
Abstract
Objectives
Pericardial effusion is a rare clinical manifestation in idiopathic inflammatory myopathies (IIMs). It has been described in a small number of literature studies worldwide. We describe the clinical and laboratory characteristics of 19 IIM patients combined with pericardial effusion, and compare them with previously reported cases. The single-center observational-study-inspired collected of 156 IIM patients with complete data from January 1, 2016 to January 1, 2021 in the First Affiliated Hospital of Xinjiang Medical University, of which 19 patients had pericardial effusion.
Methods
The clinical characteristics of 19 IIM patients complicated with pericardial effusion were investigated by descriptive analysis and compared with previously reported cases.
Results
19 cases of IIM patients had pericardial effusion (12.2%), patients without a large amount of pericardial effusion or pericardial tamponade. There was a predominance of women in the patients with 78.9% pericardial effusion . In the clinical examination, 10 cases showed chest tightness (52.6%), pulmonary fibrosis (47.4%), and the frequency of muscle nuclear magnetic, which suggested that muscle lymphocyte infiltration rate was 63.2%. Anti-Ro-52 antibody and anti-Jo-1 antibody were positive (26.3%, 42.1%). IIM patients with pericardial effusion were accompanied by decreased serum albumin levels and elevated ESR. In the literature review, the most common clinical characteristics of IIM patients with pericardial effusion were female, pulmonary fibrosis, shortness of breath, positive anti-Ro-52 pulmonary fibrosis, and anti-Jo-1 antibody.
Conclusion
In the study, 19 patients of IIMs with pericardial effusion present with chest tightness, and are accompanied by pulmonary fibrosis, positive anti-Jo-1 antibody, and anti-Ro-52 antibody. It is suggested that pericardial effusion in IIM patients may be related to anti-synthetase antibody.
Keywords
Introduction
Idiopathic inflammatory myopathies (IIMs) are a group of autoimmune diseases with proximal muscle weakness, rash, and myalgia as the main manifestations. It mainly includes clinical subtypes such as dermatomyositis, polymyositis, and amyopathic dermatomyositis.1–5 The pathogenesis of IIM is still unclear, but a series of factors such as genetic susceptibility, environmental triggers, immunity, and medication history play a role in the development of the disease. IIMs may affect muscles, skin, joints, esophagus, lungs, heart, and other tissues and organs. Common complications of IIMs include interstitial lung disease, cancer, arrhythmias, and thrombosis, resulting in poor prognosis and increased mortality. The first symptoms are mostly rash and muscle weakness of proximal extremities.6,7
Heart involvement is one of the common complications of IIMs, mainly manifested as left ventricular diastolic dysfunction, arrhythmia, and conduction block. Pericardial effusion is uncommon, and the clinical symptoms are often insidious, that is mostly discovered accidentally. Therefore, it is easy to be ignored by patients and doctors, leading to irreversible dysfunction and even death. Autoimmune disease is one of the causes of pericardial effusion.8–11 There has been a lot of research on the clinical features of myositis with interstitial lung disease, cancers, and thrombosis. However, there were few studies on IIMs complicated with pericardial effusion at home and abroad. Therefore, this study analyzed the general data, clinical features, laboratory findings, and imaging features of IIMs combined with pericardial effusion, as well as, compared them with previously reported cases.
Materials and methods
Patients
This single-center observational-study-inspired was conducted in the First Affiliated Hospital of Xinjiang Medical University; using data collected from the health information base and patient anonymity, the subject which met the Helsinki declaration cannot be found. 156 patients with IIMs were collected from January 1, 2016 to January 1, 2021, which had complete data.
According to the diagnostic criteria for IIMs and echocardiography results, which were assessed by two experienced clinicians, 19 patients met the study criteria. The diagnosis met the Bohan/Peter criteria 8 and ENMC (European Neuromuscular Center) criteria. 12 Pericardial effusion was assessed by echocardiography.
