
Abstract
The spectrum of pathological conditions affecting the nasopharynx includes infections, congenital anomalies, and tumoral lesions, particularly angiofibroma, nasopharyngeal carcinoma, and lymphoma. Hypertrophy of adenoid tissue is a frequent phenomenon in children, but it is less common in the adult population. With this case report, we wanted to point out the importance of rhinological and otological manifestations of adenoid hypertrophy in adult patients. A 48-year-old man presented with impaired hearing in both ears, difficulty breathing through the nose, impaired sense of smell, hyponasal speech, and occasional scanty bleeding from the right side of the nose. After taking detailed data, the diagnostics included a classic ENT examination, endoscopy of the nasal cavity and nasopharynx, audiological diagnostics, allergy tests, computerized tomography of the paranasal sinuses and the skull base, and serological analysis for viruses and protozoa. A soft tissue lesion that filled the entire nasopharynx was surgically removed, and the pathohistological analysis indicated B-cell small lymphocytic lymphoma (SLL) with polyclonal plasma cell differentiation. Serological analyses showed that it was a human immunodeficiency virus (HIV)-positive patient, who also had a high blood titer of IgG to the Epstein-Barr virus. The patient was admitted to another institution for oncology treatment under the supervision of an infectious disease specialist. Although rare, malignant transformation of nasopharyngeal lymphoid tissue is possible. B-cell SLL with polyclonal plasma cell differentiation represents a minority of malignancies originating from the nasopharynx, and there are limited data regarding epidemiologic and treatment outcomes. Early recognition and thorough evaluation are essential to distinguish benign enlargement from more serious conditions.
Introduction
Once primarily associated with children, enlargement of adenoidal tissue is increasingly being diagnosed in the adult population presenting with upper airway obstruction. Adults affected may report ongoing nasal stuffiness, excessive nasal secretions, snoring, and frequent postnasal drip. Analysis of cases suggests that persistent infections and allergic responses are the primary causes of lymphoid tissue growth in the adult nasopharynx. Furthermore, exposure to environmental pollutants and smoking are also implicated as notable risk factors for the development of this condition.1,2
Occupational and environmental exposures—particularly to pesticides, organic solvents, hydrocarbons, and agricultural agents—are associated with an increased risk of small lymphocytic lymphoma/chronic lymphocytic leukemia (SLL/CLL). 3 Farming-related pesticide exposure (including herbicides such as 2,4-D and atrazine, insecticides like chlorpyrifos and pyrethrins, and fungicides such as captan) increases SLL/CLL risk by approximately 26%–110% in a dose-dependent manner, likely mediated through oxidative stress and epigenetic dysregulation. 4 Long-term exposure to hydrocarbon solvents (e.g. benzene, toluene), common in manufacturing and painting occupations, roughly doubles the risk of B-cell lymphomas, 5 while prolonged occupational sunlight exposure (>10 years) has been associated with a 2.5-fold increase in risk. 6 These environmental factors may act synergistically with HIV-related immunosuppression through impaired immune surveillance and reduced detoxification capacity, although direct data linking such exposures to nasopharyngeal involvement in HIV-positive patients remain limited.
It is essential to acknowledge that in adults, adenoidal hypertrophy can mimic the clinical presentation of significant nasopharyngeal diseases, including malignant tumors, lymphoproliferative disorders such as non-Hodgkin lymphoma, and infections caused by Epstein-Barr virus (EBV), cytomegalovirus (CMV), and human immunodeficiency virus (HIV).1,2 Because these conditions may overlap clinically, current recommendations emphasize the need for a comprehensive diagnostic evaluation whenever a new nasopharyngeal mass is identified in adults. This assessment should include endoscopic inspection and, following removal, histological examination to determine the underlying cause and definitively exclude malignant disease.
We present a rare case with B-cell small lymphocytic lymphoma (SLL) in which HIV infection primarily manifested with symptoms of an enlarged adenoid in an adult patient.
