
Abstract
The majority of publications have concentrated on individual psychological interventions with a limited focus on manualized group-based approaches for those presenting with mental health difficulties following a history of trauma. Survive & Thrive (S&T) is a psychoeducational course designed for survivors of interpersonal trauma which utilizes cognitive behavioural skills training while delivering psychoeducation on how a history of victimization can impact on the survivors’ life. This qualitative study was designed to gain an insight into female survivors of interpersonal trauma experience of S&T and the associated group dynamics component to evaluate this psychological intervention. The participants described their experience of S&T as a journey towards recovery. The study highlights the benefits of group-based interventions in regard to learning experience within a social context whilst also identifying areas for further development based on the participants’ feedback.
Introduction
There is an increasing number of individuals being exposed to traumatic life events who are seeking mental health support, which is linked to an increased number of patients being referred to statutory psychological services (e.g. Alistic et al., 2014; Hopper et al., 2018). Gibbons (2016) reviewed referral rates to Tayside Adult Psychological Therapies Services between April and mid-July 2016. Her findings showed that over half of patients assessed during this time period experienced trauma that impacted on their psychological functioning. Sweeney and colleagues (2015) captured similar findings regarding the prevalence of trauma presentations in the UK mental healthcare systems, highlighting the need for trauma-informed systems that are effective and benefit both staff and trauma survivors. To support trauma survivors, we need to understand better the effect of trauma on mental health and the limitations of the current evidence-based approaches. This paper reflects the ethos of the Group Analysis Journal which addresses the group dynamic processes in various groups, including organizations and general society in the wider context.
There is limited research into Phase-1, manualized group interventions to support individuals with history of trauma and its consequent symptomatology. The Matrix (NHS Education in Scotland, 2014) was designed to plan the delivery of evidence-based psychological therapies, including group-based interventions. However, the majority of the available research focused on quantitative data, which omits capturing individuals’ experience of manualized group interventions alongside the challenges and benefits of group dynamics that can form a meaningful part of the treatment. A qualitative approach was adopted, as it considers socially constructed meanings that cannot be assessed by numerical data. It offers an insight into how change can be formed in social settings whilst evaluating its contributing factors.
This paper focuses on understanding patients’ experience of Survive & Thrive (S&T) developed by Sandra Ferguson (2008) in conjunction with NHS Education in Scotland. It is a 10-week psychoeducational group designed for people with a history of interpersonal trauma (IPT). S&T aims to achieve patient safety and stabilization in accordance with the phased-based approach for trauma treatment. It promotes understanding of the normal range of reactions to trauma and cognitive behavioural skills training. Sessions are run weekly by two mental health professionals trained in delivering S&T. Each week covers a different topic related to IPT, such as the nature of abuse/trauma and its effects, keeping safe, depression, anxiety, anger, shame and guilt, flashbacks/nightmares, and effective communication. As this is a manualized psychoeducational approach, sharing of detailed adverse experiences was not encouraged. Thus, providing a safe environment for individuals to learn about the impact of trauma on mental wellbeing. Given the manualized nature of S&T, it is important to understand the group dynamic as an intervention itself for those with IPT history.
IPT and mental health
S&T was specifically designed for IPT, which is defined as having a traumatic experience of emotional and physical abuse/neglect, sexual abuse across the lifespan, domestic abuse, stalking, and/or harassment in adulthood (Ferguson, 2008). Exposure to traumatic events during childhood can substantially influence a child’s development which is strongly associated with experiencing mental health issues throughout their lifespan (Hetzel-Riggin and Roby, 2013). Alistic and colleagues’ (2014) meta-analysis suggest an average prevalence rate for Posttraumatic Stress Disorder (PTSD) of 15.9% across trauma-exposed children and adolescents. Surviving IPT can influence a number of individuals’ functioning abilities, such as their emotional regulation, alterations in attention and consciousness (dissociative symptoms), self-perception (self-blame, guilt), in perception of the perpetrator (acceptance of the perpetrator’s belief system), difficulties with both trust and intimacy, impact on their sense of safety (anxiety), and sense of hopelessness (depression) (Courtois, 2008). Whilst we understand the range of IPT impact on individuals functioning abilities, we are still learning about their experience of the specialist treatment approaches.
Evidence-based treatment for IPT
The majority of the research has concentrated on individual treatment approaches for patients with a history of IPT. Courtois and Ford (2009) argued that at a service level, group therapy is more efficient as it can be offered more broadly. It provides patients with a sense of normalization of their symptoms as a response to trauma with a sense of not being alone; they are not the only one who feels this way (Foy et al., 2001; Lukens and McFarlane, 2004). Additionally, it counteracts isolation, provides peer support and observational learning while ameliorating shame/guilt-based cognitions (Herman, 1992; Lukens and McFarlane, 2004).
The group analysis concept explains that we are born out of our social context which is at the core of how we operate. This places emphasis on understanding our past and present, social and cultural context. The group-based approach encourages not only seeing individuals’ lives in isolation but in a social context (categorization) and connected to others (identification). There is limited research on the effectiveness of manualized approaches for IPT and how having a structured approach can facilitate understanding of one’s experience in social context.