Data
Clinical data were obtained through a retrospective review of medical records. The general information of the patients was recorded, including gender, ethnicity, age, age of first episode, course of disease, blood pressure, and body mass index (BMI); clinical manifestations, such as sun rash, Gottron sign, Gower sign, mechanic hand, erythema of the nail, V-sign, and muscle strength; the patient’s laboratory test results when visiting our hospital, including blood routine, biochemical analysis, coagulation analysis, inflammatory factors, and erythrocyte sedimentation rate; immunological indicators: (1). Antibodies related to IIMs, including anti-RO-52 antibody and anti-polyphoteric/hard skin (PM/SCL) 75/100 antibody; (2). Anti-histidine-specific antibody, antibodamyl TRNA synthetase (Jo-1) antibody, anti-threonyl TRNA synthetase (PL-7) antibody, antanetyl TRNA synthetase (PL-12) antibody, anti-glycyl TRNA synthetase (EJ) antibody, anti-hemineyl TRNA synthase (OJ) antibody, anti-melanoma differentiation related gene 5 (MDA5) antibody, and anti-nuclear matrix protein 2NXP2) antibody; Imaging examination and others: heart ultrasonic heart map, neck vascular ultrasound, muscle nuclear magnetic, high resolution CT etc. We collected all data that met the inclusion and exclusion criteria in the past 5 years for comprehensive analysis. The data were checked by two researchers to ensure accuracy. An experienced clinician was invited to assist in the assessment to address potential biases.
Ethics
With the approval of the Ethics Committee of First Affiliated Hospital of Xinjiang Medical University (K202110-01), we conducted the retrospective study that met the Helsinki Declaration.
Literature review
We searched the English-language literature in the PubMed database and EMBASE (Library of Xinjiang Medical University) for all related articles, using the following four key words: idiopathic inflammatory myopathies, IIMs, pericarditis, and pericardial effusion.
Statistical analysis
SPSS26.0 statistical software was used. Data in line with normal distribution used average ±standard deviation, and data that did not meet normal distribution were indicated by the median and percentile.
Results
Clinical and antibodies features of 19 idiopathic inflammatory myopathies patients with pericardial effusion
Clinical and antibodies features of 19 idiopathic inflammatory myopathies patients with pericardial effusion.
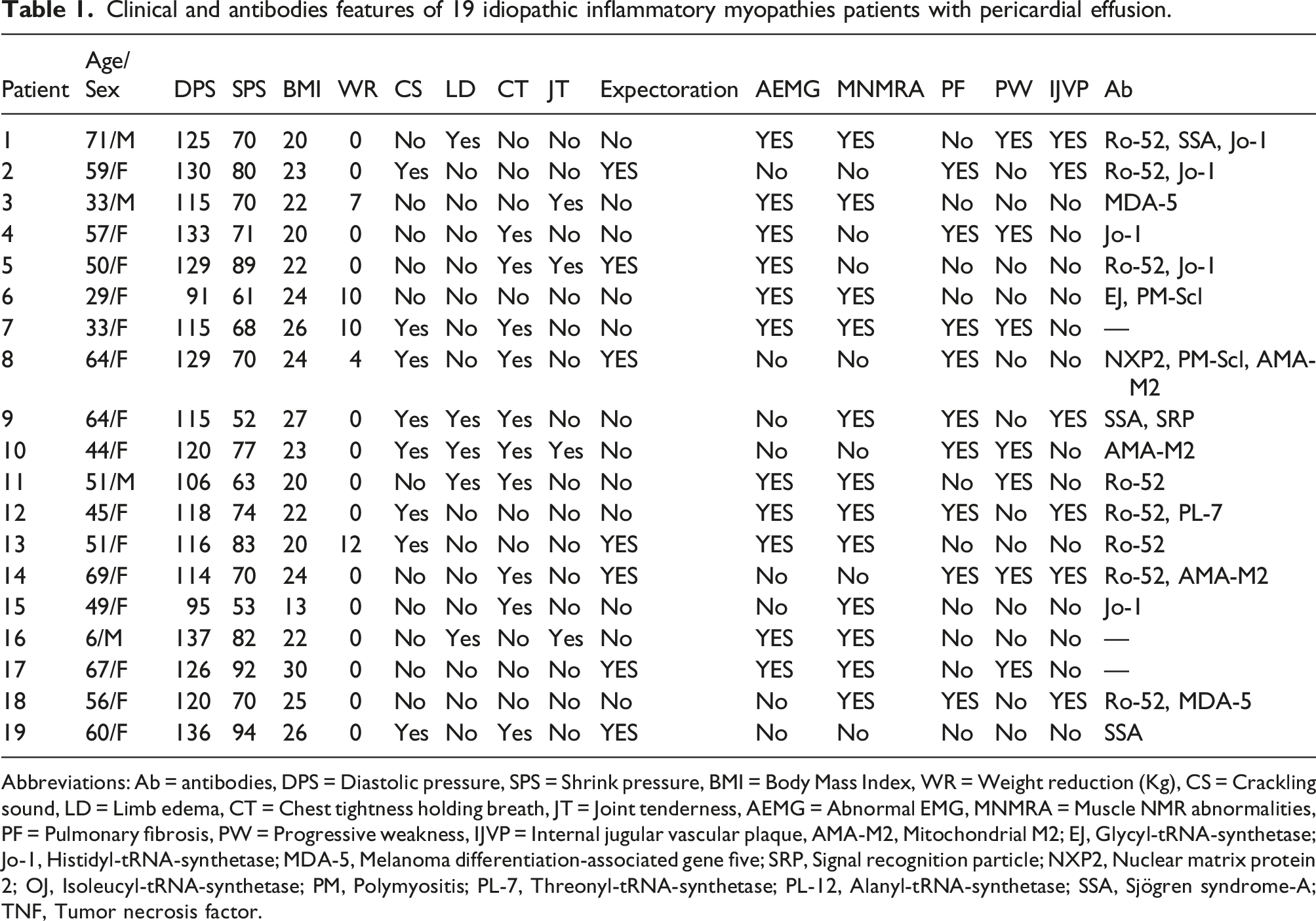
Abbreviations: Ab = antibodies, DPS = Diastolic pressure, SPS = Shrink pressure, BMI = Body Mass Index, WR = Weight reduction (Kg), CS = Crackling sound, LD = Limb edema, CT = Chest tightness holding breath, JT = Joint tenderness, AEMG = Abnormal EMG, MNMRA = Muscle NMR abnormalities, PF = Pulmonary fibrosis, PW = Progressive weakness, IJVP = Internal jugular vascular plaque, AMA-M2, Mitochondrial M2; EJ, Glycyl-tRNA-synthetase; Jo-1, Histidyl-tRNA-synthetase; MDA-5, Melanoma differentiation-associated gene five; SRP, Signal recognition particle; NXP2, Nuclear matrix protein 2; OJ, Isoleucyl-tRNA-synthetase; PM, Polymyositis; PL-7, Threonyl-tRNA-synthetase; PL-12, Alanyl-tRNA-synthetase; SSA, Sjögren syndrome-A; TNF, Tumor necrosis factor.
