
Abstract
Oral diseases have been adversely associated with cardiovascular diseases (CVD), which are also the most frequent cause of death in older population. The aim of this study was to investigate the association among oral status indexes and CVD in patients aged more than 65 years attending in the Oral department of a public hospital Policlinico Umberto 1 of Rome. The study population consisted of 533 patients. Dental status was detected measuring the Decayed, Missing, and Filled Teeth (DMFT) and Community Periodontal Index (CPI) indexes. The chi-square test with a 95% confidence level was used to assess qualitative variables. Odds ratios (ORs) and stepwise logistic regression were used to calculate risk estimates; the independent variables: age, gender, DMFT, CPI index, Geriatric Oral Health Assessment Index (GOHAI) score, and tooth loss were included in the statistical model. P value <0.05 was considered a statistically significant cut-off. No differences were found between females and males for DMFT and CPI. GOHAI data were worst for females. Patients with CVD had less education and oral care (P < 0.05), and higher CPI index and number of missing teeth (P < 0.05). Data show that patients with more than 18 missing teeth have 2.5 times greater risk of CVD. CVDs are associated with type 2 diabetes mellitus, underweight, and obesity (P < 0.05). From the findings of this study, it can be confirmed a significant link between CVD and oral health. A cooperation among geriatrician, cardiologist, and dentist is suitable to counteract the development of CVD and to early identify patients at risk of CVD.
Keywords
Introduction
The association between systemic illnesses and diseases of the oral cavity has been studied for many years, mainly because diseases of the oral cavity seem to be a risk factor for cardiovascular events and type 2 diabetes mellitus. 1 Several studies have shown that the prevalence of periodontal disease and attachment loss increased significantly with age; moreover, it has been shown that most patients with periodontal disease were suffering from systemic disease. 2 It is known that the oral health status may interfere in people’s food choices; thus, the diet is usually poor in nourishing terms, affecting the individual’s general health, leading to increased levels of cholesterol, triglycerides, and obesity, and raising the risks of developing cardiovascular diseases (CVD). Researchers postulated a possible link between periodontal and CVD. 3 The concomitant presence of periodontitis may start and/or exacerbate the inflammatory response in atherosclerosis due to a direct and indirect mechanism. Direct mechanism is due to bacteremia caused by tooth brushing and dental procedures 4 of gingival sulcus and pockets. Moreover, viable periodontal pathogens and bacterial DNA have been isolated from human atheromas. 5
Indirect mechanism is attributable to the local production of inflammatory and autoimmune factors from periodontal tissue that circulates in the blood stream and could contribute to damage the vascular endothelium during the immunological cross-reactions between anti-pathogen antibodies and host vascular antigens. This ultimately results both in atherosclerosis and atheromatous plaque rupture. 6 Consequently, it is very important to control the risk factors for diseases of the oral cavity. Studies suggest that the treatment of periodontitis may be associated with positive effects both on inflammatory serum markers and on endothelial function. 7
The oral health problems are assessed measuring teeth loss and teeth decays; Decayed, Missing, and Filled Teeth (DMFT) index is another common index in dental epidemiology to assess the oral health and caries prevalence by a dentist. Periodontal status was assessed by Community Periodontal Index (CPI) that measure severity and degree of disease (gingivitis, task deepness) according to a World Health Organization (WHO) recommendation. 8 Masticatory function, oral self-perception, and psychosocial impact on patients are usually scored by the Geriatric Oral Health Assessment Index (GOHAI), a measurement system designed to assess the oral health problems of older patients. 9
A lower GOHAI score and a higher DMFT index are expected in poor dental health. The objective of this study was to conduct a retrospective analysis to detect oral health status and a possibly association between dental indexes and presence of vascular diseases in elderly patients.
Methods
From January 2015 to February 2016, 533 patients (308 females, 225 males) were asked to visit the Geriatric Dentistry Department of “Policlinico Umberto I” of Rome for a routine check of their oral cavity/dental status. All subjects gave informed, signed consent to participate in the study.
The mean age of patients was 73.93 (±7.8 standard deviation (SD)) ranging 65–98 years.
