
Abstract
Angiosarcomas are malignant tumors of endovascular origin, which may be divided into primary and secondary forms. Secondary breast angiosarcomas are an increasing problem, especially in patients treated with breast-conserving surgery followed by radiotherapy.
We report a case of radiation-induced angiosarcoma of the breast in a 77-year-old woman who presented with a suspect lesion in her left breast. Excisional biopsy and subsequent immunohistochemical staining of the specimen was performed. Histological report was diagnostic for low–intermediate grade angiosarcoma. The tumor cells were diffusely positive for CD31 and CD34. We performed surgical resection with mastectomy.
A multidisciplinary approach with bleomycin-based electrochemotherapy, radiation treatment, and chemotherapy with pegylated liposomal doxorubicin has been most useful to control subsequent local relapses. To date, the patient is under close observation and is performing well. No recurrence has been demonstrated after ending of chemotherapy.
Introduction
The angiosarcoma is a malignant mesenchymal tumor composed of neoplastic elements, which arise from endothelial cells. Breast angiosarcomas are extremely rare: their incidence is about 0.05% of all breast cancers.1,2 Primary forms usually occur in young women (mean age, 35 years) as painless and palpable lesions, sometimes associated with skin depigmentation. 3 However, secondary forms are observed in older women (mean age, ⩾60 years) as erythematous plaques or nodules. 4 Angiosarcomas related to chronic lymphedema following mastectomy and axillary lymph node dissection are localized to the upper limb or chest wall (Stewart-Treves syndrome). 5 Radiation-induced angiosarcomas after breast-conserving surgery can involve the skin, breast parenchyma, and chest wall.
These tumors generally require a multidisciplinary approach. Surgery is the main treatment, while local treatments such as electrochemotherapy and radiotherapy should be evaluated in each case. Chemotherapy may have a role both in adjuvant treatment than in a palliative setting.
We describe a case of radiation-induced angiosarcoma after breast-conserving surgery in an elderly patient. The case is interesting both for the clinical history and for the responses obtained with different treatments performed.
Case presentation
In February 2011, a 77-year-old woman referred to our department for a follow-up visit.
She had undergone quadrantectomy of the left breast and axillary dissection in April 2003 for an invasive ductal carcinoma (stage I [pT1N0M0]; ER +15%; PgR +30%; HER2 IHC 1+) followed by radiotherapy on the residual breast (60 Gy in 30 fractions) and adjuvant hormone therapy (tamoxifen, 20 mg/daily for 2 years, and anastrozole, 1 mg/daily for subsequent 3 years).
On clinical examination, we noted a detected and ecchymotic lesion (1.3 cm) near the scar of the previous breast surgery. A chest computed tomography (CT) scan revealed skin thickening and a subcutaneous nodule (2 cm) suggestive of tumor recurrence. 18FDG-PET confirmed tracer uptake in the left breast (SUVmax 2.9). There were no metastases in other organs.
An excisional biopsy was performed. The cut surface showed a well-confined nodule (0.9 cm) with a spongy and hemorrhagic aspect. Histologically, the lesion revealed anastomosing vascular channels with minimal endothelial atypia, separated by pleomorphic spindle cells, which often bounded clefts containing red blood cells. On immunohistochemistry, spindle cells were positive for CD31, CD34, and vimentin, but negative for pan-cytokeratin, with mild and focal reactivity for smooth muscle actin, showing an endothelial differentiation. A mitotic index of 10 mitotis figures per 10 high-power fields and a Ki67 of 90% were reported. The diagnosis of low-grade angiosarcoma of the breast was made.
One year later, the patient showed purplish, papular, and nodular skin lesions with ulcerated areas in her left breast. An ultrasound scan confirmed the presence of marked edema and disorganized breast tissue (5 cm). The patient had undergone left mastectomy and breast reconstruction by the latissimus dorsi myocutaneous flap procedure. The specimen revealed nodules with necrotic and hemorrhagic areas, extending in the subcutaneous tissue both in the superficial layer and in the deeper layer, up to infiltrate underlying striated muscle (Figure 1). Immunohistochemistry results were positive for vimentin, CD31, and CD34, and negative for pan-cytocheratin. The diagnosis was low–intermediate grade angiosarcoma, with capillary and papillary type growth pattern. Tumor cell infiltration was also observed in the fibromuscular stroma of nipple (Figure 2).

A macroscopic photograph of breast angiosarcoma: multiple, well-defined red nodules that appear spongy and hemorrhagic on the cut surface.

(a, b) Hematoxylin and eosin staining (10×). Angiosarcoma, low-grade, capillary type: the neoplasm is composed of small, anastomosing vascular channels, infiltrating the collagenous stroma of the nipple. (c, d) Hematoxylin and eosin staining (10×). Angiosarcoma, intermediate-grade, papillary type: the tumor shows densely cellular areas and prominent papillary formations with hyperchromatic endothelial cells. (e, f) Immunohistochemical staining (10×). A strong, diffuse immunoreactivity for CD34 and CD31, surrounding cellular elements, and vascular spaces. There is a tendency to dissect the adipose tissue at the periphery. (g, h) Immunohistochemical staining (10×). Negativity for pan-cytokeratin (g) and a strong, diffuse immunoreactivity for vimentin (h) in the neoplastic population.
