
Abstract
The failure of traditional antimicrobial treatments is becoming a worldwide problem. The use of Aloe vera is of particular interest for its role as curative agent and its efficacy in complementary therapies for a variety of illnesses. This study evaluated the antimicrobial activity of A. vera inner gel against a panel of microorganisms, Gram-positive and -negative bacteria, and Candida albicans. In addition to A. vera inner gel being used in the treatment of peptic ulcers, in dermatological treatments, and wound healing, it was also tested on the sessile phase of clinical Helicobacter pylori strains (including multi-drug-resistant strains) and on planktonic and sessile phase of Staphylococcus aureus/Pseudomonas aeruginosa clinical isolates from venous leg ulcers.
A. vera inner gel expresses its prevalent activity against Gram-negative bacteria and C. albicans in respect to Gram-positive bacteria. The results of the A. vera antibiofilm activity showed a decrease of the produced biomass in a concentration-dependent-way, in each analyzed microorganism. The data obtained show that A. vera inner gel has both an antimicrobial and antibiofilm activity suggesting its potential use for the treatment of microbial infections, in particular for H. pylori gastric infection, especially in case of multi-drug-resistance, as well as for an effective wound dressing.
Introduction
Over the years the success of traditional antimicrobial treatments against infections due to bacteria and yeasts has been strongly affected by the increase of resistant strains. This emergence is often caused by overuse or misuse of common antibiotics, but it is also widely documented that the ability of species to form biofilm plays an important role. 1 In fact, tolerance of biofilms to antimicrobials killing is of 100–1000-fold above the minimal lethal dose, and occurs for a wide number of antimicrobials and microbial species. 2 As multi-drug-resistance has become worldwide problem, new antibacterial and antibiofilm strategies are demanded and necessary.
In the last decade, the use of medicinal plant species in the management and treatment of Gram-positive and -negative bacteria and Candida albicans infections represented a new frontier of research in the phytopharmacological field. 3 In particular, among these medicinal plants, Aloe vera or A. barbadensis is of particular interest to its historic reputation as a curative agent and its widespread use in complementary therapies for a variety of illnesses. 4 To date, a large number of biological activities have been ascribed to A. vera leaf extracts such as antimicrobial, anti-inflammatory, lipid and glucose lowering, antiproliferative, immunostimulatory, and antioxidant functions. 5 The active compounds of A. vera include anthraquinones, as aloin, aloe-emodin, acemannan, flavonoids, saponin, sterols, amino acids, and vitamins. 6 In particular, it is notable that the anthraquinones, present in A. vera inner gel, have direct antibacterial activities. 7
In the first part of this study, the antimicrobial activity of A. vera inner gel was determined against a panel of microorganisms including Gram-positive and -negative bacteria and C. albicans. In addition to A. vera inner gel being used in the treatments of both peptic ulcer 8 and wound healing, 9 it was also tested on sessile phase of clinical Helicobacter pylori strains (including multi-drug-resistant strains), previously tested on their planktonic phase 10 and on planktonic and sessile phase of Staphylococcus aureus/Pseudomonas aeruginosa clinical isolates. Staphylococcus spp. and Pseudomonas spp. represent the predominant bacterial species associated to the infection processes of chronic wounds, and their biofilm forming capability increases the tolerance against antimicrobials. 11 Finally, it is well known that the failure of the anti-H. pylori therapeutic regimens is due to both the H. pylori multi-resistance and to its capability to form biofilm.10,12
Materials and methods
Extraction of Aloe vera inner gel
The plant of A. vera var, barbadensis Miller was retrieved at a local farmer plant in Manoppello, Abruzzo, Italy and came from the Farm Francesco Amati (Contrada Ciurbo, 6, 72017 Ostuni, Italy), which manufactures and sells plants of A. vera and arborescens. The plant was grown without chemical fertilizers on a fundus of about 1 acre of land in the city of Ostuni (40°44’00” South and 17°35’00” West) away from sources of pollution. A mature and fresh leaf of A. vera, of a 5-year-old plant, approximately 70–80 cm long was washed with fresh water, its thick epidermides was removed and the inner gel was cut into pieces.
The solid mucilaginous and transparent gel was collected in a dark sterile container for light protection and homogenized with an Ultra-Turrax (T10 basic ULTRA-TURRAX, IKA-Lab, Milan, Italy) in 2% dimethyl sulphoxide. Then, the solution was treated for a short time (1–2 min) at 85–90°C, filtered with 0.80 µm filter (Millipore, SpA, Rome, Italy) and used immediately after for antimicrobial assay. No chemicals were added and the original composition was maintained. The chemical fingerprint of the A. vera inner gel used for this study was investigated in our previous work. 10
Bacterial strains and culture conditions
The microorganisms listed in Table 1 were used for the experiments. S. aureus PECHA 10 and P. aeruginosa PECHA 9 clinical strains were chosen as typical biofilm producers and as strains responsible for chronic wounds.1,13 These strains were isolated from the wound of a patient with venous leg ulcer. 1
In vitro antimicrobial activity of Aloe vera inner gel against Gram-positive and -negative bacteria and Candida albicans.