The staff group collaborating in this study was composed of geriatricians, cardiologists, dentists, and other health professionals. A pre-designed medical history questionnaire including social status, habits, medical history, general health, and drug assumption were filled by each patient. Medical history, particularly focused on vascular diseases (stroke, previous myocardial infarction (MI), ischemic heart diseases, carotid plaque, peripheral artery diseases, etc.), and common atherosclerotic risk factors (arterial hypertension, diabetes, body mass index, etc.) have been recorded.
Patients with active cancer or recent vascular events have been excluded from the study. Each patient was introduced to GOHAI Index consisting of 12 questions that highlight aspects considered to have an impact upon the quality of life of the older population, such as functional limitation, chewing discomfort, esthetic dissatisfaction, and psychosocial problems. A high GOHAI score indicates satisfaction, a good perception of their oral status and a good oral health. Furthermore, a dental screening was performed by two dentists who detected DMFT Index, CPI, and the presence of removable or fixed dentures.
Statistical analysis
A descriptive statistical analysis was performed for the categorical variables with the description of the frequencies (%). For the continuous variables, the measures of central tendency (mean or median) and the variability measures (SD and interquartile range) were calculated.
To assess the presence of the association between categorical variables chi-square statistical test was used; subgroup analyzes by age group, sex, weight class, oral care level, living habits, and sociodemographic characteristics were performed. To assess the possible association between sociodemographic variable levels and the oral cavity problems, a study analysis of GOHAI index response was performed. Moreover, we calculated the risk indicators (OR) as expression of the risk trend of general pathologies developing by the progressive transition to a higher class of missing teeth.