Herman’s (1992) conceptual framework identifies three phases of trauma recovery. Phase-1 emphasizes reestablishment of safety in relationships and stabilization of symptoms from trauma which affect daily functioning. This can be achieved through psychoeducational approaches which emphasize present-focused, coping strategies/skills, elimination of self-harming behaviour, control over acute symptoms, and increased self-care (Lubin et al., 1998; Lukens and McFarlane, 2004). Phase-1 provides a chance to make connections between trauma history and current difficulties while addressing the origins of dysfunctional behaviours as attempts to cope with overwhelming stress (Cloitre, 2016). It prepares patients for Phase-2, which entails remembering, making sense of and mourning past experiences to reintegrate traumatic memories. Phase-3 then focuses on reconnection with others to move past the trauma and enjoy future.
Mahoney and colleagues (2019) meta-analysis supports the importance of both trauma memory processing and group-based psychoeducational-only approaches for adults with PTSD symptoms. They suggest early interventions offered as part of a phased approach consisting of trauma specific symptoms psychoeducation being more effective than usual care in improving PTSD symptoms. This highlights the benefits of Phase-1 psychoeducation group-based interventions for patients to then safely engage with Phase-2 and Phase-3 treatment focused on trauma reprocessing.
Psychoeducational groups for IPT survivors
To date only two studies evaluated S&T which is widely used by NHS Scotland Psychology Services. Ball and colleagues (2013) examined female offenders’ experience of S&T. Their results indicated statistically significant differences between pre- and post-treatment scores across all PCL-C dimensions and CORE measures with the exception of the CORE-risk subscale, supporting the effectiveness of psychoeducational group-based treatment for IPT survivors. However, the purity of evaluating the effectiveness of S&T was impacted by modifying the structure by compressing the course to eight sessions. Additionally, their study cannot be generalised to the wider population given its forensic sample.
Karatzias and colleagues (2014) used a mixed-method study to examine the efficacy of S&T for survivors of childhood sexual abuse. The qualitative component of the study was built on a quantitative study that showed no clinically significant change over time in participants’ presenting problems. While there was no evidence of change over time in measures of psychological wellbeing (general distress levels, traumatic symptomatology, depression, anxiety, self-esteem, and life satisfaction), lifestyle changes were evident with participants less likely to report self-harm and presenting with reduced substance misuse, as well as involvement in illegal/antisocial behaviours at post-treatment and follow-up. Their qualitative data also suggested overall satisfaction with S&T, despite the 43% attrition rate and some apprehension prior to starting it. Increased acceptance of the reality of the abuse was identified as a key achievement and learning experience acquired.
While Karatzias and colleagues’ (2014) study provides good evidence for some change in participants’ attitudes following completion of S&T, their sample was of mixed gender (89.2% female, 10.8% male) and their conclusions do not consider how the experiences of male and female IPT survivors may differ. Women often report more sexual assaults in adulthood associated with elevated baseline guilt conditions and health related complaints, whereas men report more baseline anger directed inward (Miller and Cromer, 2015).