Case presentation
A 48-year-old male was admitted to our Department of Otorhinolaryngology for diagnosis and treatment. Ten months before admission, the patient had had nasal breathing difficulties, a reduced sense of smell, increased nasal secretion, and secretion dripping down the posterior pharyngeal wall. There was a history of frequent inflammations of both middle ears and hearing impairment, more pronounced in the left ear, as well as occasional, scant nasal bleeding. At another healthcare institution, a myringotomy was performed on the right ear several months before admission to our department, after which hearing in the right ear improved. Objective findings upon admission showed that the right tympanic membrane had a dry perforation in the anterior quadrants toward the annulus. The left tympanic membrane was retracted, yellowish, with prominent vascular markings. Rhinoscopy revealed left-sided deviation of the nasal septum. The inferior nasal turbinates were bilaterally hypertrophic. On the posterior rhinoscopy, a soft tissue lesion was visible in the nasopharynx, partially obstructing the choanae, predominantly on the right. Pure-tone audiometry showed a mild bilateral conductive hearing loss with scotomas at high frequencies, more pronounced on the left. Tympanometry revealed a flat (type B) tympanogram on the left side; measurements on the right could not be obtained. CT scan of the paranasal sinuses and skull base showed retention cysts in the maxillary sinuses and mild chronic inflammatory mucosal thickening of the anterior ethmoid sinuses. The dominant finding was a soft tissue mass filling the nasopharynx (Figure 1). Rigid and flexible endoscopy of the nose and nasopharynx revealed the presence of a soft tissue mass, macroscopically resembling a large adenoid, partially covered in blood and bleeding on contact (Figure 2). The lesion completely obstructed the right and partially obstructed the left choana. The patient underwent surgery under general anesthesia, and the excision of the nasopharyngeal mass (Figure 3), septoplasty, and left-sided myringotomy were done. During surgery, the mass was removed using a transoral approach with a Beckmann adenotome from the roof of the epipharynx and the openings of the Eustachian tubes, and sent for histopathological analysis.
