
Abstract
Background
Thalassemia is a hereditary hemolytic anemia marked by a defect in synthesizing one or more globin chains in hemoglobin. In Pakistan, approximately 10,000 patients with thalassemia are primarily dependent on blood transfusions. The β-thalassemia patients require blood transfusions and iron chelation therapy. Patients who need blood transfusions are at an increased risk of contracting transfusion-transmitted infections (TTIs) such as hepatitis B and C viruses (HBV and HCV, respectively), as well as the human immunodeficiency virus (HIV).
Objective
This systemic review aims to assess the prevalence of TTIs in transfusion-dependent β-thalassemia patients in Asia.
Methods
The data for the systematic review were gathered from PubMed, Google Scholar, the Directory of Open Access Journals (DOAJ), and ScienceDirect using the following keywords: “prevalence, HBV, HCV, HIV, thalassemia, and transfusion-transmitted infections (TTIs)," and so on. This review includes the research articles that address the prevalence of viral infections in thalassemic patients following blood transfusion.
Results
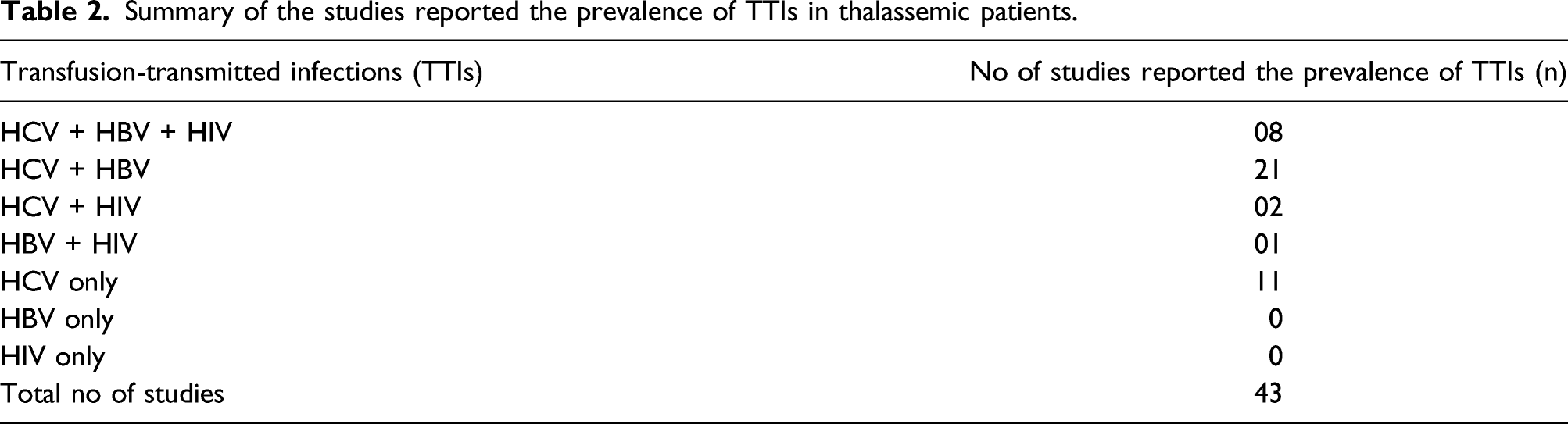
A preliminary search of various databases identified 231 potential studies. 157 duplicate studies were eliminated, and the eligibility of 59 full-length articles was determined. Only 43 studies met the inclusion criteria. Among the 43 studies analyzed, 11 reported a high prevalence of HCV alone in thalassemic patients, while 21 reported a high prevalence of HCV and HBV infection in thalassemic patients. Eight studies reported the prevalence of all three TTIs examined, namely, HCV, HBV, and HIV, in patients with transfusion-dependent thalassemia.
Conclusion
Preventable transfusion-transmitted infections occur frequently, and robust national policies and hemovigilance are required to detect and mitigate the infection risk.