Laboratory characteristics of IIM patients combined with pericardial effusion
Laboratory test results of patients with IIMs.

Connective tissue disease associated markers.

Literature review
Main characteristics of patients with pericardial effusion/pericarditis, previous and present reports.

Discussion
The heart involvement is the most important cause of death in patients with IIMs, such patients may experience heart conduction block, supraventricular arrhythmia, or cardiomyopathy, which may cause syncope, congestive heart failure, etc. Some studies have suggested that autoimmune diseases can cause pericardial effusion, which is a subclinical heart damage in patients with IIMs, this may be related to the decline of right heart function, but it cannot be ruled out that it is a chronic non-suppurative inflammatory reaction in which a large number of inflammatory cells infiltrate the primary disease.10,11,21,22 Among them, IIMs with pericardial effusion is easy to be ignored in clinical practice, except that pericardial effusion caused by autoimmune diseases is usually small in volume and hemodynamics are not significant, it is also considered that this is related to the lower incidence of IIMs itself. 13
In this study, we analyzed the clinical and laboratory characteristics of patients with IIMs complicated with pericardial effusion at First Affiliated Hospital of Xinjiang Medical University over a 5-year period. There are few cases of IIMs with pericardial effusion. Due to the small sample size, some clinical features may have been over-amplified, so we also included a review of published cases in the literature to overcome these problems. Studies have suggested that the frequency of IIMs with pericardial effusion is 12.37%–17%, 23 which is similar to the 12.2% in this study, and similar to other studies, the patients with pericardial effusion in our collected cases are all small or moderate pericardial effusions (small effusion is 50–100 mL, moderate effusion is 100–500 mL, and large effusion> 500 mL); however, if there is no large amount of pericardial effusion or pericardial tamponade,7,24–27 it is more reliable.
In our current research, nine of the patients with pericardial effusion had pulmonary fibrosis (47.4%) and presented pulmonary crackles on auscultation (42.1%). Some case reports showed that patients with pericardial effusion have rapidly progressive interstitial lung disease, or they came with each other.13–15,28 Crackling sounds are a common sign of interstitial lung disease, it is considered to be related to the severity of interstitial lung disease and the sample size.