In May 2012, the patient presented painful and dark-red skin lesions both in her right breast and in the left hemithorax. A chest CT scan and 18FDG-PET revealed a nodule (2 cm; SUVmax 9.0) in the right breast, ipsilateral axillary lymphadenopathy (SUVmax 1.4), and an area of tissue thickening (5 × 2 cm; SUVmax 8.0) in the left parasternal region. The patient had undergone right mastectomy. In the same surgical procedure, skin lesions in the left hemithorax were treated by bleomycin-based electrochemotherapy. The specimen revealed purplish, papillary lesions and ulcerated nodules with diagnostic features of low–intermediate grade angiosarcoma. Electrochemotherapy was used to treat nodules ⩽3 cm in diameter. Bleomycin was administered intravenously (15,000 IU/m² in 45 s). Skin lesions were treated in the subsequent 8–20 min by electric pulses at 5 kHz frequency, using an electroporator device and needle electrodes with hexagonal array. Four weeks later, the mastectomy scar had healed up well. All lesions treated by electrochemotherapy were fully responsive. The mild erythema and blackish-brown discoloration corresponded to treated areas.
In July 2012, the patient was submitted to radiotherapy (60 Gy in 30 fractions) for tumor recurrence on chest wall. After 3 months, we repeated the treatment with electrochemotherapy for the multiple, dark-red papular and nodular lesions on the abdomen.
In February 2013, with the appearance of new skin lesions on several sites, the patient agreed to receive chemotherapy with pegylated liposomal doxorubicin (40 mg/m² d1 q4w) for six cycles.
Currently, the patient remains under close observation with no evidence of local or distant recurrence.
Discussion
Secondary breast angiosarcomas (AS) are an increasing problem. 6 Diagnostic criteria for radiation-induced AS include: history of radiotherapy; asymptomatic latency period ⩾5 years; development of tumor within a previously irradiated field; and histological confirmation.7,8
Histologically, these tumors can be divided into three growth patterns, reflecting different grade of differentiation: low, intermediate, and high grade.9,10
The low-grade tumors show a widespread proliferation of anastomosing vascular channels, which extend in breast parenchyma and in adipose tissue without papillary formations. In capillary type tumors, neoplastic vessels are dispersed in dense collagen stroma of perilobular area; these vessels may be misdiagnosed as a simple pseudoangiomatous stromal hyperplasia.
The intermediate-grade tumors have vascular channels intersecting with cellular solid areas, “spindle-cells” foci, and hyperchromatic endothelial cells with focal papillary formations.
The high-grade tumors consist of highly cellular areas with prominent formation of papillae and malignant endothelial cells with well-defined nucleoli and high mitotic index. There are, moreover, large areas of necrosis and “vascular lakes”.
Although morphological features of AS are rather heterogeneous, the prognosis is usually poor. Primary forms show local recurrences and distant metastases. In secondary forms, multiple local recurrences are also frequent. Lymph node involvement and distant metastases are rare at presentation; the contralateral breast is a common site of metastasis.
The treatment of AS usually requires an individualized approach, choosing from time to time between different treatment options and multimodal schedules of therapy, which may include surgery, electrochemotherapy, radiotherapy, and chemotherapy.
Mastectomy is considered the main treatment for these tumors; however, although resection margins are negative, the local recurrence rate is high. 11 Electrochemotherapy may be an effective local treatment for cutaneous and subcutaneous tumors of any histological type. This approach is based on synergistic action of low-permeant chemotherapeutic agent, such as bleomycin, and brief and intense electric pulses, to increase cell membrane permeability.12,13 Radiotherapy and chemotherapy have a controversial role in radiation-induced AS. Use of radiotherapy is limited by factors such as previous delivered dose, toxicity related to re-irradiation, and possible radioresistance of radiation-induced lesions. Recently hyperfractionated radiotherapy produced encouraging results; however, there are no standardized protocols for this option. 14 Chemotherapy may represent a palliative treatment both for inoperable patients and for repeated recurrences. Taxanes and anthracyclines are usually the most used agents.15,16 In a retrospective study of 125 patients, paclitaxel and liposomal doxorubicin produced similar results with an average progression-free interval of 4.2 and 4.0 months, respectively. The addition of ifosfamide to doxorubicin may improve the response rate, but at the cost of highly increased toxicity, mainly in elderly patients. 11
In our practice, we administer the Comprehensive Geriatric Assessment (CGA) to every patient ⩾70 years, in order to decide the best treatment strategy (Figure 3). Therefore, the patient had undergone CGA, integrating information on different aspects such as functional status, co-morbidities, and issues related to age. 17 Considering the functional autonomy and the absence of relevant co-morbidities, she was eligible for surgical treatment.