Research aims
This study was designed to address the existing gap in the literature regarding manualized group-based therapy approaches for trauma to facilitate an understanding of female survivors’ experiences of psychoeducational courses, namely S&T. This study’s exploratory structure is inherently phenomenologically oriented. By understanding participants’ experiences, the course could be further tailored to their needs. It can inform clinical decision making in adapting the more challenging parts of the course to ensure that future patients further benefit from S&T, and to prevent early disengagement from the treatment. The local S&T service audit showed attrition rate of 53.1% based on a sample of 243 females.
Method
Participants
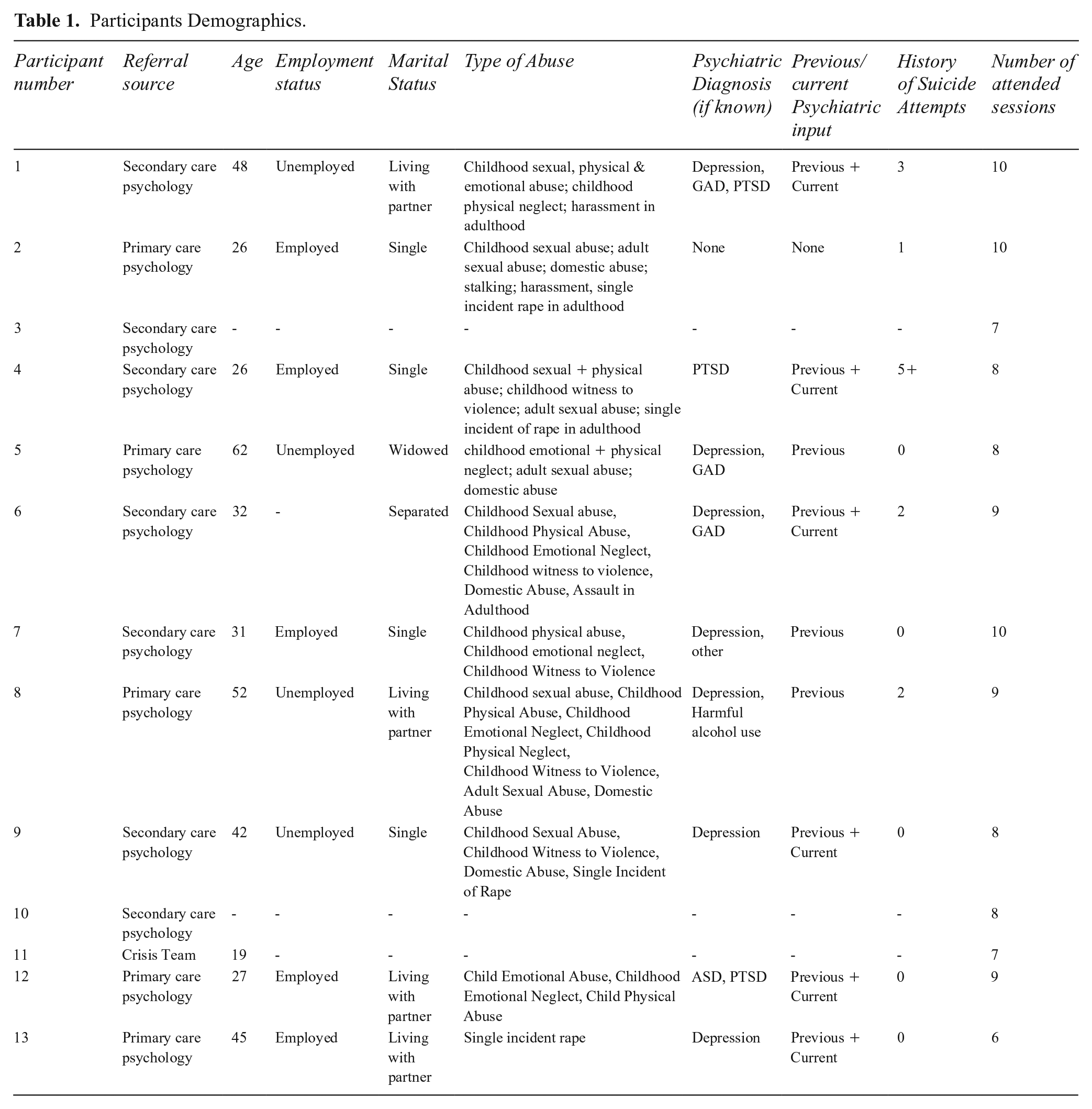
Participants were patients seen within NHS Scotland Adult Psychology Outpatient Service referred to S&T provided across the adult mental health services within that region. Thirteen female patients, who met the inclusion criteria, were interviewed about their experience. Demographics are provided in Table 1.
Participants Demographics.
Inclusion criteria
Women between the ages of 18–65 with a history of IPT who attended at least six of the 10 S&T sessions.
Exclusion criteria
Participants could not be known perpetrators of abuse themselves or have attended a group co-facilitated by the Chief Investigator (CI).
Procedure
NHS ethical approval was granted. The S&T team identified potential participants meeting the inclusion criteria. Thirteen women agreed to participate in the study. Each participant attended a 30-minute semi-structured interview, which explored their experience of S&T. Each interview began with a neutral open-ended question, such as: ‘What has been your experience of attending S&T?’ The conversation developed during the course of the interview into unique interactions typical of the verbatim. The transcript omitted non-verbal signals whilst it incorporated pauses, overlapping speech and interviewee’s change of intonation.
Design and analysis
A qualitative approach was adopted which considers socially constructed meanings. It is more sensitive to multiple interpretations that individuals may make of their experiences in the process of meaning-making (Smith, 1996). The data were explored using Interpretative Phenomenological Analysis (IPA; Smith, 1996). This approach provides participants with space to voice their experience, and the meaning they assign to these. IPA is an established, systemic and phenomenological-focused approach that allows for the interpretation of first-person accounts in a meaning-focused qualitative method (Smith, 1996).
The data analysis involved five separate stages, as per the IPA methodology.
Meaning constructions—transcribed verbatim analysed in accordance with an idiographic and iterative approach;
Identification of key emerging themes and coding of these;
Coded themes comprised of constituent themes were clustered into superordinate themes—relating those to the overarching dimensions of the interview narratives;
Data was interrogated nomothetically; and
The identified themes within each transcript were entered into a table of exemplary quotes, constituent themes, and superordinate themes (Smith, 1996).
Findings
During the interviews many patients indicated to have been struggling with their mental health prior to accessing S&T. Table 1 captures the number of interviewees’ attempts on their life prior to enrolling in S&T, reinforcing the sense of helplessness regarding the future described by the interviewees.