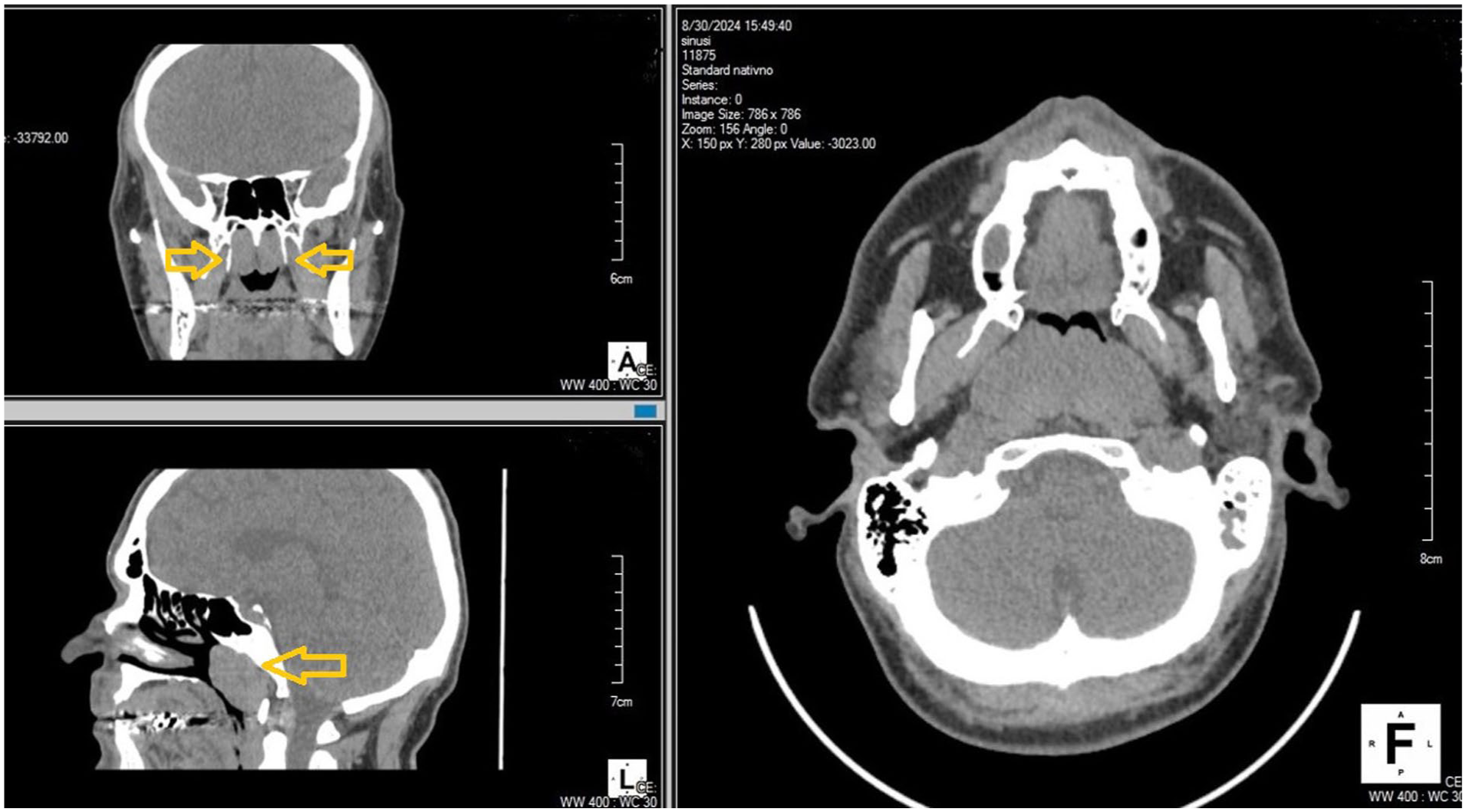
CT scan of the paranasal sinuses and skull base showed retention cysts in the maxillary sinuses and mild chronic inflammatory mucosal thickening of the anterior ethmoid sinuses. The dominant finding was a soft tissue mass filling the nasopharynx (arrowheads).

Flexible endoscopy of the nose and nasopharynx revealed the presence of a soft tissue mass in the nasopharynx, macroscopically resembling a large adenoid, partially covered in blood and bleeding on contact.

Macroscopic appearance of the excised mass from the nasopharynx.
Histopathological analysis after the hematoxylin-eosin staining described fragments of respiratory mucosa diffusely infiltrated with tumorous lymphoid tissue composed of small cells with oval nuclei, loose chromatin, inconspicuous nucleoli, and scant to moderately abundant cytoplasm (Figure 4(a) and (b)). The pathologist could not explicitly determine whether this represented a neoplastic or infiltrative lesion. However, after the immunohistochemical analysis (staining positive for CD20, CD43, and CD138), the final report revealed that the morphological and immunohistochemical findings correspond to B-cell SLL with polyclonal plasma cell differentiation (Figure 5(a)–(c)). DNA analysis of B-lymphocyte clonality confirmed that no monoclonal immunoglobulin heavy chain (IGh) rearrangement was detected in the examined sample.

(a) Histopathological analysis showing the surface of the removed nasopharyngeal mass with transition epithelium and fibrous stroma strongly infiltrated by lymphocytes (Hematoxylin and eosin stain, magnification ×200) and (b) Hematoxylin and eosin stain showing lymphoid architecture by small mature lymphocytes (Magnification ×200).

(a) Immunohistochemical analysis showing diffuse CD20 positivity, (b) CD43 positivity, and (c) CD138 positivity (magnification ×200).