Variables showing significant association at the univariate analysis with CVD were included in a multivariate logistic regression model. The level of significance was set at the value of 0.05, and all analyses were performed with IBM SPSS v.21 software.
Results
The mean of the DMFT was 13.8 (SD: 7.1). Among all patients, 8.6% (n = 46) had more than 12 decayed teeth, 43.7% (n = 233) had more than 12 missing teeth. A total of 122 patients (52.4%) had more than 18 missing teeth. No difference between females and males was seen in DMFT index (13.6 ± 7.3 vs 14.1 ± 7.0, P > 0.05).
The GOHAI index was used to describe the general health status of the studied population. GOHAI sample mean (±SD) was 15.24 ± 8.88. As expected, the GOHAI index significantly decreased with age. Females experienced lower values than men. Data regarding GOHAI status of patient classified as “good,” “mediocre,” and “bad” conditions are reported in Table 1.
Distribution GOHAI items across Likert scale.
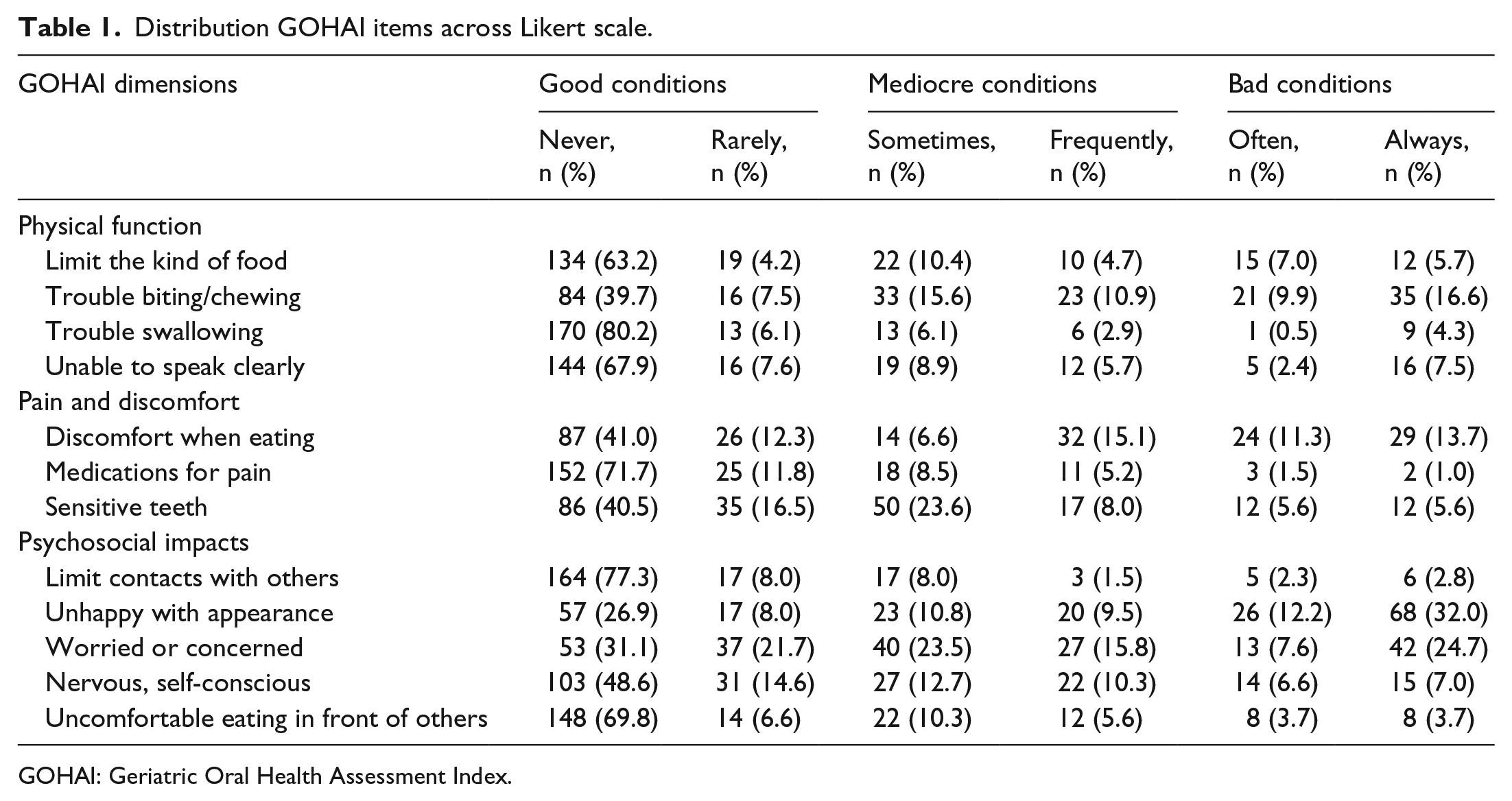
GOHAI: Geriatric Oral Health Assessment Index.
Despite the results shown in Table 1, the quality of life was determined by the included in the study patients as acceptable. The proportion of patients who claimed that they never had trouble swallowing was 80.2%. Discomfort of eating in front of others was never experienced by 69.8% of subjects. Those who have never limited their social relations because of dental status was 77.3%.
Obviously GOHAI score declines with age. Higher GOHAI scores were seen in female patients; they experienced worse perception of the health status of their oral cavity. However, there were no statistically significant differences of GOHAI values related to sociodemographic variables (education, monthly income, and living with) (Table 2).
Univariate analysis for associations between sociodemographic variables and the GOHAI mean score.