Introduction
Thalassemia is one of the most common genetic abnormalities worldwide, affecting approximately 3% (1.5 million) of the population and resulting in serious health problems such as increased morbidity and premature death and financial and emotional strain on affected families. Thalassemia is a group of hereditary hemolytic anemias defined by the defective synthesis or absence of one or more globin chains of hemoglobin. Thalassemia is classified into two types: alpha (α) and beta (β). Beta thalassemia is caused by a mutation in the beta-globin gene, whereas alpha thalassemia is caused by a mutation in the alpha-globin gene. 1
The breakdown of RBCs characterizes β-thalassemia because of defective synthesis of the β-globin chain leading to the complete absence of βo or reduced synthesis of β+ in β-globin chains. Clinically, β-thalassemia is classified into three major subtypes depending on disease severity. These subtypes include transfusion-dependent β-thalassemia major (BTM), moderate β-thalassemia intermedia (BTI), and asymptomatic β-thalassemia trait (BTT). 2 Thalassemias is more prevalent in parts of Africa, the Middle East, Southeast Asia, the Mediterranean Basin, the Indian subcontinent, and Pacific Islands,3,4 which range from 1 to 20% as a carrier in these areas. Figures showed that around 270 million people globally are the carriers of variant hemoglobins, approximately 80 million people are β-thalassemia carriers. About 300,000 to 400,000 babies are born annually with a severe hemoglobin disorder, of which 23,000 suffer from thalassemia major, with almost 90% occurring in low-resource countries.5,6 Patients affected with thalassemia major require blood transfusions regularly for their survival.
The cornerstone therapy in improving the lifespan and the existence of thalassemic patients is the safe and adequate blood transfusions with regular iron chelation. Suboptimal screening of donors or testing and blood processing will increase the risk of additional complications such as transfusion-transmitted infections. Blood transfusion practices challenge the life of thalassemia patients and can cause new medical problems such as transfusion-transmitted infections like HCV, HBV, HIV, and syphilis infections.7,8
In developing countries, the lives of β-thalassemic patients remain more prone to TTIs as they need frequent blood transfusions for their survival due to unreliable screening tests for blood donors with non-compliance with bio-safety standards. 9 Repeated transfusions could cause further difficulties, like iron overload, since it is not monitored appropriately. However, relatively safe blood transfusion methods are adopted in the developed world due to highly sensitive screening techniques for blood donors such as nucleic acid technology to minimize the chances of infectious blood units being collected during the “window period.” 10 Chiavetta et al. (2003) 11 reported an estimated risk of TTIs in developed countries including Canada, USA, and other European countries are less than 2.5% for each one million contributions. Whereas developing countries still have not integrated the critical requirements for practicing the modern blood transfusion processes. 12
HBV is one of the most widespread viral infections13,14 and is considered the 10th most common cause of death. An expected one-third of the biosphere’s population has serological evidence of HBV infection. 15 The most frequent symptoms of hepatitis B are nausea and jaundice; however, the clinical picture varies among individuals.16,17 One patient dies after 30–45 s due to HBV infection. According to The Center for Disease Control and Prevention (CDC) USA, HBV is 10 times more contagious than HCV and a hundred times than HIV.18,19 Studies reported that large numbers of individuals have asymptomatic, chronic, and occult hepatitis B infection (OBI).14,20 Thalassemia patients are at risk of infection due to frequent blood transfusion along with its constituents. 21 To minimize the spread of HBV infection, most blood transfusion services use an ELISA test for HBsAg detection during donor screening. Despite this, cases of post-transfusion hepatitis have been reported, indicating that the ELISA technique is not entirely effective. HBsAg test is a rapid test routinely used for screening blood donors which is a simple qualitative test and the result is read visually within few minutes. This test is not reliable because of its lower sensitivity and specificity, and subjective evaluation of its result. Nucleic acid amplification technology (NAT) test is an advanced molecular test which detects specific target DNA/RNA segment of the virus amplified in vitro, enabling the detection of low levels of virus in blood sample by increasing the specific target RNA/DNA present in detectable level. NAT testing is the highly recommended and reliable method of donor screening in developed countries.22,23
