
Abstract
Objective:
Community treatment orders (CTOs) exist in more than 75 jurisdictions worldwide. This review outlines findings from the international literature on CTO effectiveness.
Method:
The article draws on 2 comprehensive systematic reviews of the literature published before 2013, then uses the same search terms to identify studies published between 2013 and 2015. The focus is on what the literature as a whole tells us about CTO effectiveness, with particular emphasis on the strength and weaknesses of different methodologies.
Results:
The results from more than 50 nonrandomized studies show mixed results. Some show benefits from CTOs while others show none on the most frequently reported outcomes of readmission, time in hospital, and community service use. Results from the 3 existing randomized controlled trials (RCTs) show no effect of CTOs on a wider range of outcome measures except that patients on CTOs are less likely than controls to be a victim of crime. Patients on CTOs are, however, likely to have their liberty restricted for significantly longer periods of time. Meta-analyses pooling patient data from RCTs and high quality nonrandomized studies also find no evidence of patient benefit, and systematic reviews come to the same conclusion.
Conclusion:
There is no evidence of patient benefit from current CTO outcome studies. This casts doubt over the usefulness and ethics of CTOs. To remove uncertainty, future research must be designed as RCTs.
The Community treatment order (CTO) has over the last 4 decades or so become a preferred clinical and policy solution for addressing nonadherence with treatment on the part of patients with severe mental illness who, in the era of deinstitutionalization, are largely treated in the community. 1 By making adherence to treatment a legal requirement, CTOs are intended to prevent repeated relapse leading to frequent readmission, thus breaking the revolving door cycle that make these patients’ lives very difficult. The idea is that a period on CTOs would help patients achieve stability and engage in treatment, while also reducing risks to them and their community. CTOs may also provide a less restrictive alternative to hospitals. 2
Provisions for CTOs now exist in mental health legislation in more than 75 jurisdictions worldwide, 9 of which are Canadian provinces. From the 1980s onwards, most states and provinces in the United States and Canada introduced CTOs. 2 In Australia and New Zealand, CTO legislation was passed in the late 1980s or early 1990s. As in Canada, CTOs there are initiated by clinicians, while in the United States, CTOs are usually made by the court on the application of clinicians. 3 Clinician-initiated CTOs exist in some European countries, including Scotland, Sweden, Denmark, Norway, England and Wales, and Switzerland. CTO regimes differ regarding the length of the order (though 6 months is common), the threshold for compulsion, whether patients must have a history of readmissions or nonadherence, and whether they must be an involuntary inpatient to qualify for a CTO. 3
Even if their use varies considerably between service catchment areas and over time, in general CTOs seem to be used more frequently by services in Australasia than in North America, with the more recent UK regimes falling between. Usage also varies between individual psychiatrists. In the United Kingdom, for example, a recent survey found that some psychiatrists never used them, while others had used them more than 100 times. 4 While this may to some extent reflect differences between services and caseloads, it does seem to suggest that the application of this law is shaped, at least in part, by personal opinion.
The introduction of CTO legislation to a new context is often preceded by significant debate about whether it is ethically justifiable to restrict the liberty of adults with decision-making capacity who have not broken any law. More recently the debate has focused on whether CTOs provide clinical benefits. Some have raised concern about a lack of evidence for a practice that is increasingly widespread. 5 The aim of this article is to provide an overview of existing evidence for clinical and social outcomes of CTOs.
Method
To date, close to 200 empirical articles on CTOs have been published, and, of these, around 80 report quantitative outcome analyses. Only three RCTs have so far been reported. Most existing outcome studies have been subject to systematic review: those published prior to 2006 by Churchill et al, 2 and those from 2006 to 2013 by Maughan et al. 6 In this article, I draw on the findings from these reviews plus the existing meta-analyses. Additionally, the search terms used in both reviews (details published elsewhere 6 ) was repeated in May 2015 in PsycINFO, MEDLINE, and EMBASE to include in this analysis studies published since 2013. Nineteen papers of relevance were identified (some from hand searching).
As the main focus here is on the effect of CTOs on patient outcomes, I will only very briefly discuss the descriptive literature. Also, as detailed descriptions of the outcome studies are available in previous reviews, I focus here on the big picture: that is, what the literature as a whole tells us about CTO effectiveness. Particular attention is given to randomized controlled trials (RCTs) and meta-analyses as they provide the most robust evidence.
