
Abstract
Horner’s syndrome (HS) is caused by an interruption of the cervical sympathetic pathway to the eye and the face. Acquired HS is mainly caused by benign or malignant neoplasms, and in patients with a history of cancer, it is almost always the result of tumor infiltration into the periphery or the central region of the cervical sympathetic chain.
We present the case of a 52-year-old patient with long-term disease-free survival (6 years) after a radical mastectomy for breast cancer who presented with cervicobrachialgia and typical HS due to a left lateral-cervical and supraclavicular lymph nodal mass. Treatment of the metastatic disease with taxanes and concurrent trastuzumab resulted in a complete pain resolution, as well as long-term clinical and radiologic remission; however, the neurological cohort of HS remained as the expression of permanent damage to the sympathetic pathway.
This report presents a highly rare case of HS as the first and solitary appearance of metastatic disease in a breast cancer patient. This neurologic involvement should always raise suspicion of metastatic infiltration, and the early recognition of the syndrome may prevent permanent nerve injury.
Introduction
Breast cancer is the leading neoplasia in the female sex and the second most common cause of cancer-related death in women. 1 Breast cancer has a tendency to spread to the lungs, bones, liver, adrenal glands, and skin; remarkably, one-third of breast cancers have metastasized to the lymph nodes at presentation. The thorax is a common site of metastasis, with involvement of the lymph nodes, bones, lungs, pleura, or heart and pericardium. 2
Horner’s syndrome (HS), also called oculosympathetic paresis, is a rare but significant clinical entity resulting from the disruption of the sympathetic neuronal pathway from the hypothalamus to the eyes and face. 3 There is a characteristic triad of partial ptosis (upper eyelid drooping), miosis (pupillary constriction), and hemi-facial anhidrosis (absence of sweating). Sometimes, there can be an apparent mild enophthalmos due to eyelid sagging. HS can be caused by many benign and malignant conditions: neoplasia is the most common cause, accounting for 35–60% of all cases.4,5
We report a single case of HS due to metastases to the lateral-cervical and supraclavicular lymph nodes as the first sign of the spread of breast cancer; very few cases have been described in the literature.
Case presentation
In April 2013, a 52-year-old Caucasian woman presented at the Emergency Unit of the Cardarelli Hospital in Naples, Italy, complaining of 3 weeks of left cervicobrachialgia.
Her past medical history included operable breast cancer 6 years earlier. In fact, in October 2006, the patient underwent left modified radical mastectomy with axillary lymph node dissection for a pT3 pN3 invasive tumor of the left breast. The subsequent histopathology revealed an infiltrating ductal carcinoma with a maximum diameter of 7 cm and aggressive biological behavior: Grade 3, ki-67 = 35%, ER and PgR <5%, and HER2-overexpression, associated with multiple foci of carcinoma in situ and lymph vascular invasion. Moreover, metastases in 16 of 18 dissected lymph nodes at axillary levels I–III were found.
Because of the high recurrence risk, the patient received adjuvant chemotherapy consisting of six courses of the TEC regimen (docetaxel [75 mg/sqm], epirubicin [75 mg/sqm] and cyclophosphamide [500 mg/sqm]), followed by radiotherapy of the thoracic wall; nevertheless, she refused subsequent adjuvant treatment with trastuzumab. She remained disease-free during follow-up of more than 5 years, without cancer and/or treatment-related symptoms.
On admission to our hospital, she complained a left cervicobrachialgia. On clinical examination, a left lateral cervical and supraclavicular mass was evident, with typical HS including constriction of the pupil (miosis), drooping of the eyelid (ptosis), hemi-facial anhidrosis, and mild enophthalmos. Biochemical tests revealed elevated levels of CA15.3 (52.5 U/mL), while serum levels of CEA, CA19.9, and CA125 were within the normal limits. Magnetic resonance imaging (MRI) of the brain, performed to exclude central nervous system (CNS) damage, was negative, while a whole-body computer tomography (CT) scan demonstrated a left lateral cervical and supraclavicular lymph node mass, which measured approximately 60×50 mm and incorporated the main neck vessels (Figure 1). Multiple peri-aortic lymph nodes (maximum diameter of 30 mm) were also described.

April 2013: CT scan at the diagnosis showing a left laterocervical and supraclavicular lymph node mass.