During hospitalization, serological tests were performed for hepatitis B antigen (HBsAg) (negative), hepatitis C virus (negative), HIV, CMV, EBV, varicella zoster virus (VZV), herpes simplex virus (HSV), and immunoglobulins against Toxoplasma gondii (IgG and IgM—both negative). The presence of IgG antibodies to CMV, EBV, VZV, HSV-1, and HSV-2 was confirmed. Serological testing (Roche Cobas analyzer, Basel, Switzerland) indicated HIV, and reverse transcription polymerase chain reaction (RT-PCR) testing of the patient’s plasma confirmed HIV infection. Therefore, the patient was EBER-positive, meaning EBV RNA was detected in tumor tissue by in situ hybridization.
Blood sampling and lymphocyte typing were performed—the lymphocyte population was analyzed on an FS/SS plot. Absolute values of T lymphocytes (CD3+) were elevated, while relative values remained within physiological limits. Absolute and relative values of the CD4+ T-lymphocyte subpopulation were decreased. Absolute values of CD8+ T-lymphocytes were increased, while relative values remained within physiological limits. The CD4/CD8 ratio was below physiological limits (0.5).
The patient was admitted to another institution for oncology treatment under the supervision of an infectious disease specialist. The therapeutic protocol R-CHOP (rituximab + cyclophosphamide + doxorubicin + vincristine + prednisone) with rituximab was implemented. Prophylaxis of opportunistic infections was also carried out, with monitoring of liver function, kidney function, and hematologic parameters due to additional toxicities that may be more pronounced in HIV-positive patients. The treatment of HIV infection was combined therapy with tenofovir, lamivudine, and dolutegravir. One year after being admitted to our clinic, he is successfully carrying out oncology therapy. The quality of breathing through the nose, hearing, and sense of smell was good. The local findings in the nose, ears, and nasopharynx were good at the follow-up examination.
Discussion
When adults experience nasal blockage on both sides, enlarged adenoids should be included in the list of possible diagnoses. While this study did not find a significant link between adenoid hypertrophy and chronic nasal or middle-ear conditions, the authors stress the importance of thoroughly assessing the nasopharynx in adults with upper airway complaints, since adenoid hypertrophy continues to be an important diagnostic consideration.2,7 Histopathological findings suggest that adult adenoid tissue differs morphologically from pediatric adenoids. While childhood adenoids typically show hyperplastic lymphoid follicles with active germinal centers, adult specimens demonstrate features of chronic inflammation, including lymphocytic infiltration, fibrosis, and squamous metaplasia of the respiratory epithelium. These changes support the hypothesis that adult adenoid hypertrophy is most often a consequence of long-standing inflammatory processes, such as chronic upper airway infections or persistent allergic stimulation, rather than a newly developed lymphoid proliferation. 8 Of course, this refers to situations when adenoid enlargement in adults is not a consequence of the tumor process.
Nasopharyngeal masses are a known, though less common, initial sign of HIV infection. In HIV-positive patients, these masses are most often caused by benign lymphoid hyperplasia rather than cancer.8,9 For patients with HIV, nasopharyngeal masses are primarily benign and usually result from lymphoid hyperplasia.8,9 Conversely, malignancies are more frequently observed in HIV-negative individuals. 9 According to the study by Erasmus et al., 9 only 7.7% of nasopharyngeal masses in the HIV-positive group were malignant, compared to 25% in the HIV-negative group. These findings are similar to those of Desai. 10 In this study, the pathohistological analysis of all evaluated cases showed only nonspecific reactive lymphoid hyperplasia, with no signs of malignancy. A strong association with HIV seropositivity was found—14 out of 14 adult patients were HIV-positive, either previously known or diagnosed during the study. 10
The other authors in some earlier studies emphasize that although not all lymphoid hypertrophy in HIV disease represents malignancy, the increased lifespan of HIV-positive patients may lead to a higher incidence of neoplastic degeneration in the nasopharynx. 11 Among individuals living with HIV, the appearance of lymphoid tissue proliferation within the nasopharynx carries the potential for progression to malignancy, including lymphoma or other neoplastic conditions. Given that nasopharyngeal lymphoid proliferation in adults can closely resemble neoplastic processes, it is critical to perform tissue sampling to definitively exclude malignancy and ensure accurate diagnosis. 10 In our patient, a mass was initially identified in the nasopharynx and subsequently confirmed as lymphoma by histopathological examination.
