
Abstract
This pilot study aimed to explore the effectiveness and safety of dexibuprofen suppository in the treatment of PDA in preterm infants. Preterm infants with gestational age <34 weeks and color Doppler echocardiographic evidence of hemodynamically significant PDA (hs PDA) with systemic hypoperfusion was intended to be included into this study since January 2020. As of January 1, 2021, this trial had recruited 87 preterm infants who met the inclusion criteria. Neonates were admitted into hospital within 1 hour after birth and were randomly assigned into two groups. Group one included 44 preterm newborns administered with oral ibuprofen. Group two included 43 preterm newborns administered with dexibuprofen suppository. This preliminary study showed that rectal dexibuprofen and oral ibuprofen were both effective for the closure of PDA, and the closure rate of dexibuprofen suppository was comparable to that of oral ibuprofen after the 1st and 2nd courses of treatment. In addition, rectal dexibuprofen did not increase the incidence of adverse outcomes, including bronchopulmonary dysplasia, intraventricular hemorrhage, sepsis, and necrotising enterocolitis. This pilot study showed dexibuprofen suppository is as effective and safe as oral ibuprofen; yet, better designed, muticenter controlled studies are still needed.
Introduction
At present, very premature infants are becoming common. The relevant risk factors include bacterial vaginosis, multiple pregnancy, advanced age pregnant woman, and assisted reproductive technology.1-2 After birth, a considerable number of premature newborns accompany patent ductus arteriosus (PDA). In a third of premature infants with birthweight less than 2500 g, the PDA remains open, especially during the early days of life (<7 days). 3 And sometimes, the PDA fails to self-close in preterm neonates. But there has been no consensus on clinical or sonographic criteria when treating PDA. The conservative management includes PDA non-treatment,4,5 targeted ventilation strategies, fluid restriction, and diuretic therapy to counteract the effect of PDA shunt.6,7 However, the hemodynamic instability caused by the left to right shunt and associated run off may cause renal or gastrointestinal effects including spontaneous perforation, necrotising enterocolitis (NEC), and bronchopulmonary dysplasia (BPD).8,9 Pharmacological intervention in PDA relies on different agents. At present, paracetamol, ibuprofen, and indomethacin are the common agents to help PDA constriction. 10 And, ibuprofen has been one of the most widely used therapeutic drugs with lower toxicity. According to different reports, oral ibuprofen has comparable efficacy to paracetamol 11 or indomethacin.12,13 In general, non-steroidal anti-inflammatory drugs (NSAIDs) are characterized by small volumes of distribution and high degree of protein binding. 14 However, differences in variability and clearance in half-life are of special relevance in NSAIDs.
Among different NSAIDs, dextrarotatory isomer of ibuprofen—dexibuprofen is the pharmacologically effective enantiomer, which was first launched in Austria in 1994. 15 As one kind of NSAIDs, it was claimed that a dose of 0.75:1 (dexibuprofen and ibuprofen, respectively) would be enough in order to obtain comparable pharmaceutical efficacy. 16 Theoretically, rectal administration is more convenient than oral administration. It could reduce irritation to the stomach. In addition, suppository shows higher absorption and utilization. Moreover, rectal administration does not add to the burden on the liver metabolism. Vilenchik R et al. once compared the pharmacokinetics of oral vs. rectal ibuprofen in healthy volunteers. They found the mean peak plasma concentration of rectal ibuprofen was lower, and the average time to peak was considerably longer. 17 Hadas D et al. also investigated the effectiveness and safety of ibuprofen suppository in 490 children with fever. Each patient received ibuprofen suppository (5–10 mg/kg/dose). And results showed rectal administration of ibuprofen suppository gives overall satisfaction and is well tolerated. 18
But the use of NSAIDs is not without adverse reaction, as their mechanism relies by the effect on the cyclooxygenase cycle, effectively altering the number of vasoconstrictive substances. With the strong net vasoconstrictor effect, several adverse reactions might lead to abnormal cerebral perfusion, renal injury, and NEC. 19 To date, there have been a few studies describing the effectiveness and safety of dexibuprofen suppository in children with fever. But for the treatment of PDA in premature infants, the evidence is largely absent. In view of the above, this randomized controlled trial aimed to find evidence on the effectiveness and safety of rectal dexibuprofen compared to oral ibuprofen for treating PDA in preterm newborns.