An incisional biopsy of the large mass was performed, and a morphological examination showed grade 3 carcinoma. On immunohistochemical testing, the cancer cells were positive for CK7, weakly positive for estrogen (ER) and progesterone receptor (PR) (1–2%), focally positive for mammaglobin and gross cystic disease fluid protein-15 (GCDFP-15), negative for TTF-1, and strongly positive for HER-2 (score 3+), confirming metastasis from primary breast cancer. Although the staging workup, including the bone scan, was negative for distant metastases, within a few days, the patient started to complain of lancinating pain in the elbow, as well a pain and dysesthesia in the ulnar aspect of the left hand. These symptoms required medical therapy and were successfully treated with tapentadol at a dose of 200 mg/day.
First-line treatment with a standard regimen of chemotherapy (docetaxel 100 mg/sqm) and concurrent immunotherapy (6 mg/kg/BW trastuzumab) every 3 weeks was planned. The patient experienced rapid clinical benefit from the treatment, and the cervicobrachialgia resolved after two courses; therefore, she did not require additional tapentadol. In contrast, the neurological set of symptoms, including miosis, partial ptosis, hemi-facial anhidrosis, and a mild enophthalmos, did not benefit from the treatment.
A CT scan that was performed after 3 courses of first-line chemotherapy showed a significant reduction of the tumor lesion in the context of the left supraclavicular fossa (37×32 vs. 60×50 mm), while the peri-aortic lymph nodes were completely regressed. A reduction in the CA15.3 level was also observed (28 vs. 52.5 U/mL). Therefore, the treatment was continued, with no grade III/IV toxicities, until nine courses were completed, and the final CT scan revealed complete remission of the lymph node involvement (Figure 2).

September 2013: CT scan showing a complete remission after treatment.
At the time of writing, our patient is undergoing maintenance treatment with trastuzumab and anastrozole without pain, and the characteristic triad of HS is still present.
Discussion
We present a rare case of a metastatic breast cancer causing Horner’s syndrome as the first sign of late tumor dissemination.
HS can be caused by infiltration to paravertebral sympathetic nerves and/or pressure on the sympathetic plexus. The neurologic symptoms concern the affected side, and they consist of the inability to fully open the eye (ptosis), pupillary constriction (miosis), loss of hemi-facial sweating (anhidrosis), and enophthalmos. 5
HS results from any lesion that interrupts the sympathetic 3-neuron arc pathway from the hypothalamus to the eye, following a long route that includes central, preganglionic, and postganglionic neurons. First-order neurons originate from the posterolateral hypothalamus, descend into the brainstem and intermedium lateral column of spinal cord, and exit at the cervical (C8) and thoracic (T1–T2) levels of the spinal cord as second-order neurons. Then, the preganglionic segment (second neuron) incorporates into the sympathetic trunk, which crosses the brachial plexus over the apex of the lung and ascends to the synapses of the superior cervical ganglia. Third-order (postganglionic) neurons pass alongside the internal carotid artery, entering into the cavernous sinus to the orbit and the eye, where they enervate the dilator muscle of the pupil, Mueller’s muscles of the eyelids, and the lacrimal sac. The third-order fibers involved in facial sweating usually run with the external carotid artery; thus, third-order lesions do not often result in anhidrosis.
The etiologies of acquired HS are summarized in Table 1. The most common cause of acquired HS is neoplasia, which is malignant far more often than benign, accounting for 35–60% of all cases and determining neuronal pathway lesions. The conditions producing preganglionic HS are mainly malignant tumors.5,6 In a case series of 450 patients with HS, 7 270 (60%) patients had an identifiable cause: 34 (13%) of these patients had first-order neuronal (central) lesions, 120 (44%) had second-order (preganglionic) lesions, and 116 (43%) had third-order (post-ganglionic) lesions. HS is very rare as an initial sign of metastatic dissemination in breast cancer, and only a few cases have been described in the literature.8,9
Causes of Horner’s syndrome.