Nasopharyngeal lymphoma, as a primary malignancy of the head and neck, accounts for only a small proportion of tumors that originate in the nasopharynx worldwide. 12 In Asia, NK/T-cell lymphomas account for 47.5% and B-cell lymphomas for 52.5% of NPL cases, while in the West, B-cell lymphomas are more common (77.5%–87.6%) and NK/T-cell lymphomas are rare (6%). For nasopharyngeal non-Hodgkin lymphoma, B-cell types represent over 90% of cases in the West and 64.3% in Asia, indicating significant regional variation in lymphoma subtype prevalence. 12
It appears in several subtypes, most commonly diffuse large B-cell lymphoma (DLBCL) and extranodal natural killer/T-cell (NK/T) lymphoma. This diversity suggests that multiple biological mechanisms contribute to how these lymphomas form. 12 Epstein-Barr Virus (EBV) is playing an important, but not exclusive, role in its development. EBV assists cancer cells by promoting growth, helping them evade the immune system, and causing genetic changes. 12 Our study documented one rare case of nasopharyngeal small B-cell lymphoma with polyclonal plasma cell differentiation. This patient was EBER-positive, meaning EBV RNA was detected in tumor tissue by in situ hybridization. Hsueh et al. 12 reported only 2 cases of SLL in a series of 35 patients with primary nasopharyngeal lymphoma. The authors briefly mention it as an unusual histopathologic subtype, likely due to its singular occurrence and borderline reactive features within their cohort. 12 Nasopharyngeal involvement of SLL is considered exceptionally rare.12,13 Aldawas et al. 13 present a rare case of association of SLL and chronic lymphocytic leukemia (CLL) manifesting as a mass in the nasopharynx with bilateral middle ear effusion. This presentation is highly unusual, as SLL/CLL typically involves the lymph nodes, bone marrow, and blood, and rarely originates in the nasopharynx. 13
Serological testing performed afterwards revealed HIV positivity in our patient. Knowing the recommendations of the World Health Organization (WHO), we concluded that HIV was detected in the advanced stage of the disease. Current research underscores the value of monitoring CD4+ and CD8+ T cell populations to track HIV progression, with a focus on CD4+ decline, CD4/CD8 ratio, and additional cell markers. 14 Our patient’s immune status was assessed using lymphocyte subset analysis. Results demonstrated a reduced CD4+ T-cell count and a low CD4/CD8 ratio, both characteristic of immunosuppression in HIV infection. These findings indicate advanced immune compromise. The presence of elevated CD8+ T cells further reflects persistent immune activation typical of chronic HIV infection. Overall, this immunologic profile is consistent with chronic HIV and significant suppression of cellular immunity. If the CD4+ count were confirmed below 200/μL or if opportunistic infections developed, the criteria for AIDS would be met. 14
Serological analyses also revealed multiple viral co-infections, prompting us to investigate their impact on lymphoma genesis. HIV and EBV are key factors in the development of B-cell lymphomas, especially in immunocompromised individuals. According to Lurain et al., 15 HIV infection raises lymphoma risk by weakening the immune system rather than directly causing cancer. HIV triggers chronic immune activation, overstimulates B-cells, and reduces CD4+ T-cells, which impairs immune surveillance and allows abnormal B-cell clones to expand. In this compromised state, viruses such as EBV further promote lymphoma. 15 EBV persists in B cells in a latent state and expresses viral proteins (such as LMP1 and EBNA2) that promote B-cell activation, proliferation, and resistance to apoptosis. In HIV-associated immune suppression, the reduced cytotoxic T-cell surveillance allows EBV-infected B cells to expand uncontrollably. This combination of viral oncogenic signaling and impaired immune control supports clonal outgrowth and accumulation of genetic abnormalities. As a result, EBV contributes to the development of EBV-positive lymphoma in immunocompromised individuals.15–17
Normally, cytotoxic T cells control these infected cells, but weakened immune surveillance allows EBV-infected B cells to proliferate without restraint. Subsequent genetic and epigenetic changes, influenced by environmental and cytokine cues, drive the eventual transformation into malignant lymphomas. The specific pattern of viral gene expression (latency I–III) influences the lymphoma subtype. EBV acts as a cofactor—promoting B-cell activation, immune evasion, and cooperating with genetic instability rather than functioning as a direct oncogene.15–18
The literature indicates that while monoclonal, EBV-driven B-cell lymphomas with plasma cell differentiation are common in HIV-positive patients, polyclonal variants are rare, particularly in the context of profound immunosuppression and multiple herpesvirus co-infections.19,20
Current research does not support a direct role for CMV, VZV, or HSV in causing lymphoma. Their main impact on lymphoma patients is through immune modulation and increased infection risk, not direct lymphomagenesis.