HCV is an RNA virus from the hepacivirus genus and belongs to the family Flaviviridae. It is a hepatotropic virus. Nearly 180 million people are infected with chronic hepatitis with a prevalence of around 2%, and about 3–4 million individuals are being infected every year globally. Six genotypes have been recognized amongst the hepatitis C virus identified worldwide.24,25 Prevalence of HCV in β-thalassemia patients have been reported in published studies conducted on multi-transfused thalassemia patients.26,27 The higher risk of HCV infection in β-thalassemia patients is mainly linked with the mean age of the patients, mean duration, and the extent of blood transfusion. HCV virus is the most prevalent infection in thalassemic patients worldwide, and in Pakistan, 2.2–14% prevalence of HCV infection is described. 28
Human immunodeficiency virus (HIV) infection and acquired immune deficiency syndrome (AIDS) are caused by HIV, 29 which belongs to a subdivision of retrovirus called lentivirus. HIV is transmitted from infected people through exchanging various body fluids such as blood, semen, breast milk, vaginal secretions, and from mother to child during pregnancy and delivery. Risk factors for the transmission of HIV include unprotected sex, needle stick injuries, unsafe blood transfusion, and tissue transplantation. 30 The transmission risk for the spread of HIV infection through the transfusion of screened blood is minimal. Also, there is a marked reduction in the likelihood of HIV transmission via blood transfusion due to the usefulness of new screening tests. 31 By 2009, UNAIDS Pakistan and National AIDS Control Programme assessed that nearly 130,000 HIV cases in Pakistan had been identified, with an overall prevalence of less than 0.05% in the general population. The frequency of TTIs in transfusion-dependent β-thalassemic patients will be reduced by following the upgraded parameters of blood banks by using globally approved kits to screen donor blood before transfusion to the patients. Furthermore, strict serological blood screening for TTIs before transfusion must be applied in blood banks. 32
This systemic review aims to assess the prevalence of TTIs in transfusion-dependent β-thalassemia patients from Asia.
Material and methods
Literature search, inclusion criteria, and data extraction
The data for the present systematic review was collected from PubMed, Google Scholar, Science direct, PakMediNet, Digital Libraries, and Directory of Open Access Journals (DOAJ) search engines by using the keywords: “Prevalence, HBV, HCV, HIV, Thalassemia, Blood transfusion, Transfusion-transmitted infections (TTIs), Frequent transfusion, and Repeated blood transfusion complications.” All the research articles addressing the prevalence of viral infections amongst thalassemic patients following blood transfusion published during the last 20 years were included. All the studies either reporting the prevalence of all the three types of TTIs, that is, HBV, HCV, and HIV or either one or two of these infections in thalassemic patients were included in the study. Studies reporting other coinfections in thalassemic patients or no coinfection were excluded from the study. In contrast, those studies reporting coinfection of HBV, HCV, and HIV without thalassemia were also excluded from the current systematic review. Those studies were excluded if they were published other than the English language, such as review articles, editorials, letters, and commentaries. Initial search through different databases retrieved 231 studies. After duplicate removal, 157 studies were reviewed, out of which 59 full-text articles with relevant studies were assessed for eligibility while 98 studies were excluded with reasons, as shown in the Prisma flow chart (Figure 1). Only 43 studies on TTIs in thalassemic patients fulfilled the inclusion criteria for this systematic review and were analyzed. Prisma 2009 flow chart summary of selection process.
Statistical analysis
Data were extracted from all the searched articles and then entered into Microsoft Office Excel 2013. The extracted data was then analyzed for the frequency percentage of the transfusion-transmitted infections (TTIs) in thalassemic patients.
Results
A preliminary search of various databases identified 231 potential studies for the current systematic review. 157 of these were duplicates and were therefore excluded from the study. After excluding 98 studies for various reasons, there were 59 full-length articles assessed for eligibility. Only 43 studies involving 12,446 thalassemic patients co-infected with TTIs, such as HCV, HBV, or HIV, met the inclusion criteria and were analyzed.
Seroprevalence of TTIs amongst multi-transfused thalassemia patients.