Patients and methods
This is a prospective, non-blind, randomized and controlled pilot study.
Preterm infants
As previously reported, the closure of oral ibuprofen for treating PDA is around 77.6%. 20 Based on that study, it was estimated that the closure rate of oral ibuprofen is around 78%. This study adopted a non-inferiority design with α = 0.05 and 1-β = 0.80. The sample size ratio of the two groups was designed as 1:1. We used Pearson Chi-square test by SAS software (9.4) to calculate the sample size. The sample size of oral ibuprofen group and rectal dexibuprofen group is 95, respectively.
Inclusion criteria: Preterm infants with gestational age <34 weeks and color Doppler echocardiographic evidence of hemodynamically significant PDA (hs PDA) with systemic hypoperfusion was intended to be included into this study since January 2020. As of January 1, 2021, this trial had included 87 preterm infants who met the inclusion criteria. Here, we summarize the results of this phase into a pilot report. The included neonates were admitted to the neonatal intensive care unit (NICU) of Jiangsu Maternal and Child Health Hospital, Nanjing Medical University, which is a representative Grade III NICU in Jiangsu province, East of China. Exclusion criteria: Before medication, patients with abnormal coagulation function, intraventricular hemorrhage (IVH) ≥ grade III, non-hs PDA, urine output less than 1 mL/kg/hour for 24 consecutive hours, acute kidney injury, inherited metabolic diseases, duct-dependent congenital heart disease or major congenital anomalies were excluded. The written informed consent has been obtained from parents. Study protocol was approved by the Ethical Committee of Jiangsu Maternal and Child Health Hospital (Number: 202004037-1). This study conforms to CONSORT 2010 statement 21 with a checklist (Supplementary).
A total of 812 preterm infants with PDA were hospitalized in our NICU after birth; 725 were excluded as showed in flow chart (Figure 1). Finally, 87 preterm infants were randomly assigned into two groups. Random number table method was used for randomization. Group one included 44 preterm newborns using oral ibuprofen, and group two included 43 preterm infants with dexibuprofen suppository (Figure 1). Flow chart of this study.
Data collection
All enrolled infants were admitted to hospital within 1 hour after birth. After admission, clinical data were collected by two neonatologists and checked by a third person. The data contain mother’s age, gestational age, gender, birthweight, 5 min Apgar score, diagnosis, blood gas, respiratory support, outcomes, etc. Laboratory investigations included albumin
Clinical outcomes
Primary outcomes include PDA closure after 1st course, PDA closure after 2nd course and need for surgical ligation. Secondary outcomes include duration of mechanical ventilation, mortality, IVH, NEC, gastrointestinal bleeding, sepsis, and BPD. BPD is defined as a requirement for oxygen at 36 weeks PMA.23,24 IVH is defined and classified according to the literature reported by Papile LA 1978 and Volpe JJ 2008.25,26 NEC is defined and classified according to Bell’s staging criteria. 27
Echocardiographic measurement
Echocardiographic measurements were screened at the third day after birth by attending physicians using Vivid E9 ultrasound scanner (GE Company, USA). It was performed initially before treatment, and later detected after 3 days to estimate the ejection fraction, pulmonary artery systolic pressure, internal diameter of the duct size, left to right shunting of blood, end diastolic reversal of blood flow in aorta. Hs PDA was defined by the presence of systemic hypoperfusion combined with at least one of the following criteria: Left-atrium to-aortic-root ratio in moderate PDA between 1.4 and 1.6, and >1.6 in large PDA; Internal ductal diameter ≥ 1.5 mm; Left pulmonary artery diastolic flow velocity > 0.25 m/sec; Left ventricular output >300 mL/kg/min; Low antegrade flow in systole or diastole; Reverse or absent diastolic flow in the descending aorta.28,29 Surgical PDA ligation was considered while treatments of echocardiographically confirmed hs PDA failed. 30 The judgment criteria for PDA closure are that there is no abnormal shunt in color Doppler blood flow imaging and spectrum Doppler ultrasound fails to detect continuous shunt spectrum.