Results
Descriptive Studies
Local studies of the views and experiences of patients, clinicians, and family members conducted in the United States, Europe, or Australasia show a very similar picture to that reported from Canada. 7 Clinicians prefer to have CTOs available as an option 8,9 and many believe CTOs have the desired effects. 10,11 Family members often find CTOs necessary or helpful 12 but are concerned that the order is insufficient to help patients lead better lives, and that other community services must also be offered. 13,14 Patients reportedly hold mixed views. Many find some aspects of the order helpful, while other aspects restrict their lives in ways that can be highly problematic. 13 –18 The highest priority for all 3 groups is usually to avoid hospital admission. 16 It is worth noting that the experienced advantages of CTO often are expressed by way of comparison with detention in hospital, not with receiving comprehensive community services voluntarily.
Descriptive studies from around the world demonstrate that, despite some differences in legislation, CTOs are used for the same group of patients. Around two-thirds are male, their mean age is around 40 years, they tend to be diagnosed with schizophrenic disorders, and have a history of nonadherence and multiple admissions. Many misuse substances, are single, self-neglecting, relatively isolated, and have a history of violence or criminal offences. 2
Types of Outcome Studies
It is generally accepted that RCTs, systematic reviews, and meta-analyses top the hierarchy of evidence in medicine. By randomly allocating patients to treatment under a CTO or to a control condition, RCTs reduce the effects of bias, inadequate matching, and regression to the mean. Defining the hypotheses and outcome measures a priori, as RCTs do, also reduces the risk of false-positive findings (type 1 error). Systematic reviews provide comprehensive and structured overviews of a field of research, and meta-analyses pool data from RCTs and other high-quality studies, increasing statistical power and generalizability. Only a small number of studies, however, investigate CTO outcomes with such a high level of rigour: 3 RCTs, 19 –21 2 systematic reviews, 2,6 1 Cochrane review, 22 and 2 meta-analyses. 23,24
Most published outcome studies to date use nonrandomized methods. They are mainly controlled before-and-after (CBA) studies with matched non-CTO control subjects, uncontrolled before-and-after (UBA) studies where the patient’s clinical status is compared before and after being placed on CTOs, or epidemiological studies that observe, but do not match, CTO and non-CTO populations. Well-designed, nonrandomized studies can produce insights about associations between CTOs and outcomes. There are potential methodological obstacles that limit their generalizability, however, which are exacerbated by small sample sizes. Nonrandomized designs, and particularly UBA studies, are vulnerable to service changes over time (for example, closure of beds). CBA studies may be confounded by problems in adequate matching of patient characteristics (for example, illness severity) and UBA studies may be confounded by regression to the mean. Studies using routine administrative data have the potential advantage of including data on all CTO patients in an area or jurisdiction, thus avoiding selection bias, but they are at the mercy of the quality of the registers they use. They also have the potential to test multiple hypotheses, so strategies for reducing the likelihood of false positives are required.
The outcomes most frequently measured in CTO studies (regardless of methodology) are readmission rates, time in hospital, and use of community services. Other outcomes, such as number of admissions, time to readmission, medication possession, adherence, victimization, arrest, mortality, quality of life, and perceived coercion have also been measured. However, there is a lack of consistency across studies as to the outcomes included and how they are measured. 25
What Review Studies Find
The largest systematic review to date was conducted by Churchill et al 2 and included 72 articles published before 2006. Among these, 28 reported outcome analyses (2 RCTs, 6 CBAs, 5 UBAs, 14 exploratory analyses, and 1 Cochrane review) from 9 different studies. Two articles were not published and a further 2 were flawed so that differences between groups were not estimable. These 4 are excluded from the present review. None of the 9 studies showed evidence suggesting that CTO kept patients out of hospital, reduced length of stay, or improved compliance. There was also no evidence for “any effect of CTO on social functioning, arrests, homelessness, general mental state, psychopathology, quality of life, carer satisfaction, or perceived coercion.” 2, p 179 Some small local studies, 26 –30 all reporting improved patient outcomes, were excluded in Churchill et al’s review given their naturalistic, retrospective design, combined with very small sample sizes (from 25–70 ). 2
A more recent systematic review by Maughan et al 6 included 18 articles (1 RCT, 9 CBAs, 6 UBAs, and 2 epidemiological) from 11 studies or registers, published from 2006 to 2013. These showed more mixed results, but the authors still concluded that there was no evidence that CTOs led to improvements in readmissions, length of stay, or use of community services.