While the gut microbiome’s role in lymphoma and the stability of the nasopharyngeal microbiome in HIV are well documented, 21 the nasopharyngeal microbiome in HIV-positive patients with B-cell lymphoma remains unexplored. This represents a significant opportunity for future research.
Comprehensive epidemiological analyses and large-scale datasets concerning HIV-associated lymphomas and nasopharyngeal masses consistently demonstrate that indolent B-cell lymphomas, particularly small lymphocytic lymphoma (SLL/CLL) occurring in the nasopharynx, are exceedingly rare. This rarity underscores the exceptional nature of such cases and indicates that they do not represent a recognized clinical pattern.
A recent multicenter Chinese cohort study, conducted between 2008 and 2021, comprising 407 HIV-associated lymphoma cases, which is the largest national cohort to date, found that 91.6% were B-cell lymphomas. Among these, diffuse large B-cell lymphoma (DLBCL) represented 73.2%, and Burkitt lymphoma 12.6%. Notably, only four cases (1.0%) were classified as CLL/SLL across all anatomical sites. These findings highlight the extreme rarity of SLL/CLL in HIV-positive patients, particularly in the nasopharynx. 22
Erasmus et al. 9 reported on a hospital-based series of 151 nasopharyngeal biopsies (78 HIV-positive, 32 HIV-negative), systematically compared histological findings according to HIV status. The majority of nasopharyngeal masses in HIV-positive patients were benign lymphoid hyperplasia. 9 Only a small minority were malignant, and SLL was not identified among them. These findings further emphasize the exceptional nature of SLL/CLL at this anatomical site in HIV-positive individuals. 9
A separate bi-institutional cohort of 53 primary aggressive B-cell nasopharyngeal lymphomas from 2 USA centers included DLBCL and related aggressive B-non-Hodgkin lymphoma, but indolent entities like SLL were absent. 23
Large-scale epidemiological data from the Balkan region addressing the occurrence of SLL/CLL in the nasopharynx among HIV-positive patients are currently lacking. To the best of our knowledge, no regional studies specifically examining this entity have been published to date. Consequently, our interpretation relies on available international data and the absence of reported cases in the relevant local literature, which together suggest that nasopharyngeal involvement of SLL/CLL remains exceedingly rare in this setting as well.
From a clinical perspective, continuous monitoring of immune status is essential in these patients to preserve immune system integrity. Equally important is a comprehensive understanding of host responses in the context of multiple coexisting infections, where malignant diseases may exhibit distinct biological behavior and therapeutic responses.
To our knowledge, no comparative study specifically addresses HIV-positive nasopharyngeal B-cell SLL. Therefore, direct comparison is not currently possible. The most appropriate available reference for contextual interpretation would be large cohorts of HIV-associated aggressive B-cell lymphomas, using CD4/CD8 profiles, combined antiretroviral therapy plus immunochemotherapy (e.g. R-CHOP) and survival data as indirect benchmarks to underscore how immunologically typical—but anatomically and histologically exceptional—our patient is.