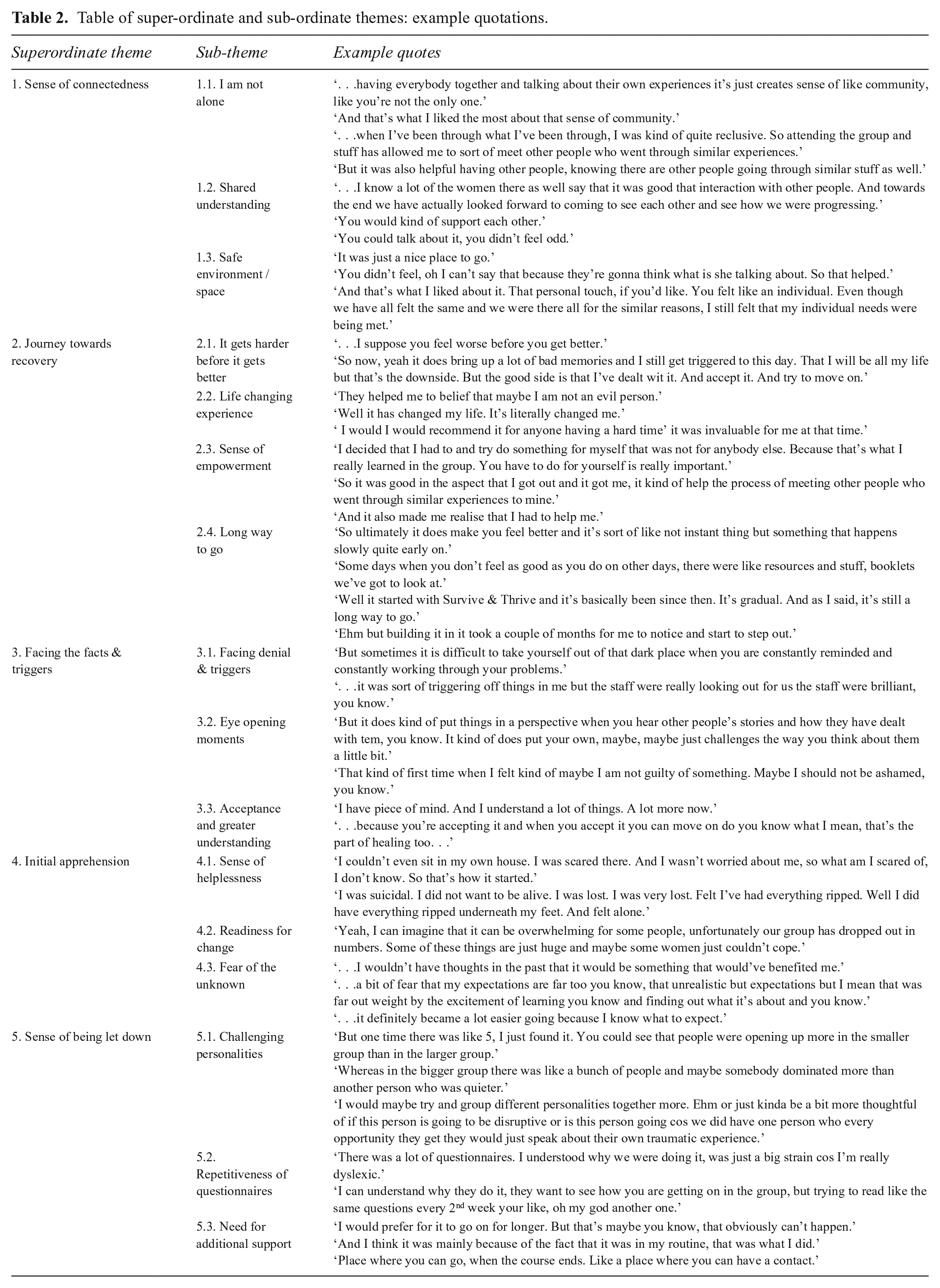
The main theme identified was a belief to be the only one feeling this way. Five superordinate themes emerged through the analytical process. The interviews offered varied individual expressions of these themes, and consistent commonalities allowed some insight into the effectiveness of the manualised group-based psychoeducational intervention. It highlighted the meaning patients have taken from this experience and the process by which this may occur. Table 2 outlines the captured superordinate and subordinate themes with example quotations. Further elaboration of the themes, accompanied by verbatim illustrative data excerpts, is provided below.
Table of super-ordinate and sub-ordinate themes: example quotations.
Theme 1: Sense of connectedness
Figure 1 shows the CI’s interpretation of how the superordinate and respective subordinate themes occurred during the interviews based on the participants’ experience of self while attending S&T. Despite each interview being very individualistic, a pattern was identified in how the participants understood their experience of S&T and the overlap of the stages they went through.