When repeating the search from those previous reviews to identify outcome studies published since 2013, 19 articles were identified, 9 of which reported on the outcomes described in Table 1 (6 UBAs, 1CBA, 1 epidemiological, and 1 meta-analysis). One article reported secondary outcomes from an RCT. 31 The remaining 9 papers 32 –40 reported on a wide range of other outcomes (for example, medication, access to secondary services, and mortality), with mixed, but largely negative, results as to CTO benefit.
Study by outcome from UBAs, CBA, RCTs, and meta-analyses.
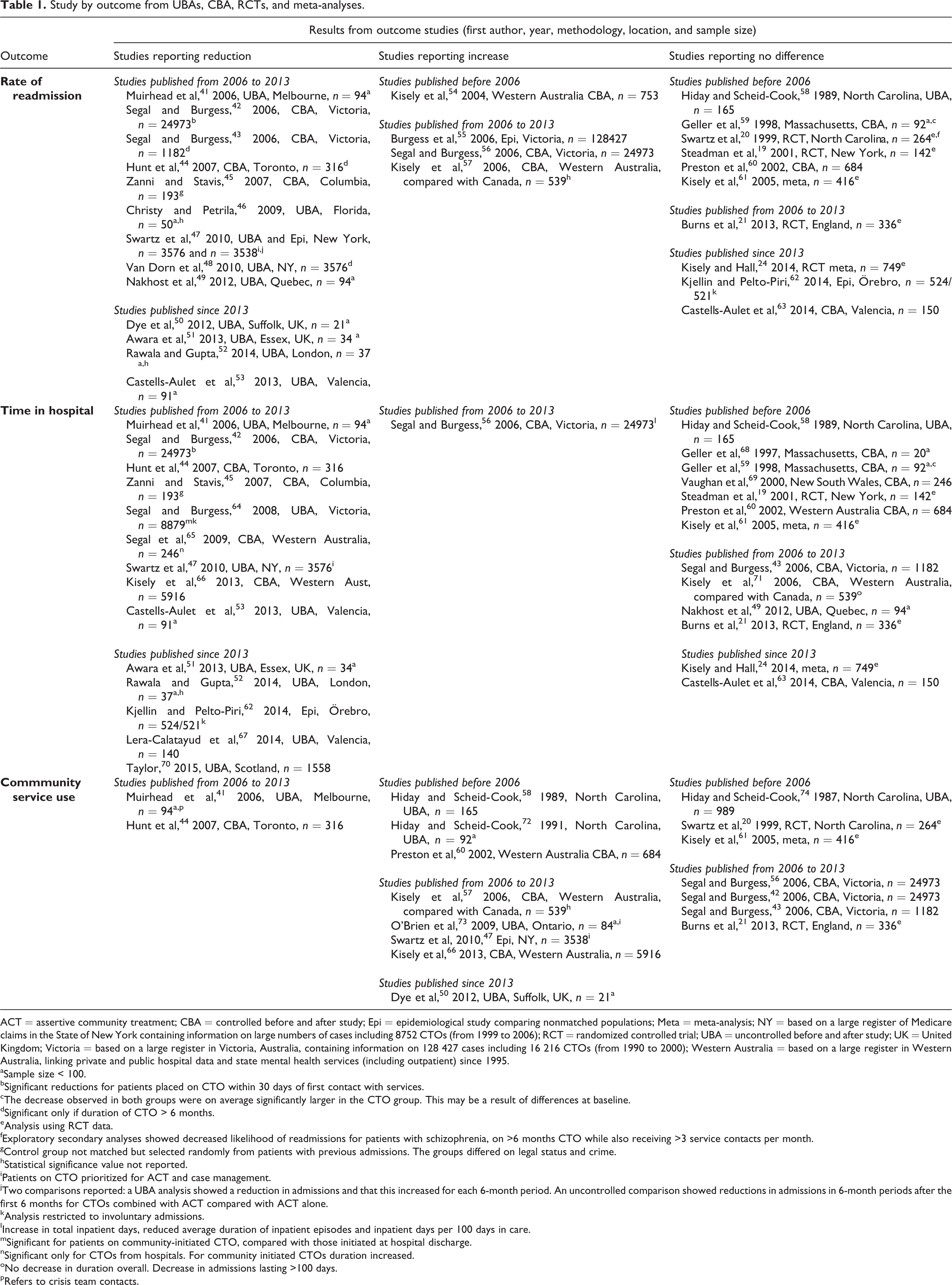
ACT = assertive community treatment; CBA = controlled before and after study; Epi = epidemiological study comparing nonmatched populations; Meta = meta-analysis; NY = based on a large register of Medicare claims in the State of New York containing information on large numbers of cases including 8752 CTOs (from 1999 to 2006); RCT = randomized controlled trial; UBA = uncontrolled before and after study; UK = United Kingdom; Victoria = based on a large register in Victoria, Australia, containing information on 128 427 cases including 16 216 CTOs (from 1990 to 2000); Western Australia = based on a large register in Western Australia, linking private and public hospital data and state mental health services (including outpatient) since 1995.
