’ private chambers rather than in open court). In a slightly different case, Smith v. Jones (1999), a psychiatrist completing a risk assessment on a dangerous patient sought to disclose the information about that dangerousness to authorities. The SCC identified the circumstances under which a psychiatrist may disclose such information; namely, when the risk to identified people of serious harm or death is clear and imminent (implying a sense of urgency). While the issue of a duty to third parties (beyond patient and doctor) was addressed in this case, the level of detail offered was minimal and cursory.
In a 1984 case, LDF v. A psychiatrist (1984), the material issue was one of discovery and privilege. The SCC offered very little guidance while granting the interim order for disclosure. Two other disclosure cases about sexual histories of the plaintiffs came out differently: in Doe v. Hirt (1993), the British Columbia Supreme Court denied disclosure pending further investigation; in GAB v. Sampath (1999), the Newfoundland Supreme Court granted disclosure.
Dismissal by Limitation Period
Two Ontario claims (Cascone v. Rodney [1982] and Berger v. Benchitrit [2002]) for involuntary hospitalization and alleged negligent use of drugs respectively were dismissed as filed after the expiration of the limitation periods (time line for the civil action to be filed).
Defamation Cases
Three defamation cases were identified. In Kravit v. Dilli (1998), the British Columbia Supreme Court dismissed a claim that part of a psychiatric report contained defaming information. The information was considered privileged, as it appeared in a judicially ordered report. The Walton v. Walker (1990) defamation case was also dismissed. This was due not to the expiration of the limitation period but due to the plaintiff’s delay of almost 2 years in taking the next step. In Golley v. Mansfield (1989), the British Columbia Supreme Court granted damages of Can$20 000 in a defamation case brought against a psychiatrist by a nurse.
Summary Judgment and Dismissal of Cases
In 2006 a patient, Benson, claimed false imprisonment against a psychiatrist who admitted him to a Manitoba hospital under the applicable Mental Health Act. The claim was dismissed pursuant to a summary judgment application, as the Mental Health Act provided a good faith defense. Kurdina v. Gratzer (2009), involving a claim of negligence (wrongfully diagnosing schizophrenia) was similarly dismissed. The patient’s nonpsychiatrist expert instead diagnosed the effects of psychotronic rays.
Other Observations
A bad outcome does not equal a successful litigation as epitomized in University Hospital (Alberta) v. Lepine, [1966] in which the Judge commented that “negligen[ce] must be judged not by its consequences alone but also by considering whether a reasonable person should have anticipated what happened…” The courts are also more likely than not to grant requests for access to psychiatric records.
Discussion and Recommendations
Since 2000, the number of court litigated cases has been trending downward. This trend suggests that less malpractice is being found and that successful psychiatric liability claims are decreasing in Canada. The trend may also be a reflection of a less litigious society; a product of the checks and balances embedded in the health system; a result of better representation by the medical defense agency (CMPA); or even an expression of defensive psychiatric practice. Over the last 2 decades, efforts to improve care of psychiatric patients (effective treatments, fewer side effects, family-centred suicide prevention, a recent application of apology principles) may decrease malpractice in general and court litigated cases specifically. 16,17
Consequences considered, finding psychiatrists liable in only 17.5% of the written judgments is reassuring when compared with 39% in other studies, 18 though the figures are higher in cases involving completed suicide. 12,16 –18 The outcomes depend in part on how many claims proceed to trial. Excluding cases settled out of court, 80% of claims proceeded to trial, compared with 75% of claims against 107 US psychiatrists paid out and settled before trial. 19 Since 75% of Canadian cases going through the courts were successfully defended, psychiatrists may feel some relief; unfortunately, new categories of claim are just beginning to emerge, involving side effects and metabolic syndrome. 8 Avoiding complacency through prudent practice is still advisable, even though—in a 10-year US study of 2000 medical malpractice cases—psychiatry was considered a low frequency risk category, compared with other specialties. At a rate the authors calculated as 1.5 claims per 100 psychiatrists per year, psychiatrists could be expected to be sued every 12 years. 6 We found payouts to be much less than are usually reported in the United States 18,20 and Europe. 21 Payouts to plaintiffs vary depending on the medical specialty, level of health care spending, capping policies, out of court settlements, compensatory models and severity or extent of injury in malpractice, and the reasonableness of the trier of fact. 1,18,22,23
We are aware that the cases reviewed are but a part of the total cases representing the views of the legal system on psychiatric practice. However, these written judgments represent an important record of courts’ views of clinical practice and the components of malpractice (duty, damage, dereliction of duty, and direct causation) which had to be established by psychiatric expert witnesses. 1
In determining the standard of professional practice to be met, the Ontario Court of Appeal in Ahmed v. Stefaniu (2006) clarified the concepts of “honest and intelligent exercise of judgment” and the meaning of a “reputable body of opinion within the profession” even if in the minority. 1 To ensure consistency in determining negligence, the correct benchmark, achieved through expert training, should be applied. This indirectly regulates the standard of practice of psychiatry and by extension contributing to an anxiety-free standard of care. 24 We suggest that high standards of training, emphases on core competencies and the introduction of the forensic psychiatric subspecialty, give psychiatry the best chance, not only of improving standards of practice, but also of prevailing in suit.
Previously, the main causes of claims 25 were: complications of electroconvulsive therapy, complications of psychotherapy, suicide, side effects of psychotropics, lack of informed consent, and diagnostic problems. In Canada, high priority has not been given to the duty to third parties as created by the cases following the Tarasoff 26 decision in the United States. The Alberta case of Wenden (1991) is the closest that the Canadian Courts have come to finding that a psychiatrist owed a duty of care to third parties (that is, the patient’s victim beyond the patient). By establishing the standard of care as reasonable care and skills rather than perfection, the guidance of the courts is anchored on establishing foreseeability.