Medicine administration
The enrolled neonates were randomly assigned to oral ibuprofen group or dexibuprofen suppository group. Patients received oral ibuprofen (Ibuprofen suspension 20 mg/mL; Johnson & Johnson Company, China) 10 mg/kg/d for the first day, followed by 5 mg/kg/day for two consecutive days. A second course of oral ibuprofen was given for three more days (10–5–5 mg/kg/day) if the duct was still significantly patent. Because a dose of 0.75:1 (dexibuprofen and ibuprofen, respectively) would be enough in order to obtain comparable pharmaceutical efficacy. 16 Patients received dexibuprofen suppository (Dexibuprofen suppository 50 mg/each dose; Dayin Company, China, www.dynemed.com.cn) 7.5 mg/kg/d for the first day followed by 3.75 mg/kg/day for two consecutive days. A second course of suppository was given for three more days (7.5–3.75–3.75 mg/kg/day). As an off-label drug, dexibuprofen suppository used in this study is originally designed for treating fever in children. The approval number is H20010642 which has been awarded by China Food and Drug Administration (Executive standard WS-225 (X-200)–2001-2014Z).
Statistical methods
Statistical analysis was performed using SPSS 13.0 software. Quantitative data which obey normal distribution were showed as mean and standard deviation. The comparison between the two groups used t or t’ test. Quantitative data which obey skew distribution were showed as median and quartile. The comparison between the two groups used Wilcoxon Rank Sum test. For qualitative data, Pearson Chi-square test, Likelihood ratio test, or Fisher’s exact test were performed. p < 0.05 was considered statistically significant.
Results
Analysis of baseline data
Baseline data of the two groups.

aSGA, means small for gestational age. AGA, means appropriate for gestational age. LGA, means large for gestational age.
bPROM means premature rupture of membranes. ‡LR means likelihood ratio.
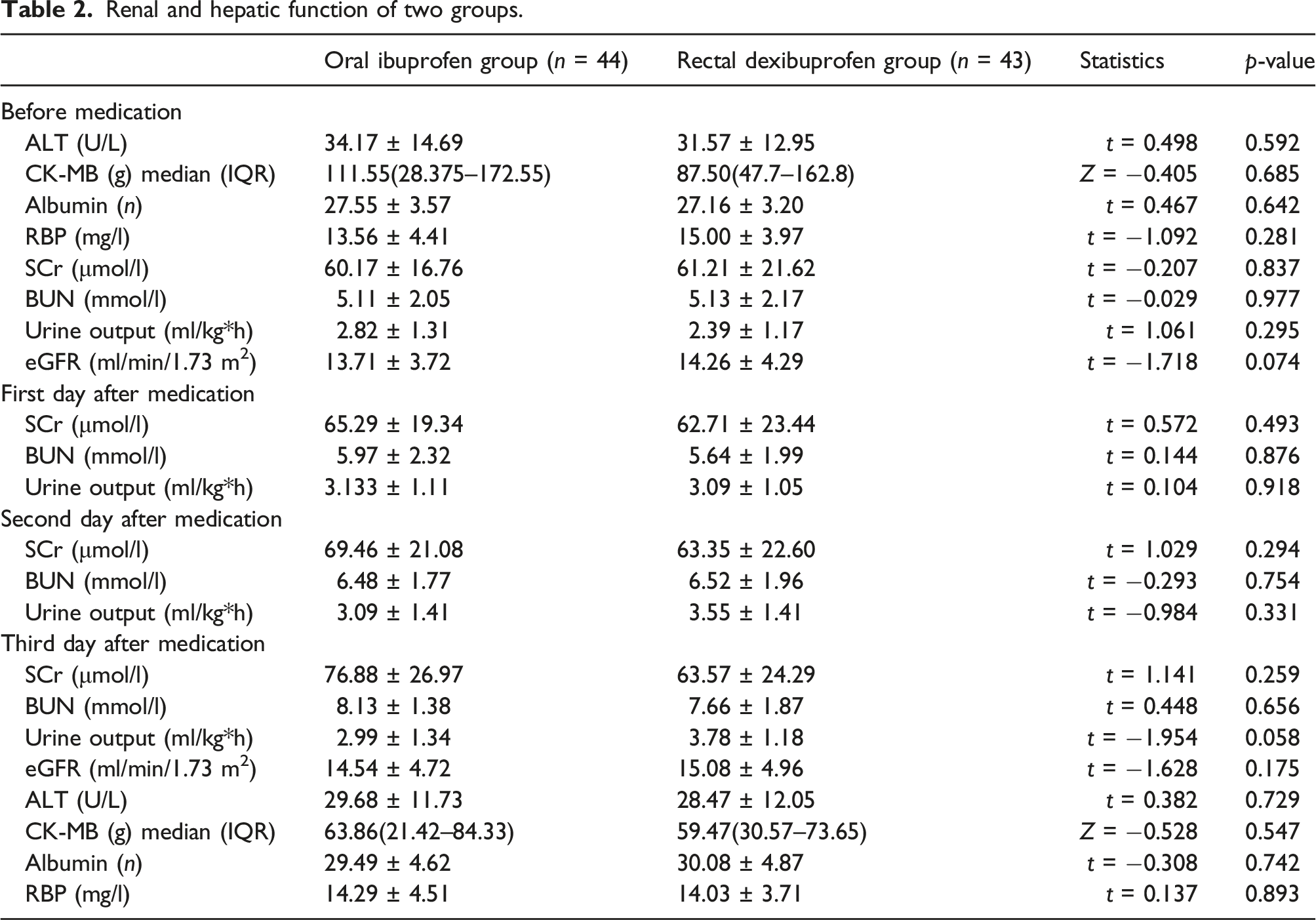
Renal and hepatic function of two groups
Renal and hepatic function of two groups.