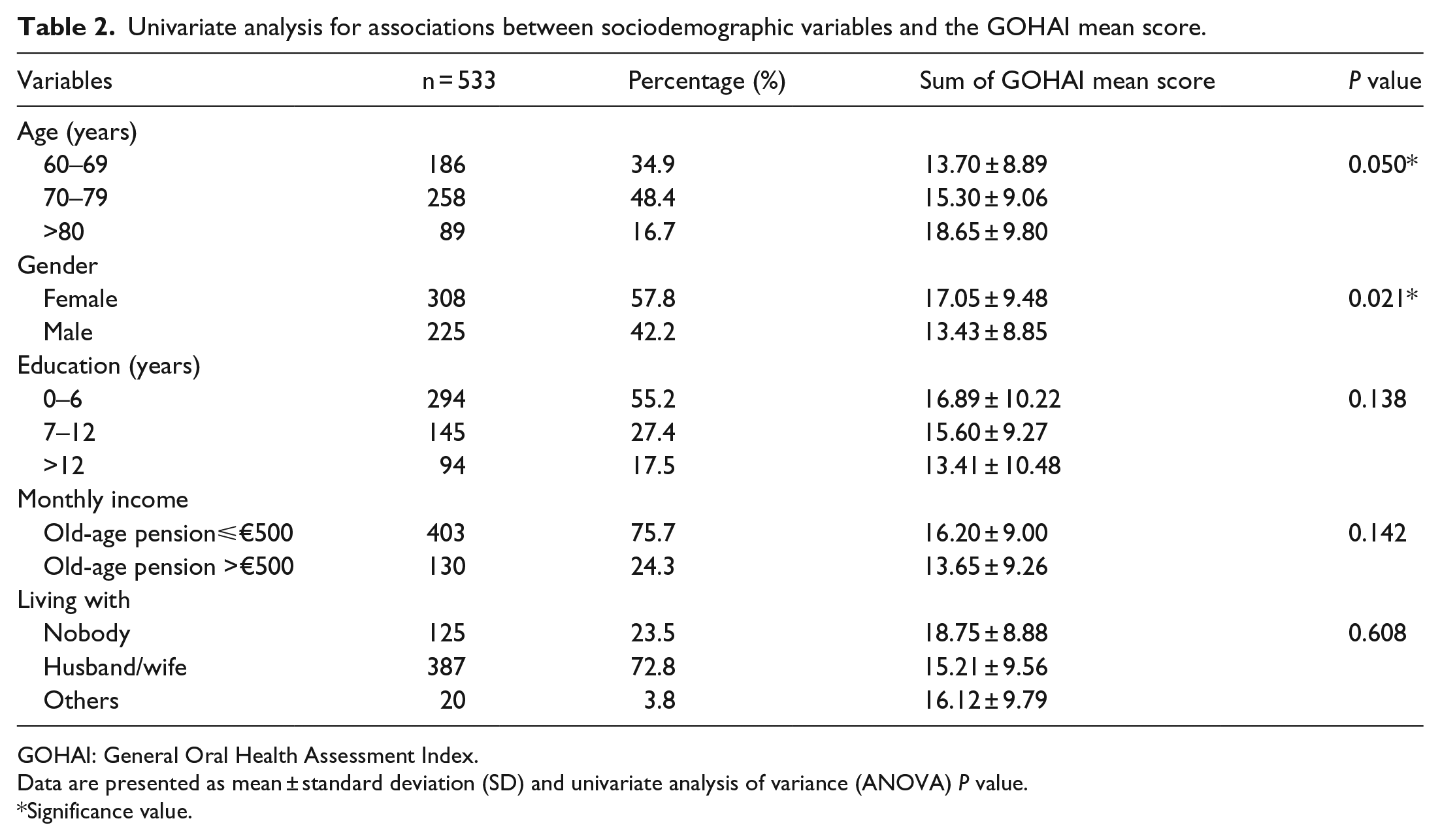
GOHAI: General Oral Health Assessment Index.
Data are presented as mean ± standard deviation (SD) and univariate analysis of variance (ANOVA) P value.
Significance value.
No significant differences in DMFT and CPI indexes between people with different life styles (alcohol/smoking) have been observed.
Vascular diseases affected 69.8% of subjects (n = 372). As shown in Table 3, patients with vascular diseases had mean age, sex, monthly income, chronic obstructive pulmonary disease (COPD), alcohol intake, smoking habit, comorbidity similar to those observed in patients without vascular diseases. Patients with CVD had lower education resulting in shorter education time (P < 0.05) were more frequently affected by type 2 diabetes mellitus (P < 0.05), underweight, and obesity (P < 0.05). The married people were more affected by cardiovascular problems (66.9% vs 52.8%), with a reverse trend for the single persons.
Stepwise logistic regression between the independent variables and the presence of cardiovascular disease.

SD: standard deviation; COPD: chronic obstructive pulmonary disease; CPI: Community Periodontal Index; DMFT: Decayed, Missing, and Filled Teeth.
is the level of significance minor of the set value of 0.05.