In our patient, an inverted CD4/CD8 ratio (0.5), reduced CD4+ T-cell counts, elevated absolute CD3+/CD8+ values, and prior IgG seropositivity to EBV/CMV/HSV/VZV are consistent with the typical pattern of advanced HIV-related immunosuppression observed in lymphoma patients (CD4 often <200/μL at diagnosis). In a US HIV-NHL registry (n = 2828, 1996–2010), 90% of patients had AIDS-defining lymphomas with similarly low CD4/CD8 ratios; SLL/CLL was rare (1.1%, 30 cases in total, with no nasopharyngeal cases reported). Head and neck HIV-associated lymphomas show comparable serological profiles, with EBV IgG being almost universal. 24
The good outcome with R-CHOP in this case is similar to improved results seen in HIV-related lymphomas when ART is used: complete response rates for DLBCL/Burkitt are over 70% when CD4 counts are above 100/μL, and 3-year survival rates since the HAART era are around 60%–80%. 25 Standard care also includes prophylaxis for opportunistic infections and careful monitoring of liver, kidney, and blood toxicity, as HIV patients are at higher risk. 25 This patient’s symptom-free status at 1 year (normal nasal breathing, hearing, and smell) is better than averages for low-grade lymphomas without HIV, where 5-year survival is similar to HIV-negative cases but with extra infection risks. ART (tenofovir/lamivudine/dolutegravir) in this case restored immunity effectively, which was not possible in earlier cases without modern therapy.
B-cell lymphoma of the nasopharynx is primarily treated with chemo-immunotherapy (e.g. R-CHOP) and radiotherapy, rather than surgery. Surgery is typically limited to diagnostic or excisional biopsies or to palliative symptom relief, such as securing an airway in cases of obstruction. 12 In the case of the patient we diagnosed and treated, we did not initially suspect that it was a malignant lesion in a patient with acquired immunodeficiency. We came across this data during detailed diagnostics that included several steps. On the other hand, cases of adenoid hypertrophy in adults are not so rare and are not so often associated with lymphoma or viral infections that affect the state of immunity.7,8 That was the only reason one of the first items in our patient’s treatment was the surgical removal of the soft-tissue mass in the nasopharynx.
Conclusion
Most adult cases of adenoid hypertrophy result from recurrent bacterial or viral infections of the nose, sinuses, and nasopharynx, as well as allergic inflammation of the upper airway. Clinicians should consider underlying viral infections such as HIV and EBV, which may promote lymphoid tissue growth. Although rare, malignant transformation of nasopharyngeal lymphoid tissue is possible. B-cell small cell lymphoma with polyclonal plasma cell differentiation represents a minority of malignancies originating from the nasopharynx, and there are limited data regarding epidemiologic and treatment outcomes. Early recognition and thorough evaluation are essential to distinguish benign enlargement from more serious conditions.
Footnotes
Acknowledgements
This case report was performed as a part of the scientific project of the Faculty of Medicine of the Military Medical Academy, University of Defence, Belgrade, Serbia (MFVMA02/23-25/).
Author contributions
Milica Labus: Conceptualization, data curation, writing—original draft preparation, review, and editing. Aleksandar Perić: Conceptualization, data curation, writing—original draft preparation, review and editing, supervision, funding acquisition. Merida Mehmedović: Data curation, writing—original draft preparation, review, and editing. Jelena Sotirović: Data curation, writing—original draft preparation, review, and editing. Stevan Matić: Data curation, writing—original draft preparation, review, and editing. Milena Jović: Data curation, writing—original draft preparation, review, and editing. Biserka Vukomanović Đurđević: Data curation, writing—original draft preparation, review, and editing.
Consent to participate
Written informed consent was obtained from the patient to participate in this study.
Consent for publication
Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Data availability statement
Data sharing is not applicable because of the nature of this study (case report).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
As this study involved human participants, it was reviewed and approved by the Ethics Committee of our institution (Approval number 21/2022).