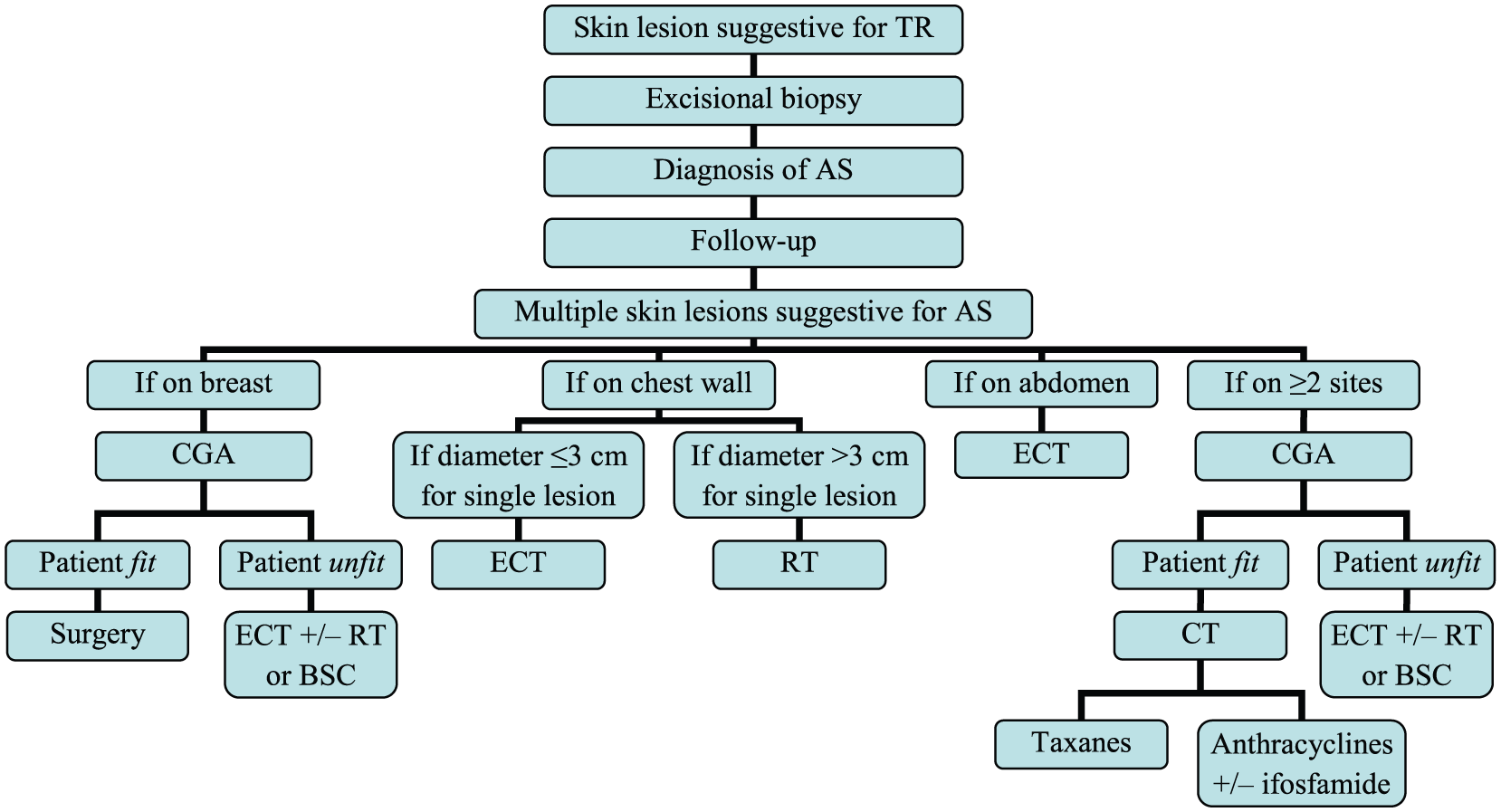
Flow chart of decision-making process. AS, angiosarcoma; BSC, best supportive care; CGA, Comprehensive Geriatric Assessment; CT, chemotherapy; ECT, electrochemotherapy; RT, radiotherapy; TR, tumor recurrence.
For breast reconstruction we used the latissimus dorsi myocutaneous (LDM) flap. This procedure, although in recent years is used less than the transverse rectus abdominis myocutaneous (TRAM) flap, may be considered an acceptable and reliable option especially in older patients, because it is associated with fewer postoperative complications. 18
Electrochemotherapy was performed to treat small skin lesions on the chest wall and abdomen, in order to avoid repeated surgical excisions, while the use of radiotherapy was reserved for treatment of larger and superficial lesions, obtaining a good locoregional control of the disease.
Regarding chemotherapy, we chose a single-agent regimen with pegylated liposomal doxorubicin. The dose was decreased by 20% of the standard regimen to further reduce the risk of toxicity. Pegylated liposomal doxorubicin was preferred to taxanes for good tolerability and greater compliance of our patient with a drug administered every 4 weeks. In fact, the treatment was well tolerated and the patient completed all six planned cycles without adverse effects (Table 1).
Summary of therapeutic options performed.

In our experience, a multidisciplinary approach with surgery, chemotherapy, and locoregional treatments, such as radiotherapy and electrochemotherapy, induced significant objective responses in our patient, prolonging survival and allowing her, at the present time, a better quality of life.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.