Oral care was worse prevalently in patients with vascular disease (P < 0.05). Accordingly, CPI index was significantly higher (P < 0.05), and the number of filled teeth was significantly lower (P < 0.05) in this group of patients. Moreover, the number of missing teeth was higher in patients with vascular diseases (P < 0.05). Old people with more than 18 missing teeth (25.8%) showed an increased risk of CVD (P < 0.05). Table 4 compares the unadjusted proportions of chronic disease group of each missing teeth class with those of patients without any missing tooth (control group), through OR calculation and corresponding confidence intervals (95% confidence interval (CI)). Apart from cardiovascular disease and diabetes mellitus, the presence of increasing step-scale of missing teeth tended to raise the risk to suffer from any selected chronic disease. To note the progressive increasing risk of cardiovascular disease moving from a minor missing teeth class to a superior one. Particularly, the subjects with more than 18 missing teeth had a 2.5 major statistically significant risk to suffer by a cardiovascular disease. The augmented levels of missing teeth, despite non-significant results, mark a positive trend risk even for the others observed pathologies.
Disease calculated risk (OR) by missing teeth classes.

OR: odds ratio; COPD: chronic obstructive pulmonary disease; CI: confidence interval.
No relationship among underweight, obesity, CVD, and number of missing teeth has been observed; nevertheless, in subjects with normal weight, number of missing teeth discriminated patients with (n = 121) or without CVD (n = 66) (12 ± 8 vs 9 ± 8, P < 0.05) suggesting that number of missing teeth affect also the quality of the diet.
Logistic regression confirmed that CPI index (OR = 1.067, 95% CI = 1.025–1.110, P = 0.002), the number of filled teeth (OR = 0.929, CI = 0.884–0.976, P < 0.05), and those of missing teeth (OR = 1.033, CI = 1.007–1.060, P = 0.013) were associated with vascular diseases independently from age (range 65–98), sex, and other comorbidities.
Discussion
Tooth loss as well as poor oral care is a worldwide public health issue.10–12 Our study shows a significant correlation between number of missing teeth and CVD; in fact, old people with more than 18 missing teeth have 2.5 times greater risk of CVD. These data agree with the literature; in fact, Holmlund et al. 11 reported an increased risk of mortality from coronary heart disease in subjects with <10 teeth compared to those with >25 teeth. Oluwagbemigun et al. 12 in a study conducted on 24,313 people found that an increasing number of teeth is inversely related to risk of MI.
The presence of more than 20 natural teeth has a fundamental role in maintaining a satisfactory nutritional status. Missing teeth could lead to altered dietary intake and poor nutritional status, which could contribute to increased risk of developing chronic diseases.
Consequences of tooth loss are multiple and not only of a physical nature. The psychological effects reported by various authors with high frequency are shame, tendency to isolation, decreased self-esteem. In our study, 30% of patients refer discomfort because most of them did not have prosthesis with a consequent esthetic and masticatory worsening. The worst GOHAI observed in women is probably due to their higher esthetic needs which lead them to be more exigent. Considering that 96% of the patients enrolled in this study are missing at least one tooth, we can deduce that the loss of natural teeth is a pervasive phenomenon among Italian subjects over 65.
Our results show that 43.7% subjects have more than 12 missing teeth, and 52.4% have more than 18 missing teeth. Around 40% of patients showed an acceptable oral hygiene.
The limitations of the study were represented by (1) retrospective analysis and (2) lack of correlation between nutritional status and/or alcohol consuming and DMFT, CPI, and GOHAI indexes. In this study, we did not evaluate the obesity type by the waist-to-height ratio (WHR). In addition, we believed that in Italy the older people prefer to declare to be soberer in a non-anonymous questionnaire.
With these limitations, considering the high prevalence of patients with more than 18 missing teeth, our data suggest a need for educational and social measures to improve patients’ attitudes to dental care and to encourage the use of prostheses among the elderly in order to restore a normal chewing to allow a suitable nutrition.
Considering that elderly people account for 20% of the population, that the average life has lengthened and the growing increase in public spending for the elderly, geriatrist cardiologist and dentist should collaborate to improve oral health education in elderly and prevention to counteract development of CVD and other general diseases and to early identify patients at risk of CVD.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.