Clinical outcomes
Clinical features of the two groups.

aCMV means conventional mechanical ventilation
bHFV means high frequency ventilation; ‡LR means likelihood ratio.
Discussion
A common early cardiovascular problem of prematurely born infants is hs PDA. The utility of active management and the timing and modality of PDA treatment have been debated. Two updated Cochrane meta-analysis compared placebo or no treatment with ibuprofen or paracetamol, it was found that there was no increase in the duration of mechanical ventilation, or incidence of mortality, NEC, chronic lung diseases, IVH, and periventricular leukomalacia.31,30 In contrast, other reports showed persistent ductal shunting may lead to pulmonary overcirculation, increasing the risk of BPD; conversely, shunting may induce systemic hypoperfusion, increasing the risk of NEC, IVH, renal failure, and death.32,33 Over the past years, NSAIDs along with other pharmacotherapeutic agents have been used to treat PDA to reduce such complications. Kluckow et al. once performed a placebo‐controlled randomized trial and demonstrated that preterm infants <29 weeks with a large PDA who received indomethacin versus placebo within 12 hours of birth had significantly lower incidence of early pulmonary hemorrhage (2% vs 21%). 34
Dexibuprofen is the active enantiomer of the widely used ibuprofen. Ibuprofen and dexibuprofen differ in the physico-chemical properties according to pharmacological properties and metabolic profiles. In our unit, dexibuprofen suppository was not used as the first choice but rather as an alternative treatment for closing hs PDA when not applicable to ibuprofen (such as feeding intolerance). In the past several years, dexibuprofen suppository has been mainly used to treat children with fever. 35 Therefore, to test the hypothesis of whether dexibuprofen suppository is as effective as ibuprofen for closing hs PDA, we conducted this prospective, randomized controlled trial in preterm infants to evaluate the effectiveness and safety of dexibuprofen suppository.