Anti-Jo-1 antibody was significantly related to pulmonary hypertension, which could cause lung damage and heart damage, anti-Jo-1 antibody could also act as a chemotactic factor to induce cell damage mediated by T cells, 13 at the same time, pericardial effusion would compress the surrounding lung tissues, affected the gas exchange of the respiratory system, and reduced the cardiac output, which could cause chest tightness, shortness of breath, edema, and other symptoms in patients. In this study, among the 19 patients with pericardial effusion, 26.3% had positive Jo-1 antibody, while about 8.8% of the patients without pericardial effusion had positive Jo-1 antibody. Also, patients with pericardial effusion had a significantly higher proportion of chest tightness compared with patients without pericardial effusion. A multicenter study of 18 patients followed for 2.8–10.7 years suggested pericardial effusion as a possible manifestation of association with anti-PL-7 antibodies. 29 There were 25 IIM samples in our study, and there was one pl-7 positive sample in both groups (p = 0.100), considering the reasons of insufficient sample size and short follow-up time.
In addition, IIMs combined with pericardial effusion can cause muscle inflammatory infiltration and decreased serum albumin (34.36 g/L), which could lead to limb edema, 30 at the same time, tissue and organ damage was related to the activity of IIMs, and the disease activity of IIMs depended largely on the intensity of the inflammatory response, and some studies have shown that serum albumin is negatively correlated with indicators representing IIMs activity,31,32 which was similar to this study in the combined pericardial effusion group; ALB was reduced in the muscle NMR results, patients in the group with pericardial effusion had a higher proportion of muscle lymphocyte infiltration.
There were few cases of IIMs complicated with pericardial effusion, and few studies have focused on the clinical characteristics and auxiliary examination characteristics of these patients. We used the four keywords: idiopathic inflammatory myopathies, IIMs, pericarditis, and pericardial effusion, to search in two English databases (PubMed and EMBASE), and eight literatures met the requirements. They included 1 (1/13, 7.7%), 8 (8/96, 8.3%), and 10 (10/271, 3.7%) patients, additionally adding five case reports, for a total of 25 patients.13–20 Anti-synthetase syndrome is described classically by the triad of interstitial lung disease, inflammatory myositis, and presence of aminoacyl-tRNA synthetase antibodies. In common with other reported IIM patients with pericardial effusion more prevalent in women, pulmonary fibrosis and positive anti-Jo-1 antibody were the most frequent manifestations, and these common features were confirmed in a review of all cases published to date in the literature. It is suggested that pericardial effusion in IIM patients may be related to anti-synthetase antibody. In addition, muscle weakness, elevated creatine kinase, positive anti-Ro-52 antibody, and PL-7 were also present in a subset of patients.
The study also had several limitations: First, there was a lack of extensive literature and guidelines on pericardial effusion associated with idiopathic inflammatory myopathy. Second, it was a retrospective observational-study-inspired. Further prospective studies were needed to verify the conclusions of this study. Next, this study did not carry out the calculation and demonstration of the selected sample size, but we collected of all IIM patients with complete data from January 1, 2016 to January 1, 2021 in the First Affiliated Hospital of Xinjiang Medical University. Because IIMs were a rare disease with few cases to look for, the data available may not be comprehensive and may result in bias for a more complete assessment of the disease. In the future, we would include a larger number of samples from multiple regions to further explore the clinical manifestations and epidemiological characteristics of pericardial effusion in IIMs.
Conclusion
In summary, like other reported IIM patients with pericardial effusion, most of the IIM patients with pericardial effusion were female, and complicated with chest tightness, pulmonary fibrosis, positive anti-Jo-1 antibody, and anti-Ro-52 antibody. It is suggested that pericardial effusion in IIM patients may be related to anti-synthetase antibody and anti-Ro-52 antibody, which needs to be confirmed by our future studies.
Footnotes
Acknowledgements
The authors wish to thank all the persons who participated in this study, including the reviewers and medics.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation (81760800). Scientific Research Project of Science Department of Xinjiang Autonomous Region (2019D01C327).
Ethical approval
Ethical approval for this study was obtained from *NAME OF ETHICS COMMITTEE OR INSTITUTIONAL REVIEW BOARD (APPROVAL NUMBER/ID)*. With the approval of the Ethics Committee of First Affiliated Hospital of Xinjiang Medical University (K202110-01), we conducted the retrospective study that met the Helsinki Declaration.
Informed consent
Informed consent was not sought for the present study because *REASON*. We performed a retrospective study, collecting data from the health information base, and did not involve any prospective collection of data or patient interventions. The patient is anonymous, the subject cannot be found, the rights and welfare of the subject will not be adversely affected, and the research project does not involve commercial interests. So, we applied to exempt informed consent for study participants. Our research followed the guidelines outlined in the Declaration of Helsinki.