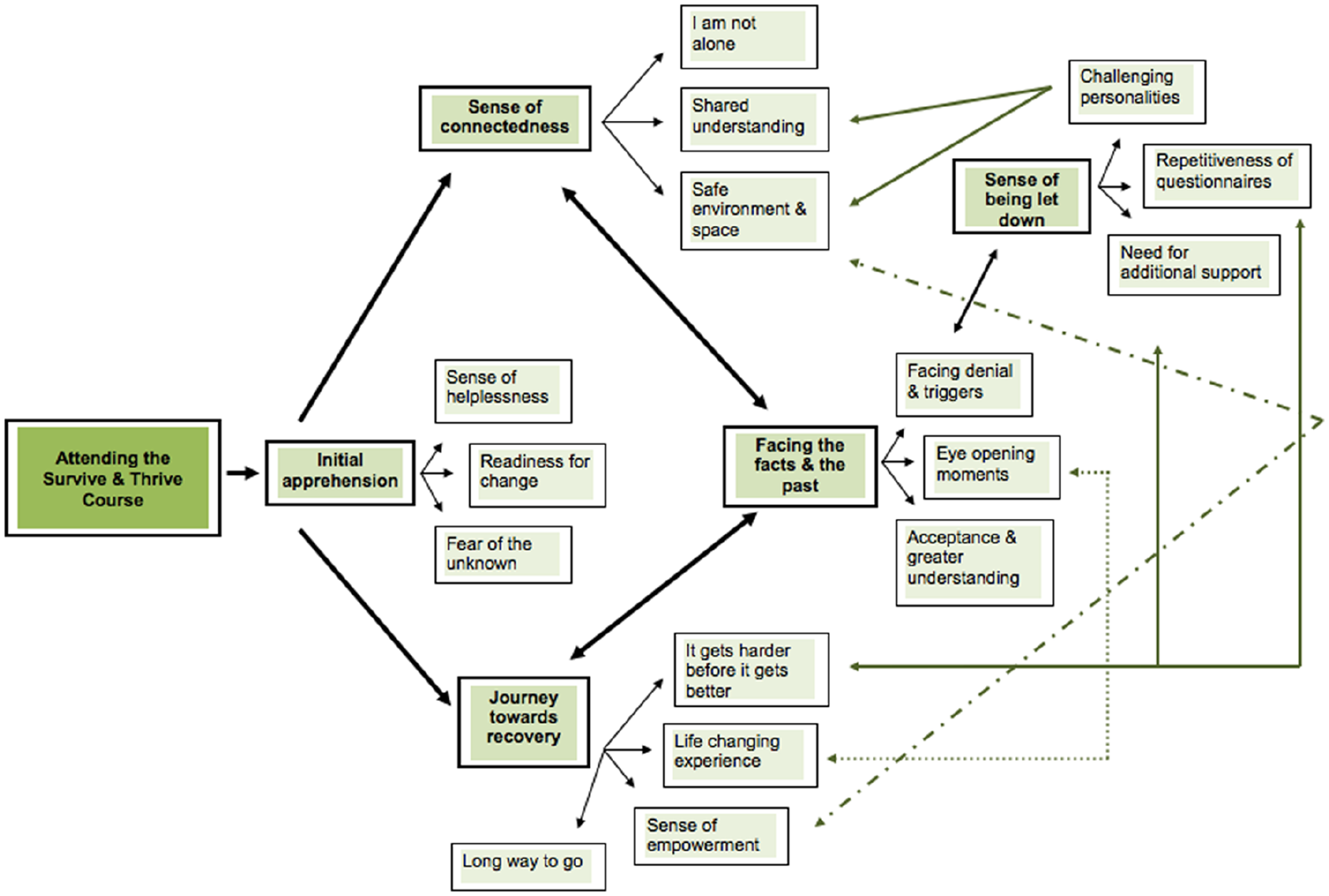
Representation of superordinate and subordinate themes as they occurred during the interviews.
1.1. I am not alone
As a consequence of what victims of IPT experience, they can feel alone. Often, they can internalize what has happened to them as being their fault, engaging in self-blame. As highlighted in a number of quote examples below, the most valuable aspect of S&T was the sense of connectedness and not being alone, as captured in the aforementioned literature (Foy et al., 2001; Lukens and McFarlane, 2004).
. . . you realize that people are in the same boat as you and before that I’ve never thought of that. (Participant5)
And: I’m sitting here crying cos I am really relieved that I got somewhere and someone I fitted in. I actually it was like all my life I felt different . . . (Participant8)
As well as: I found the experience more beneficial being with others and I was quite surprised about that . . . (Participant9)
1.2. Shared understanding
The participants then mainly spoke of benefiting from being understood without needing to go into detail about their experience. It allowed them to place their experience in a social and cultural context without having to disclose any details, as many might not have been ready for Phase-2 approach.
For example: . . . I think just having that connection of you know, not knowing what the specifics were, but having the connection of, you know nobody really deserves to be in an abusive situation and you know sort of you are strong enough to get through it . . . (Participant9)
And: . . . there’s something different about the course to just one-on-one therapy, you do your own therapy and you go and you learn more among other people who have been through similar experiences to you or at least they just understand what it’s like to have had a difficult past. (Participant12)
1.3. Safe environment/space
Going to new places and building trust can be challenging (Foy et al., 2001) therefore, creating a safe environment for individuals to talk amongst themselves is important. Such as: It felt very safe because I knew that the other women that were there, were there for the same reasons as me. And it has given me a bit more confidence to speak up in a group because we were there all for the same reason. (Participant2)
And: Just how it made you feel. It was just really nice and it was a relaxing environment as well. And it was safe. No judgement or you know it wasn’t too personal either because it was a group thing. It was good. Really good. (Participant6)
Theme 2: Journey towards recovery
The participants captured their experience of S&T as a ‘journey towards recovery’ with the subsequent themes.