Key: *: Not determined, #: Not mentioned, PCR: Polymerase chain reaction, RIBA: Recombinant ImmunoBlot Assay, CLIA: Chemiluminescence Immunoassay, ELISA: Enzyme-linked immunosorbent assay, ELFA: Enzyme-linked fluorescence assay, RIA: Recombinant immunoblot assay, EIA: Enzyme immunoassay, ECLIA: Electrochemiluminescence immunoassays.
Summary of the studies reported the prevalence of TTIs in thalassemic patients.
Discussion
Both HBV and HCV have infected 530 million out of 6 billion worldwide. 18 Pakistan is a developing country with a total population of 190 million, sharing a massive burden of infectious diseases. There is a consistent increase in viral infections in Pakistan. 69 The reported prevalence of HBV and HCV is 4.6% and 4.9%, respectively, in local population of Pakistan 15 ; Pakistan has started an extended HBV vaccination program for children. 15 However, consistent multiple transfusion to β-thalassemia primary patients has increased their life expectancy, which has also amplified the threat to acquire post-transfusion hepatitis. 68
This systemic review aimed to summarise the available literature on TTIs prevalence in thalassemic patients in Asia. The current literature survey showed that HCV was the prominent TTI among multi-transfused thalassemia patients. A lower prevalence of HBV infection than HCV among thalassemic patients is likely due to the effective HBV vaccination. Vaccination against HBV is highly effective (80–100%) in decreasing the HBV infection rate in people who received complete HBV vaccine course. 70 Although HBV prevalence is lower than the prevalence of HCV because of improved immunization status, however, it is still on higher side in comparison to HBV global prevalence in thalassemic patients ranging from 0.3–5.7%. 71 Our data on TTIs infections in thalassemic patients showed a higher prevalence of HCV coinfection than HBV and HIV coinfection in transfusion-dependent thalassemia patients in Asia. The HIV prevalence in blood donors is <0.18%. 72 An alarming trend noticed in this review analysis is that variation in the prevalence of HIV in transfusion dependant thalassemic patients in Pakistan and India has been found to be higher than the overall prevalence of HIV in donor population. There is an urgent need to initiate regular testing for HIV for better risk assessment and actual disease burden in thalassemic population.
In low-resource countries, β-thalassemic patients have limited access to safe and regular blood transfusion, possibly due to inadequate testing of blood donations for STIs and the lack of altruistic voluntary blood donors.
Despite screening of blood donors by quick Immunochromatographic Method, HCV infection is still a crucial source of viral hepatitis infection among multi-transfused thalassemia children. There might be drawbacks in donor screening using this method. 27 NAT testing is undertaken using PCR. It can be conducted in pooled testing and, therefore, cost-effective if carried out in large-scale testing and blood banking facilities. 32 Conferring to the study results, TTIs were markedly high. HCV was identified as the leading viral infection among TTIs in transfusion dependant thalassemic patients and HIV infection prevalence was also noted in few cases which might be another distressing situation in the country. 32 This study highlights the research reports from developing countries, as high-resource countries have recently implemented HCV testing since 1991 and NAT testing. It is cost-effective to test on scale through automated and centralized systems. In low-resource countries, particularly in the Indian subcontinent, the development of government policies, haemovigiliance, and education of blood banking provider is critical to reduce the risk of TTIs in blood transfused thalassemic patients.
This review study has certain limitations as limited countries’ data are analyzed. The extracted data is from the research reports published in the last 20 years, mainly from low-resource Asian countries.
Conclusion
The study concluded that the prevalence of TTIs such as HCV, HVB, and HIV is very high in transfusion-dependent thalassemia patients, emphasizing the high prevalence of HCV alone or in combination with HBV. These TTIs could be caused by a fragmented blood transfusion system, insufficient safety measures, or insufficient resources in transfusion-dependent thalassemia patients. To summarize, we propose that enacting robust policies at the regional and national levels regarding safe blood transfusion practices and donor screening under universally quality-assured procedures may help mitigate future TTI risk.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study reviews published studies and do not require ethical approval.