Compared with other NSAIDs, ibuprofen has less adverse effects. The latest meta-analysis showed that compared to indomethacin (intravenous or oral), the risk of NEC was decreased in oral ibuprofen group (7 studies, 249 infants; typical RR 0.41, 95% CI 0.23–0.73). 36 However, when preterm infants suffer from feeding intolerance, the application of oral ibuprofen is often restricted. Rectal administration could reduce the adverse effects on digestive tract. And it does not add to the burden on the liver metabolism. Based on this, rectal administration could be used as a promising alternative way for medication.
Zamani O et al. performed a multicenter, non-inferiority, observer-blinded study. 489 patients with painful osteoarthritis of the hip or knee were included to explore the safety and tolerability of dexibuprofen vs. ibuprofen powder for oral suspension. The result showed that at least non-inferiority in terms of safety and efficacy for the dexibuprofen application. 37 The result from Choi SJ’s study showed there were no significant differences in decreasing body temperature between propacetamol group and dexibuprofen group. So, dexibuprofen is considered as an effective and safe choice for treating pediatric upper respiratory tract infection (URTI) patients with fever. 38 Kim CK et al. reported a double-blind and dummy study presenting at one of five tertiary care centers. It’s found that dexibuprofen as tolerable and effective as ibuprofen for fever in children. 39 In addition, compared to ibuprofen 400 mg, Kollenz C et al. found both dexibuprofen 200 mg and 300 mg showed a trend towards superiority for sum of pain intensity difference and total pain relief. 40 Furthermore, Liao L et al. included 311 URTI children with body temperature higher than 38.5°C. They also reported rectal ibuprofen is as effective as oral group in Chinese patients. 41
Conclusion
This pilot study showed that dexibuprofen suppository was effective as oral ibuprofen for the closure of PDA, and the closure rate of dexibuprofen suppository was comparable to that of oral ibuprofen after the 1st and the 2nd courses of treatment. In addition, dexibuprofen suppository did not increase the incidence of adverse events, such as BPD, IVH, sepsis, and NEC.
Limitations
However, we must note additional limitations of our research. For example, there is still a lack of randomized controlled trials related to dexibuprofen suppository. As a pilot study, the measured data of cardiovascular function scanned by ultrasound are still being collected and analyzed, and the measurements were not included in this paper. Considering the potential heterogeneity of hs PDA measured data, more appropriate statistical methods would be adopted. In addition, the inclusion criteria in this study are preterm infants with gestational age less than 34 weeks. However, current studies have mainly focused on PDA closure in infants with gestation age less than 28 weeks. So, the sample size will be further expanded to include more very premature babies in the future study.
Supplemental Material
Supplemental Material - Effectiveness and safety of rectal dexibuprofen versus oral ibuprofen for closure of patent ductus arteriosus in preterm infants with gestational age<34 weeks: A pilot study
Supplemental Material for Effectiveness and safety of rectal dexibuprofen versus oral ibuprofen for closure of patent ductus arteriosus in preterm infants with gestational age<34 weeks: A pilot study by Jing-jing Pan, Yang Yang, Shu-dong Cui, Xiao-qing Chen and Xiao-guang Zhou in International Journal of Immunopathology and Pharmacology
Footnotes
Acknowledgements
The authors would like to thank the parents for their understanding.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Young Talents Startup Fund of Jiangsu Maternal and Child Health Hospital, China (FYRC202012 Q,C.).
Ethics approval
Ethical approval for this study was obtained from the Ethical Committee of Jiangsu Maternal and Child Health Hospital (Number: 202004037-1).
Informed consent
Written informed consent was obtained from the parentsbefore the study.
Trial registration
This randomized clinical trial was not registered because it was a pilot study.
Supplemental Material
Supplementary material for this article is available on the online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.