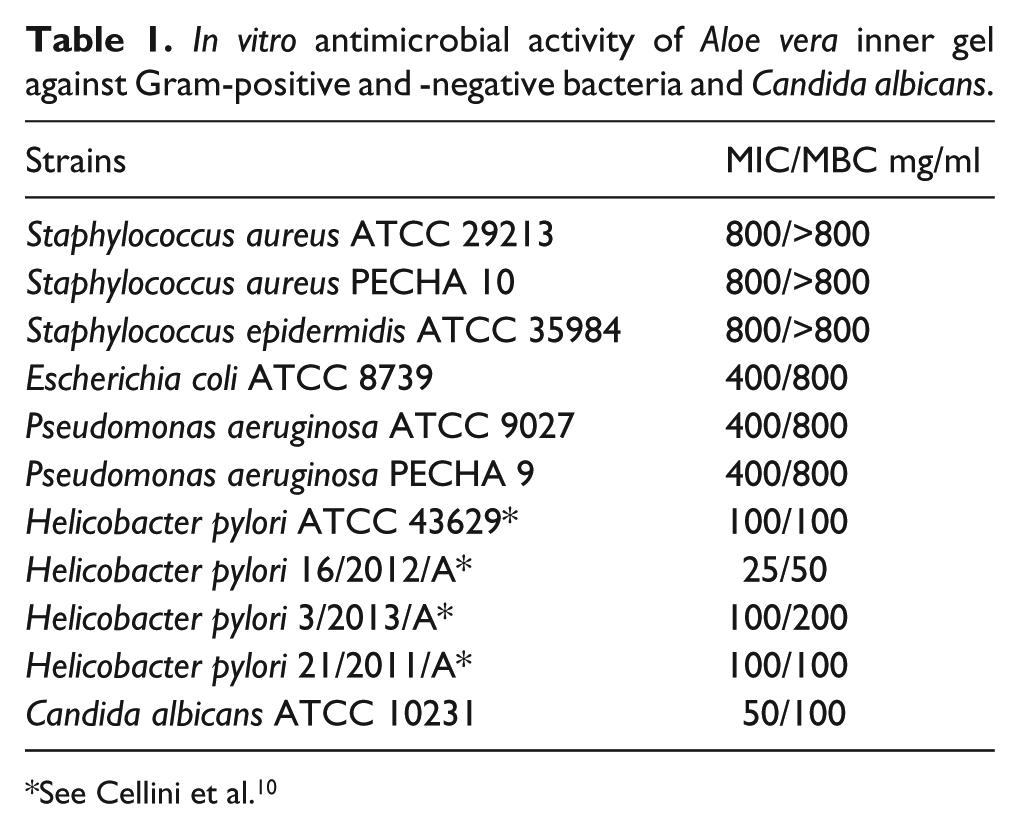
See Cellini et al. 10
The H. pylori clinical strains were chosen among a panel of H. pylori strains previously studied for their susceptibility against both A. vera inner gel and antibiotics commonly used in therapy. 10 The selected H. pylori strains for this study were the most susceptible to A. vera inner gel and expressed a different profile against the antibiotics tested. In particular, H. pylori 3/2013/A and H. pylori 21/2011/A were multi-resistant strains whereas H. pylori ATCC 43629 (ATCC LGC Standards S.r.l., Sesto San Giovanni, Milan, Italy) and H. pylori 16/2012/A were susceptible strains.
From strains stored at −20°C, pure cultures were prepared as follows: S. aureus ATCC 29213 (ATCC LGC Standards), S. aureus PECHA 10, and S. epidermidis ATCC 35984 (ATCC LGC Standards) were spread on Mannitol Salt agar (Oxoid, Milan, Italy); E. coli ATCC 8739 (ATCC LGC Standards) was spread on McConkey agar (Oxoid); P. aeruginosa ATCC 9027 (ATCC LGC Standards) and P. aeruginosa PECHA 9 were spread on Cetrimide agar (Oxoid). Then, colonies from each culture were grown at 37°C in Tryptic Soy Broth (TSB, Oxoid) overnight and subsequently diluted 1:5 in Muller-Hinton Broth (Oxoid) and incubated aerobically for 2 h at 37°C under shaking (100 rpm), to obtain the exponential bacterial growth. These cultures were then adjusted to an optical density at 600 nm (OD600) of 0.1 corresponding to approximately 108 cfu/ml, using Biophotometer (Eppendorf, Milan, Italy) and a final dilution of 1:100 was performed for the experiments.
The reference and the clinical H. pylori strains, stored at −80°C for long-term maintenance, were cultured on non-selective medium (chocolate agar [CA]) containing Columbia agar base (Oxoid) with 10% (v/v) laked horse blood plus IsoVitalex 1% (v/v) (BBL, Microbiology System, Milan, Italy) and incubated in a microaerobic environment at 37°C for 5–7 days (GasPak, Oxoid). The bacterial suspensions, containing all colonies grown on CA medium, were prepared in Brucella Broth (BB) (Biolife Italiana, Milan, Italy), adjusted to an optical density at 600 nm (OD600) of 0.2 corresponding to approximately 1.8 × 107 cfu/ml, using Biophotometer and used for the experiments.