aSample size < 100.
bSignificant reductions for patients placed on CTO within 30 days of first contact with services.
cThe decrease observed in both groups were on average significantly larger in the CTO group. This may be a result of differences at baseline.
dSignificant only if duration of CTO > 6 months.
eAnalysis using RCT data.
fExploratory secondary analyses showed decreased likelihood of readmissions for patients with schizophrenia, on >6 months CTO while also receiving >3 service contacts per month.
gControl group not matched but selected randomly from patients with previous admissions. The groups differed on legal status and crime.
hStatistical significance value not reported.
iPatients on CTO prioritized for ACT and case management.
jTwo comparisons reported: a UBA analysis showed a reduction in admissions and that this increased for each 6-month period. An uncontrolled comparison showed reductions in admissions in 6-month periods after the first 6 months for CTOs combined with ACT compared with ACT alone.
kAnalysis restricted to involuntary admissions.
lIncrease in total inpatient days, reduced average duration of inpatient episodes and inpatient days per 100 days in care.
mSignificant for patients on community-initiated CTO, compared with those initiated at hospital discharge.
nSignificant only for CTOs from hospitals. For community initiated CTOs duration increased.
oNo decrease in duration overall. Decrease in admissions lasting >100 days.
pRefers to crisis team contacts.
Table 1 displays how the results from the relevant studies indicate either improvement, decline, or no change, for patients on CTOs, measured by the 3 most commonly reported outcomes: readmission rate, time in hospital, and community service use.
As can be seen in Table 1, current studies provide a messy picture, with most relevant articles reporting no difference. Strikingly, all randomized evidence (indicated by table note e) shows no effect of CTOs on these outcomes.
As is apparent from the extensive footnotes in Table 1, comparisons across studies are less than straightforward, as a number of the reported outcomes was affected only in subgroups of patients. Numerous analyses included samples of less than 100 patients and should be interpreted cautiously. This applies particularly to UBA studies, most of which are clustered in the improved outcome cells in the table. Their small samples usually reflect that recruitment was limited to one service or area. The lack of matched control patients means these results could be due to regression to the mean. This could explain the opposite results in 2 studies conducted in Valencia, Spain, by the same team of researchers, for instance, both with a 2-year follow-up. While their UBA study showed positive outcomes for patients on CTOs, 53 their CBA study showed no difference between CTO patients and matched control patients. 63
Churchill et al rated the quality of the body of literature they reviewed as poor. Kisely et al 23 also assessed the general quality of studies to be poor. Only 5 nonrandomized studies were of sufficient quality to be pooled with the then 2 available RCTs in a meta-analysis. While not conducting a formal quality assessment, Maughan et al pointed to a lack of conceptual clarity within individual studies and in the field of CTO research as a whole. 6 There is also a lack of clarity concerning how some outcomes should be interpreted, such as length of stay and service contact, because they may reflect matters associated with the service context and not with the patient. In some studies, for example, patients placed on CTOs were prioritized for intensive services, such as assertive community treatment. It would hardly be surprising, therefore, if studies demonstrate a higher level of subsequent contact with those services. Unless it is specified what type of service is being used (which is only done in a minority of studies), it may be impossible to know whether the level of contact reflects a positive or negative outcome: increased contact with a standard community team may show improved engagement (usually interpreted as a positive outcome) but increased contact with a crisis team may indicate relapse (a negative outcome). 6 Moreover, some outcomes may be interpreted by different authors either as a CTO outcome or as part of the CTO process. For example, as just mentioned, level of service contact is used as an outcome in many studies, while others view it as part of the CTO process (that is, greater surveillance of people under CTOs). The same issue may arise in terms of admission. Under the English regime, for instance, short recall admissions for up to 72 hours are permissible, but these admissions should probably not be counted as a CTO outcome but as part of the process. 6