2.1. It gets harder before it gets better
As expected for any psychological treatment, overcoming mental health difficulties means having to open up about difficult experiences and/or engage in a behavioural change. This often gets more challenging before improvement is noted (Beck, 1997; Tasca et al., 2017). Similar experiences were captured by the participants: . . . it sort of got harder the more in depth it tended to go. And I found it harder the sort of last the last three sessions were really tough. But they were also helpful as well. (Participant4)
Or It’s therapy, isn’t it. So, it brings out the bad. Because you have to bring it all up to understand it now as an adult because everything I have seen as a child made no sense to me. (Participant6)
2.2. Life changing experiences
Once participants progressed through the sessions they found more difficult and started to move towards noticing the change, they described this as ‘life changing’. By gaining a better understanding of the normal range of emotional responses to what they have been through, it allowed them to move away from self-blame and understanding their emotions better. For example: That it made me understand that. That it is not a flaw in me, it is because of the lack of learning and caring as a child . . . But I went through most of my adulthood not understanding that and being very scared of people and not wanting to take part in things. And being very sensitive and being upset very easily. And I did not know all of these things until I have gone along to S&T. (Participant2)
And It just gave me a new perspective. Like another way to think about things rather than the way I was thinking about things. Because I was in like quite a bad way. Yeah but I found it amazing, life changing. (Participant6)
2.3. Sense of empowerment
By understanding what they have been through, learning from each other and not being alone in this process, participants reported a sense of empowerment.
Profoundly it enabled me to help myself that’s what it enabled me to do. To identify and help myself I haven’t come out as Wonder Woman, I’m not saying that cos you know life aint easy, you know. But a greater insight into the way I think . . . (Participant8)
The mode of delivery was also complimented. The role of the facilitator rather than observer was valued which provided a structure to the sessions. This felt less overwhelming and helped with confidence to open up about their experiences.
It’s like the, the group gives you this extra bit of strength and courage just the way it’s set up and the way they teach and the way that they do things . . . (Participant12)
2.4. Long way to go
Most participants reported not noticing the benefit of S&T until a couple of months later. This was highlighted in former literature regarding the need for time to consolidate newly acquired skills, and a chance to put them into practice (Pacual et al., 2015). Some also spoke of the importance of handouts they were given and being able to go back to these.
Probably it wouldn’t be until a couple of months after it. And then I started going back over the sheets and stuff. And because it wasn’t as intense and you weren’t in a room with strangers. I was going through things and understood it sort of better and how to apply it and use it. (Participant4)
Recognizing the newly acquired skills set that not everyone has: . . . it is when you actually reflect back on it when you think, well look these are skills I can take away with me. They are not something everybody know . . . (Participant1)
Acknowledging the course is not a ‘cure’ it is a guide to making improvements in one’s quality of life (Tasca et al., 2017): Now S&T it’s not a curing thing, it’s not a click fingers and done, but it gives you tools, it gives you the tools to kinda face life and to just keep going, which I needed at that time. (Participant7)
Theme 3: Facing the facts and the past
The participants described the hardest part of S&T being facing the facts; having the co-facilitators describe types of abuse with its effects on mental health. Most of the participants also recognized the benefits of having to sit through more challenging discussions, as it allowed them to gain a better understanding of their mental health (e.g. Hundt et al., 2017; Tasca et al., 2017). The themes below captured the process of what the participants experienced.
3.1. Facing denial and triggers
This theme is a common reflection of psychological treatment that was captured by prior publications (e.g. Hundt et al., 2017; Tasca et al., 2017). Patients tend to avoid remembering the past as they are unsure how to process the associated emotions. Thus, many participants described this part of the course as triggering and emotionally challenging.
The issue with it is that it’s so every single time you go it’s that whole session and you are bombarded with all of this. In a positive, not bombarded in a negative way. But you think about it and you think about it some more and you go over, over, and over it again. So that honestly I would seem both as a positive and negative because I take it for me personally if I am thinking about it all the time and working through every little bit it holds you in the past. (Participant1)
3.2. Eye opening moments
A majority of the participants described the ‘wow’ effect, when they came to a self-realization. They realized that topics they did not identify with initially have actually been relevant to them. The main topics that participants described as ‘a big eye opener’ were guilt and anger; whilst not realizing that repressing these can contribute to their maladaptive coping strategies.
Just because I feel guilty about something does not mean that I’ve caused it. And being able to share my guilt and the shame you have about the abuse has been massive. And that itself has helped you so much. It’s like nobody has ever said to me, it is not your guilt. The guilt belongs to the abuser. They were the one who were guilty. But they have left you carrying their guilt. Nobody has ever said that to me and it was like, wow. (Participant2)
3.3. Acceptance and greater understanding
Hogan and colleagues (2006) noted the benefit derived from interpersonal group-therapy based on the different processing types. This was also captured by the interviews in how the written and verbal mode of delivery enabled them to synthesize and consolidate their past experience whilst also learning through observation and from each other.
I started to gain more understanding and awareness into what I feel and why I feel the way I do. Just the way they teach, they just give you an insight . . . (Participant12)
Theme 4: Initial apprehension
Some initial apprehension regarding starting S&T was reported. This was linked to a sense of hopelessness and fear of the unknown.
4.1. Sense of helplessness
Sense of helplessness, fear of not receiving the right help and feeling stuck in life were reported by almost all participants.
My emotional state and my mental state were quite bad at that time. I was working. I was just kind of surviving. (Participant6)
Or Before I took part in the course, I was quite frustrated because I had been working quite hard to make a difference in my life and I needed that extra help. (Participant12)
4.2. Readiness to change
Some of the participants captured the importance of when S&T was offered to them. Given the sense of helplessness, being in the right place in life and readiness to change was important to engage with the treatment (Cook et al., 2017; McMurran, 2012). For example: I was really in the right place at the right time wanting it, you know . . . (Participant8)
Or I mean you have to change, you have to be willing to change I think so. (Participant12)
4.3. Fear of the unknown
Many patients fear attending a group-based treatment because of the ‘unknown’. The participants described this fear being mitigated by meeting the S&T co-facilitator(s) and seeing the room beforehand.