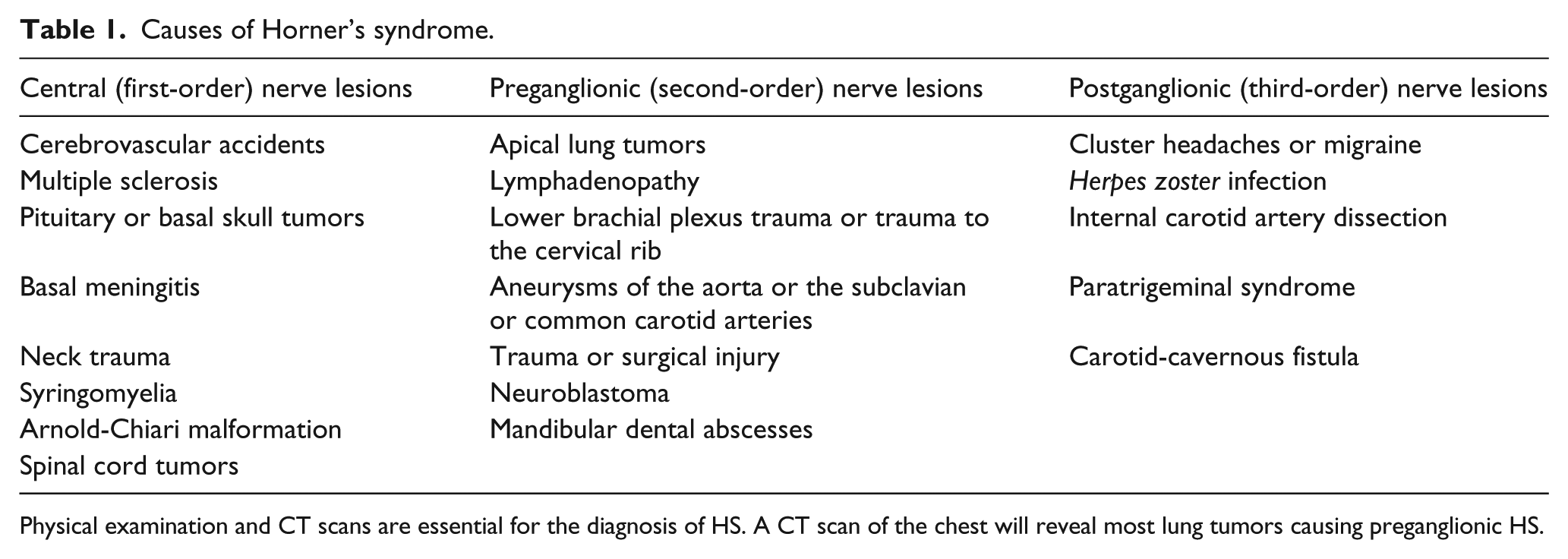
Physical examination and CT scans are essential for the diagnosis of HS. A CT scan of the chest will reveal most lung tumors causing preganglionic HS.
In breast cancer patients, neurologic complications of the upper part of the thoracic region can occur due to surgery, radiotherapy, or metastatic disease.10,11 Brachial plexopathy is a well-known complication of radiation. Involvement of the lower trunk of the plexus is usually caused by the direct extension of the tumor, while involvement of the upper trunk is usually caused by radiation. Taxanes frequently produce peripheral neuropathies; metastatic disease can cause neurologic complications in breast cancer patients, although these complications rarely include HS.
In our patient, lymph node involvement was a late manifestation of first metastatic spread, occurring 6 years after diagnosis, and was the solitary metastatic site as confirmed by an extensive staging workup. On hospital admission, the patient complained of cervicobrachialgia, which had increased over a few days, but it was not possible to establish how long the HS triad had been present.
In this case, HS was a direct consequence of the involvement of the thoracic sympathetic trunk by a disruptive lesion of the second order neurons, together with lower brachial plexus compression. Indeed, the preganglionic segment (second neuron) crosses the brachial plexus over the apex of the lung and ascends to synapses in the superior cervical ganglia.
The patient experienced a rapid, but partial, clinical benefit from chemotherapy: the cervicobrachialgia was resolved after two courses so that she did not require more analgesic, while the neurological set of HS symptoms, in contrast, did not benefit from treatment and remain present many months later. This different clinical outcome of the neurologic involvement was probably due to a different mechanism of neurologic damage. Neuropathic pain was caused by compression of the somatosensory system of the brachial plexus; therefore, tumor shrinkage induced by the treatment resolved the compression and the symptoms as well. Conversely, HS could be the result of a disruptive and permanent lesion of the second order sympathetic neurons; therefore, the neurological set of HS symptoms could be persistent, although the patient remains free of disease more than 1 year after the clinical onset.
In summary, the clinical history of our patient and the biopsy of the lesion were essential for diagnosis (late and isolated recurrence) and for analytic purposes (i.e. biomarker assessment). It was highly unusual to see HS ocular involvement as the first sign of systemic metastasis from primary breast cancer; however, this neurologic involvement should always be investigated for metastatic infiltration. The recognition of the presence of the syndrome allows for early and appropriate diagnosis, can prevent permanent nerve damage, and is essential for choosing the correct treatment.
Footnotes
Acknowledgements
We wish to thank Roberta Bonetti and Stefania Coppola, nurses in the Breast Unit Cardarelli, for their support of and contributions to the acquisition of the data.
Consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy is available for review by the editor of this journal.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.