Exploratory Studies
Among the 28 outcome analyses reviewed by Churchill et al, 14 reported subgroup or regression analyses from 1 RCT. 2 These analyses explored moderators or predictors of associations between CTOs and various outcomes, and generally found positive results. Significant reductions in readmissions were reported for the patients who were kept on a CTO for more than 6 months while also receiving frequent service contacts (≥3 per month, median 7.5). Several other outcomes (adherence, violence, arrest, or quality of life) also reached statistical significance when patients were divided up according to the duration of their CTO (and not according to randomization), or when a nonrandomized sample of 67 violent patients was included in the analysis. These exploratory analyses were not considered outcome studies as such in Churchill et al’s review (and are not included in Table 1) due to these methodological issues. The lack of significant differences in the original analysis of this trial also means they do not infer causal associations, even if they are useful for developing new hypotheses. 2 Indeed, these findings have led many subsequent studies to focus on the effects of long-term CTOs. Nonrandomized studies have not established, however, whether such long-term improvements (where observed) accrue because some patients are selectively kept on the CTO when things seem to be going well for them and the CTO is thought to be the reason. 75
Wider Outcomes Tested in Randomized Controlled Trials
Given the univocal results from RCTs, as seen in Table 1, it is worth looking at these 3 studies in more detail, including the wider range of outcomes investigated.
The New York RCT recruited patients among those referred to the outpatient commitment program at an acute hospital in New York City in 1994. 19 Patients (n = 142) were randomized, either to treatment under a court-ordered CTO or to voluntary status, and followed up for 11 months. Patients with a history of violence were excluded. The 2 groups were comparable on all variables except for a higher proportion of substance dependency in the CTO group and in homelessness among the control subjects. Both groups received case management and close follow-up during the trial (this was not standard care).
The North Carolina trial took place between 1993 and 1996, and recruited patients from 1 state hospital and 3 public inpatient services. 20 A total of 264 patients were randomized between a court-ordered CTO and voluntary status and followed up over 12 months. Those with a history of violence were not randomized but were instead enrolled in a companion study (n = 67). The 2 randomized groups were comparable, apart from lower insight and higher adherence in the CTO group. All received case management, which went beyond standard care. Attrition was low (18%) and equally distributed.
The Oxford Community Treatment Order Evaluation Trial (OCTET) took place between 2008 and 2013. Patients (n = 336) who were detained in 32 National Health Service (NHS) hospitals across England were randomized and followed up for 12 months. 21 There were no exclusions for dangerousness. Because it was considered unlawful to randomize patients deemed to need compulsory care directly to voluntary status, the control group was discharged from hospital to voluntary status through a short term (median 8 days) leave of absence from hospital (under what is called section 17 leave). There was no difference between the groups, and attrition was neglible. Both groups received case management within multidisciplinary teams, in line with local standard care for this patient group.
The samples in the 3 RCTs were similar in terms of their sociodemographics and clinical status. 25 They also matched closely that described in the literature on CTO populations internationally. 2 All 3 trials had readmission rate as the primary outcome measure, but also investigated a range of other outcomes, as listed in Table 2.
Outcomes tested in randomized controlled trials and meta-analyses.