. . . not knowing what to expect. I did meet clinician once before so I knew I would know one person I would recognize her face. Because the thought of a group of people that I do not know, group of strangers, very scary. (Participant2)
Theme 5: Sense of being let down
Despite the above captured positives, some challenges were also noted. Most of these are external factors. The feedback provided insightful points to take forward in terms of the S&T delivery.
5.1. Challenging personalities
One of the main challenges in a group-based treatment is the mixture of personalities. As captured by the participants despite the co-facilitators’ best efforts, there were some individuals who did not respect some of the S&T boundaries. Despite the benefits of having a group of individuals with shared experience supporting sense of connectedness, some patients would overshare personal experience which others found triggering. For example: It was actually the individuals. It was just that some of the trauma that they have experienced had triggered some of the stuff in me. And that was quite hard to deal with. (Participant3)
5.2. Repetitiveness of questionnaires
The participants struggled with the number of questionnaires they had to complete each week as part of the service evaluation. Not only did they find the process of this ‘repetitive’ and ‘boring’, but for some it was highlighting the lack of progress made on a weekly basis whilst triggering low self-worth.
One thing that I found a bit boring but I know that they had to do it was the questionnaires. Sometimes because I felt, I felt for a long time the same. (Participant5)
Or . . . it tends to be just adminy stuff to start with I kinda found that quite boring and quite annoying . . . (Participant7)
5.3. Need for additional support
The general feedback was that participants enjoyed S&T so much that they did not want it to end. Given it allowed them to increase their social levels and sense of connectedness, this was the most difficult part for them. Some spoke of the loss of contact, as they would not get to see each other again: I think when we were kind of put in the group for the 10 sessions and then we were kind of given coping skill and stuff and then we have opened up about stuff that has happened to us and then all of the sudden it just ended. And we have nowhere to turn to and. A lot of the, the couple of the women were like this is it then, we are not going to see each other again. (Participant3)
Some participants stated despite having the co-facilitators available during the break, they would have liked to receive additional support between the sessions. This might be linked to the range of individuals attending the course with different needs and from different services (e.g. Primary Care Psychology versus Community Mental Health Team settings), where different levels of support are provided. For example: . . . if I found the session quite hard. I’d like to speak to someone in a like an appointment just to talk about it one on one, something like that . . . (Participant11)
One of the disadvantages of a psychoeducational course is the lack of opportunity to go over sessions patients did not attend (e.g. due to illness). There are two follow-up sessions that allow for some summary, but this would not cover in full the session someone has missed.
. . . since people are also missing some it would be good to have a kind of revision also in the middle maybe or towards you know the end . . . (Participant13)
Discussion
These findings demonstrate that S&T is not a ‘cure’ for patients with a history of IPT; however, it provides them with new strategies and skills to move forward in their life. It highlights the importance of a phased approach to trauma and benefit of group-based psychoeducational courses focused on Phase-1 safety and stabilization work. One of the key themes identified by the participants was ‘sense of connectedness’. The sense of belonging and not being alone was described by the participants as the main learning from completing S&T. Given the tendency for isolation, vulnerability and difficulties around trust that IPT survivors experience, being in an environment where their social connectedness levels were addressed has helped to improve their overall well-being (Foy et al., 2001; Lukens and McFarlane, 2004). Additionally, having one’s feelings validated by others is important to all individuals, this is particularly vital for IPT survivors, who’s emotions have often been invalidated and neglected contributing to their fear of expressing their feelings (Courtois and Ford, 2009).
S&T facilitated the participants’ ability to create connections with other group members, thereby helping them to combat isolation and alienation. Participants described how sharing their experiences helped to normalize their reactions, which also contributed to shame reduction. It allowed them to understand their experience in a social context whilst learning from each other, removing stigma and developing their interpersonal skills by helping each other (Aviram and Rosenfeld, 2002; Hopper et al., 2018). They also described having a ‘sense of empowerment’ as a result of S&T, which helped with their confidence and increase in social interactions by starting to establish healthy boundaries in their relationships.
The additional superordinate and subordinate themes captured by the interviews regarding vulnerability, ambivalence, and trauma-based treatment approach, are characteristic of the initial phases of any group-based treatment (Yalom and Leszcz, 2005). Although boundaries were set to avoid sharing specific trauma experiences to mitigate these, some participants would over-share personal details. Despite the S&T facilitator training and regular generic monthly supervision, co-facilitators at times struggled to deal with challenging group members. Modality specific supervision for S&T co-facilitators focused on skills development to acknowledge challenging group members’ contributions whilst offering other members an opportunity to speak should be considered. It highlights the importance for skills-specific training on clear boundary setting that is flexible; tight enough to ensure the integrity of the group whilst loose enough to allow the emergence of natural discussion. If individuals experienced any deterioration in their mental health wellbeing during the course of S&T, opportunity was available for an onward referral to other specialist and relevant mental health facilities.