Safety in Numbers
Involvement of more than one psychiatrist, a proxy for a second opinion in 46% of claims, may have contributed to the successful outcome. Obtaining a second opinion in cases, especially complex ones, should go a long way in confirming that the standard of care has been met. 27 In Wenden (1993), a patient was seen by a nonsued psychiatrist just before leaving the hospital. He drove and crashed his car. The fact that a second psychiatrist saw him was drawn out by the Alberta Court of Appeal as sufficient to meet the standard of care. This position, unfortunately, is not foolproof: the defendant psychiatrist in Ahmed v. Stefaniu (2006) was found liable; this occurred despite the Court’s acknowledging that the psychiatrist had obtained second opinions on the case before the tragic outcome and that this was good practice; a number of factors—including the duty owed to the deceased relative of the patient, jury involvement, and the demeanor of the defendant psychiatrist may have played a more determinative role in that verdict. Psychiatrists should feel comfortable in seeking second opinions in certification, diagnostic difficulties, cases resistant to treatment, and decertification. 28 Managing countertransference toward patients should be facilitated by seeking the opinion from a neutral and objective colleague. By discussing cases with their preceptors, trainees are protected through obtaining second opinions; however, the law may hold supervisors vicariously liable in some cases. 29
Documentation
Documentation in our review presented 2 faces: on the one hand, the psychiatrist is often protected by the evidence of the record; however, plaintiff access to the same records could confirm negligence. Objective and nondefamatory documentation is critical, given the patients’ right to access the information. With electronic medical records storage of records is less of an issue. It is also important that contemporaneous notes are made at the time of the consultation and not long afterwards. Canadian courts have indicated that clinical notes essentially provide more credible and reliable information than memory. Ten years after a medical encounter, the Judge in Melanson (2008) ascribed more weight to the doctor’s notes and concluded that the evidence was reliable as they were written at the time of the relevant events, 10 years earlier. Similarly, in the British Columbia claim against a psychiatrist for not warning a patient of the potential side effects of lithium (Chancey [2000]), the Judge dismissed the claim by relying more on the notes taken before the claim than the ‘self-serving’ testimony of the psychiatrist.
System-Related Problems
Psychiatrists face real conflicts when balancing their competency roles as managers of limited resources and advocates for their patients especially when the former contributes to deficient care. In Ahmed v. Stefaniu (2006), for example, hospital staff had pressured for the patient to be discharged. This fact was thought to have played a role in the jury’s decision. Being overworked is at least mentioned in one negligent decision. Related to these conflicts are the complex and sometimes heated debate on work hours and medical errors associated with 24-hour duty schedules. 30,31 Matters, such as professional burnout and medical errors resulting from sleeplessness, continue to be debated. 32 Like boundary violations, ethical considerations should lead individual psychiatrists to decide on how much work they are prepared to take on from their employers. 33 Obviously, refusal to work can lead to conflicts with the employer, but overwork can contribute to a finding that the doctor did not meet the standard of care expected.
Evidence-Based Practice
To change the sometimes nebulous and imprecise nature of psychiatric care, clinical guidelines grew rapidly. Proliferation of clinical guidelines, which include divergent but acceptable therapeutic techniques, has implications. Apart from conflict of interest claims with guideline authors, guidelines provide only an approximation of the standard of care. 34 –36 Unfortunately, the slow rate of development and the absence of numerous guideline topics may result in unclear standards of care; this lack of clarity, rather than the guidelines themselves, has been suggested to increase claims against psychiatrists 37 when present. Note that, in general, guidelines are seen as addressing best practices, not the average practice defining standard of care. 37
Confidentiality
In Smith v. Jones [1999], the psychiatrist was given permission to release confidential information. Even though the case also involved the higher standard of solicitor–client confidentiality, the case may have some relevance to day-to-day psychiatric practice. In the obvious cases requiring reporting, the conflict between confidentiality and disclosure is not of concern. However, in grey areas we recommend innovations in policies 38 and a sequential decision paradigm similar to innovations in the beneficience–autonomy debate 39 : psychiatrists may want to consider any breach based on their conscience as the first priority, followed by colleagues’ expected practices, stipulations of regulatory agencies (College of Physicians and Surgeons), and Court decisions.
Other Nonclinical Matters
Liability may depend, not on actual negligence, but on jury selection and the defendant psychiatrist’s display of humanity, humility, and reasonableness when taking the stand. 1 We offer some advice for consideration deriving both from the case said to have Canadian psychiatrists scared and our in-depth reading of some successful cases. Consultation with ethicists and legal support especially from CMPA are additional protective steps. In many jurisdictions, an Apology Act has resulted in doctors being allowed to apologize and express regret at adverse consequences, without that apology becoming admissible against the contrite doctor. Apologies may deter bringing a claim in the first instance.
Conclusions
The court decisions on psychiatric malpractice in Canada are few and favourable. As determination of the standard of care is ultimately the prerogative of the expert psychiatrist, educating ourselves in the profession to practice prudently while striving for objectivity and honesty, will limit the problems identified above. Conforming to the standard of care is both beneficial for the patient, the psychiatrist, and the system at large. The lessons learned (confidentiality, documentation, and obtaining second opinions) can be seen as the essential ingredients of daily practice. As such, no new skills are needed, and there is no objective needed for anxiety in daily practice.
Footnotes
Authors’ Note
Presentation of 45 years of civil litigation against Canadian psychiatrists. Presented at the Canadian Academy of Psychiatry and Law Feb 2010, Banf, Alberta, Canada and Department of Psychiatry Grand Rounds presentation April 2013, Saskatoon, Canada.
Acknowledgment
We will like to thank Sudheej Krishnan, PhDC, who painstakingly provided the administrative component of completing this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.