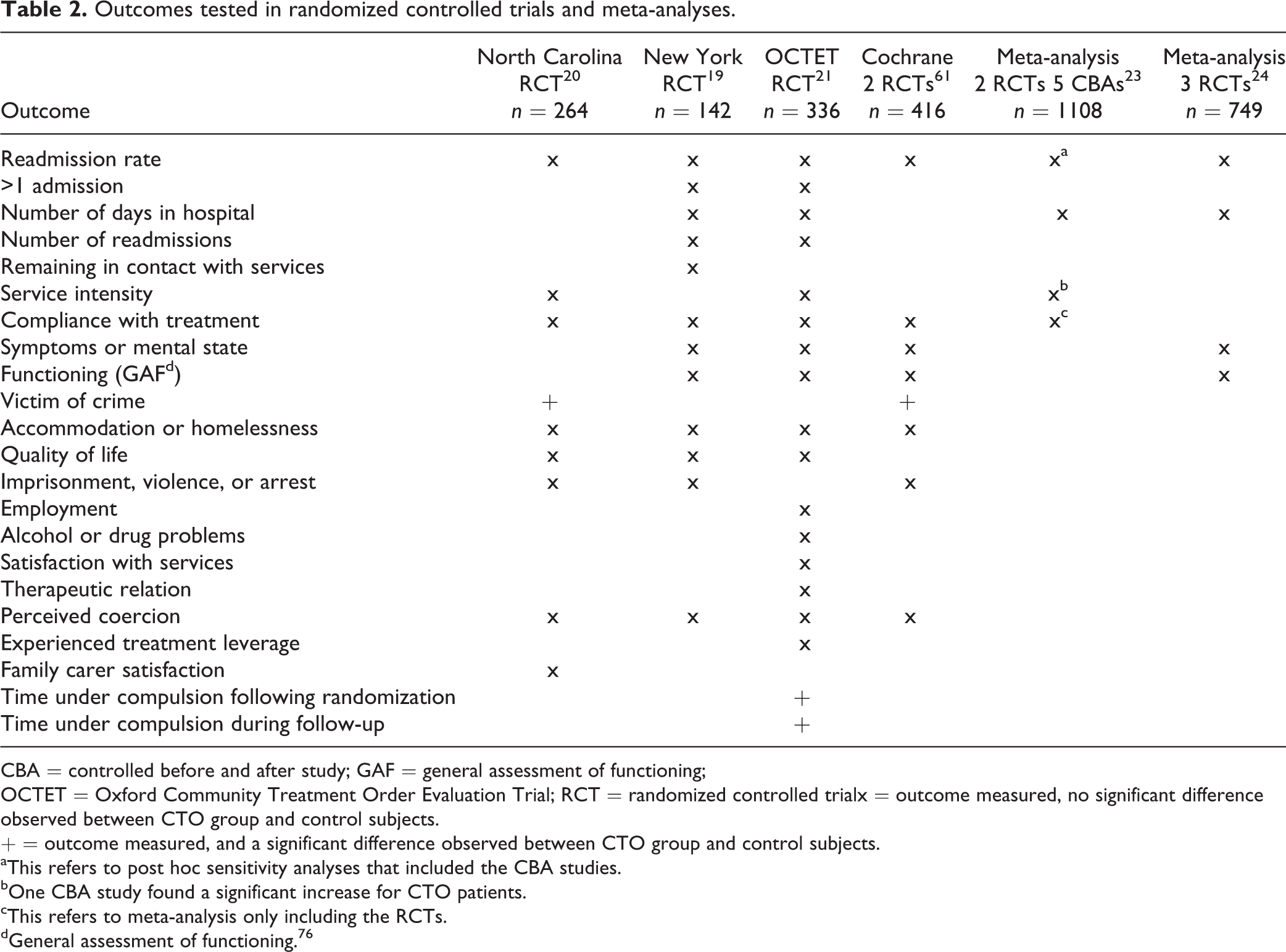
CBA = controlled before and after study; GAF = general assessment of functioning;
OCTET = Oxford Community Treatment Order Evaluation Trial; RCT = randomized controlled trialx = outcome measured, no significant difference
observed between CTO group and control subjects.