Additionally, S&T facilitators need to focus on patients’ readiness to engage with more triggering aspects of the course while providing additional support to those who might also present with co-morbid presentation, e.g. social phobia. As highlighted by the quotes, this can be mitigated by showing the clinical room and meeting the co-facilitator(s) prior to commencing S&T. Those who find the material triggering could be offered individual review appointments at set stages of the course which could also provide help with management of the more challenging group members.
Furthermore, the study highlighted the importance of time to understand the traumatic experience as well as to practise the newly acquired skills throughout the course. This was captured by the participants as a ‘journey towards recovery’ with the subordinate theme of ‘long way to go’. Despite its inherent stressors, as would be expected of any trauma-based psychological treatment, all the participants spent most of the interviews drawing on the positive aspects of attending S&T. It facilitated a sense of acceptance whilst uplifting stigma and understanding the distressing emotions while acknowledging that these will pass by having a shared experience in the group, which some expressed to have lacked during individual sessions (Aviram and Rosenfeld, 2002; Hopper et al., 2018).
S&T is not a cure, but it helps individuals develop skills to cope better with the past and associated emotions. For some it enabled them to move onto Phase-2 treatment safely. Time to practise and consolidate learning after S&T was crucial for improvement (Pascual et al., 2015). Those interviewed one to two years after completing S&T reported more changes in comparison to those who completed it two to four months ago. A longitudinal study would be required to capture the exact timeline of patients’ progress throughout and after completion of psychoeducational courses.
Overall, this study offers a valuable insight into the female survivors’ experience, adding to the previous studies that focused namely on the effectiveness of S&T. Increasing the insight of the participants’ experience of S&T might assist clinicians and mental health services in adapting this course to their patient population needs and encourage wider use of this manualized psychoeducational course. Findings from this qualitative study should be encouraging for services, recognizing the identified benefits participants experienced as a result of completing S&T.
Clinical implications
Given the above captured benefits a group-based manualized psychoeducational course for female survivors of IPT, some of the barriers to engagement with it should be further explored. This study did not focus on the reasons for disengagement from S&T, as only completers were interviewed. Despite that, it facilitated some insight to the potential contributing factors to disengagement which provide a basis for further research. These findings suggest that receiving additional support both before and throughout the course has been vital. Thus, viewing the clinic room or meeting the co-facilitator(s) in advance made a difference for some. Reduction in the measures required to complete each week should also be considered, given the feedback of this highlighting some of the lack of progress during the initial weeks.
Additionally, some of the feedback was around readiness and willingness to change. Cook and colleagues (2017) identified patient’s readiness as consisting of three components: psychological and psychiatric stability, general readiness to change, and specific skills to manage trauma-focused evidence-based treatments (e.g. distress tolerance, affect regulation skills). Their study highlighted some of the current limitations of the S&T screening process regarding readiness to engage. Existing literature outlines no specific scale that allows mental health services to define ‘readiness’ and this mainly depends on clinicians’ individual judgement (e.g. Couineau and Forbes, 2011; Zubkoff et al., 2015). This highlights the need to identify a uniform measure that can be adopted by clinicians across different services.
Strengths, limitations and future directions
Given the number of patients with a history of IPT being seen within psychology services (e.g. Gibbons, 2016) with new initiatives promoting mental health well-being, there has been an increased focus on the evaluation of different types of trauma-based interventions. This study offers a further insight into female survivors’ experience of S&T, and the factors moderating such.
The primary limitation of this study is its restricted access to the population of a single locality. Thus, to assess effectiveness of this course more broadly and to generalize the findings, this study needs to be replicated throughout Scotland to assess for other factors, such as deprivation index and/or access to other means of support. Additionally, the participants interviewed for this research ranged in terms of time since completion of the course from only a few weeks up to two years whilst importance of time to consolidate was captured during the interviews. To allow for a greater insight into the changes captured over time, future studies could schedule interviews at certain points post-completion to map these changes.
Furthermore, CI conducted this study and carried out the data analysis, meaning that potential limitations arise in using IPA. This approach draws on the researcher interpreting their understanding of the interviews with prior knowledge of the researched topic (Smith, 1996). Moustakas (1994) suggested a technique called ‘bracketing’ allowing the researcher to set aside their experiences and take a fresh perspective. It should however be noted that it is impossible to bracket one’s biases completely (Allen-Collinson, 2009).
Conclusion
Participant feedback gathered within this study suggests the benefit of a manualized group-based intervention is considerable and could provide an important means of supporting an increasing number of individuals presenting with symptoms associated with IPT. The study demonstrated that IPT survivors benefited from being able to identify that they are not the only ones struggling with their past by understanding it in the social context of those with a similar history whilst having the opportunity to learn from each other, which would not be facilitated through individual treatment. This further strengthens the importance of ‘sense of connectedness’ as a contributing factor to greater outcome from psychological interventions (Aviram and Rosenfeld, 2002; Hopper et al., 2018). This research invites mental health professionals and services to evaluate the prevalence of individual psychological treatment that is being offered to patients with IPT history over group-based psychoeducational treatment, namely S&T, and to consider the benefits of increasing access to effective treatment such can provide.