+ = outcome measured, and a significant difference observed between CTO group and control subjects.
aThis refers to post hoc sensitivity analyses that included the CBA studies.
bOne CBA study found a significant increase for CTO patients.
cThis refers to meta-analysis only including the RCTs.
dGeneral assessment of functioning. 76
As we can see in Table 2, there was no effect of CTOs on any of the outcomes, except that those in the CTO group were less likely to report being a victim of crime in the North Carolina study (16%, compared with 31%; P = 0.004). The OCTET trial found a significant difference in time under community compulsion immediately following randomization (median 182 days for those on CTO, compared with 8 days for control subjects, P < 0.0001) and in total time under compulsion during follow-up (median 255 days for those on CTO and 102 days for control subjects, P < 0.0001). Those discharged from hospital to a CTO therefore spent far more time under compulsion during the follow-up period than those in the control group. The a priori defined subgroup analysis in the OCTET trial found no difference in readmission rates based on sex, ethnicity, diagnosis, living situation, education, symptoms, or functioning. 31
The randomized evidence also has some limitations. The New York trial had a smaller than expected sample size and high attrition rates (45% at 11 months) which could have affected the statistical power. There were also issues of lack of adherence to the research protocol. 77,78 The exclusion of violent patients in the New York and the North Carolina trial may limit their generalizability. 79 The OCTET trial experienced some protocol violations with treatment of 22.5% patients (35 in the CTO arm, 40 among control subjects) not following randomization. A per-protocol sensitivity analysis removing protocol violations, the standard method for addressing this issue, did not alter the findings, however. 21
Meta-Analyses
Table 2 also shows the results of published meta-analyses. A Cochrane review pooled the 416 patients from the 2 US trials. 22 No difference was found in readmission, service use, social functioning, mental state, homelessness, satisfaction with services, or perceived coercion. There was some evidence that CTOs reduced risk of victimization. The same authors pooled high quality nonrandomized studies with the RCT data, 23 bringing the number of patients to 1108. This included patients with a history of violence and clinician-initiated CTOs. No difference was found in readmission rates, duration of readmissions, total days in hospital, or treatment and contact adherence. Finally, a meta-analysis that included patients from all 3 RCTs (n = 749) found no effect on readmissions, duration of readmission, symptoms, or social functioning. 24 In sum, all the meta-analyses concur with the available RCT evidence and the systematic reviews in their findings: CTOs have not been shown to improve patient outcomes.
Discussion
CTOs are extensively used to prevent relapse and readmission. However, there is no support in the existing evidence for the hypothesis that they have the desired results. The nonrandomized outcome studies show discrepant results. Even if we disregard methodological weaknesses, the differences between their findings are striking, with some reporting benefits and others reporting none, on the most frequently applied outcomes. None of the analyses using randomized data found any benefit to CTOs on a wide set of outcomes, with the exception of a reduced likelihood of falling victim to crime. No other clinical or social benefits have been identified at the top level of evidence, but a significant increase in time spent under coercion by patients on CTOs has been observed. This casts doubt over the use and ethics of CTOs. While several analyses have explored whether CTOs are ethically justifiable, these have been premised on the order leading to clinical or social improvements.
Despite the current evidence, the debate goes on regarding whether some patient groups may benefit from CTOs and whether they could lead to benefits not yet measured.
80
–82
To help settle uncertainty, future research should be designed so that: The findings can be generalized to other settings: Outcomes (and how they are measured) are standardized so as to increase the potential for comparison, to make it possible for a larger number of studies to be included in future reviews, and for more patients to be pooled in meta-analyses: There is clarity about whether reported measures are considered part of the CTO intervention or an outcome of it (for example, increased intensity of services, or brief recall admissions): It is possible to distinguish any effect of the CTO from other interventions that the patient is receiving (such as assertive community treatment): The analyses of outcomes during different time periods (for example, 6-month periods) can determine causal direction so as to identify any long-term effects of CTOs
To address these points, it seems that what is needed are further RCTs to complement those already conducted. Such trials would need to find mechanisms by which all eligible patients are randomized, sample sizes large enough, and protocol violations minimized. Outcome measures should be clearly defined and unambiguous in their interpretation across settings.
Footnotes
Author’s Note
Jorun Rugkåsa is a member of the OCTET group that conducted the RCT of the English CTO regime. She is grateful to Åse Marit Hammersbøen, head librarian at Akershus University Hospital, who performed the literature search in May 2015.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and (or) publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and (or) publication of this article. No sources of funding were provided for this research, except the honorarium provided by the Canadian Journal of Psychiatry for writing this review.