Finally, C. albicans ATCC 10231 was grown at 37°C in RPMI (Oxoid) overnight and then was diluted 1:5 in RPMI medium with 2% glucose (Oxoid) and incubated aerobically for 2 h at 37°C under shaking. The culture was adjusted to an optical density at 600 nm (OD600) of 0.15 corresponding to approximately 5 × 107 cfu/ml using Biophotometer and a final dilution of 1:10 was performed for the experiments.
Determination of Aloe vera inner gel minimum inhibitory concentration (MIC) and minimum bactericidal concentration (MBC)
The antibacterial activity of A. vera inner gel against all studied microorganisms was assayed by broth microdilution method according to CLSI guidelines (2012). 14 Two-fold dilutions of the substance were performed to obtain the final concentrations from 800 to 1.56 mg/ml. The microdilution method was carried out in 96-well microtitre plates (Nunc, EuroClone SpA, Life-Sciences-Division, Milan, Italy). In each well were dispensed aliquots (100 µl) of A. vera inner gel and bacterial suspension at the concentrations described above. Two hundred microliters of A. vera inner gel, bacterial suspensions, and specific media were also included as controls. All microtiter plates of Gram-negative and -positive bacteria and C. albicans were incubated aerobically for 24 h at 37°C. Microtiter plates of H. pylori were incubated in microaerobic condition for 3 days at 37°C.
MIC values were measured by determining the lowest concentration of A. vera extract needed to inhibit the visible growth of the microorganisms. After determination of MIC for each strain, the minimal bacterial concentrations (MBCs) were determined by subculturing from the non-turbid wells into specific media. The MBC was determined as the lowest concentration of A. vera inner gel that gave complete inhibition of colony formation on plates.
Two experiments in duplicate were performed.
Biofilm growth condition
The activity of A. vera inner gel was evaluated on the microbial biofilm formation capability, at sub-MIC levels, against S. aureus and P. aeruginosa clinical isolates and their mixture and against four H. pylori strains.
S. aureus PECHA 10 and P. aeruginosa PECHA 9 clinical isolates were separately harvested in TSB and incubated overnight aerobically at 37°C. In order to obtain log-phase broth cultures, the overnight cultures were diluted 1:5 in fresh TSBG (TSB supplemented with 0.5% w/v glucose) and incubated aerobically for 2 h at 37°C under shaking (100 rpm); these cultures were then adjusted to an optical density at 600 nm (OD600) of 0.1 corresponding to approximately 108 cfu/ml; a final dilution of 1:100 in TSBG was performed for each strain. Such standardized broth cultures were used to prepare a mixture 1:1 (v/v) of the two strains.
Helicobacter pylori ATCC 43629, 3/2013/A, 16/2012/A, and 21/2011/A were harvested in BB supplemented with 2% (w/v) fetal calf serum (Biolife, Italy) and 0.3% (w/v) glucose. Broth cultures, gently shaken, were then incubated overnight at 37°C in a microaerobic atmosphere. After incubation, each broth culture was adjusted to an optical density at 600 nm (OD600) of approximately 0.1. 15
The above prepared cultures (100 μl) were inoculated on flat-bottomed 96-well polystyrene microtiter plates with A. vera inner gel (100 μl) at sub-MIC concentrations ranged from half to one-32nd of the MIC value. The treated biofilms and the respective controls were analyzed for the biomass production through the crystal-violet staining method. 1 Planktonic cells were removed and biofilms were rinsed with 100 μl of H2O sterile, fixed by air drying and stained with 100 μl of crystal-violet 0.1% (w/v) for 2 min. The stained biofilms were rinsed with 100 μl of H2O sterile, air dried, and eluted with 100 μl of acetic acid 33%. The optical density was measured at 595 nm using a microplate reader (SAFAS, Munich, Germany). The results were expressed as average of OD595 values of two replicates in two different experiments.
Statistical analysis
The differences among the biofilm biomass formed at different concentrations of A. vera inner gel were performed using one-way analysis of variance (ANOVA). Probability levels of <0.05 were considered statically significant. Moreover, the method of linear regression analyses were used to establish a correlation between biofilm formation and the sub-MIC level of A. vera. Regression plots were constructed using Microsoft Excel.
Results
The antimicrobial activity of the A. vera inner gel against microorganisms used for this study, was reported in Table 1. Its prevalent activity was expressed against Gram-negative bacteria and C. albicans in respect to the Gram-positive bacteria. In particular, H. pylori strains were inhibited at concentrations never major of 100 mg/ml; E. coli ATCC 8739 and the reference and clinical P. aeruginosa strains were inhibited at 400 mg/ml, whereas C. albicans displayed a MIC value of 50 mg/ml. Of interest, the MBC values were equal to MIC values, except for few cases in which only one step above was recorded to obtain the bacterial death.
The results from the antibiofilm activity of A. vera inner gel against the sessile bacterial population detected in this study, were shown in Figure 1.
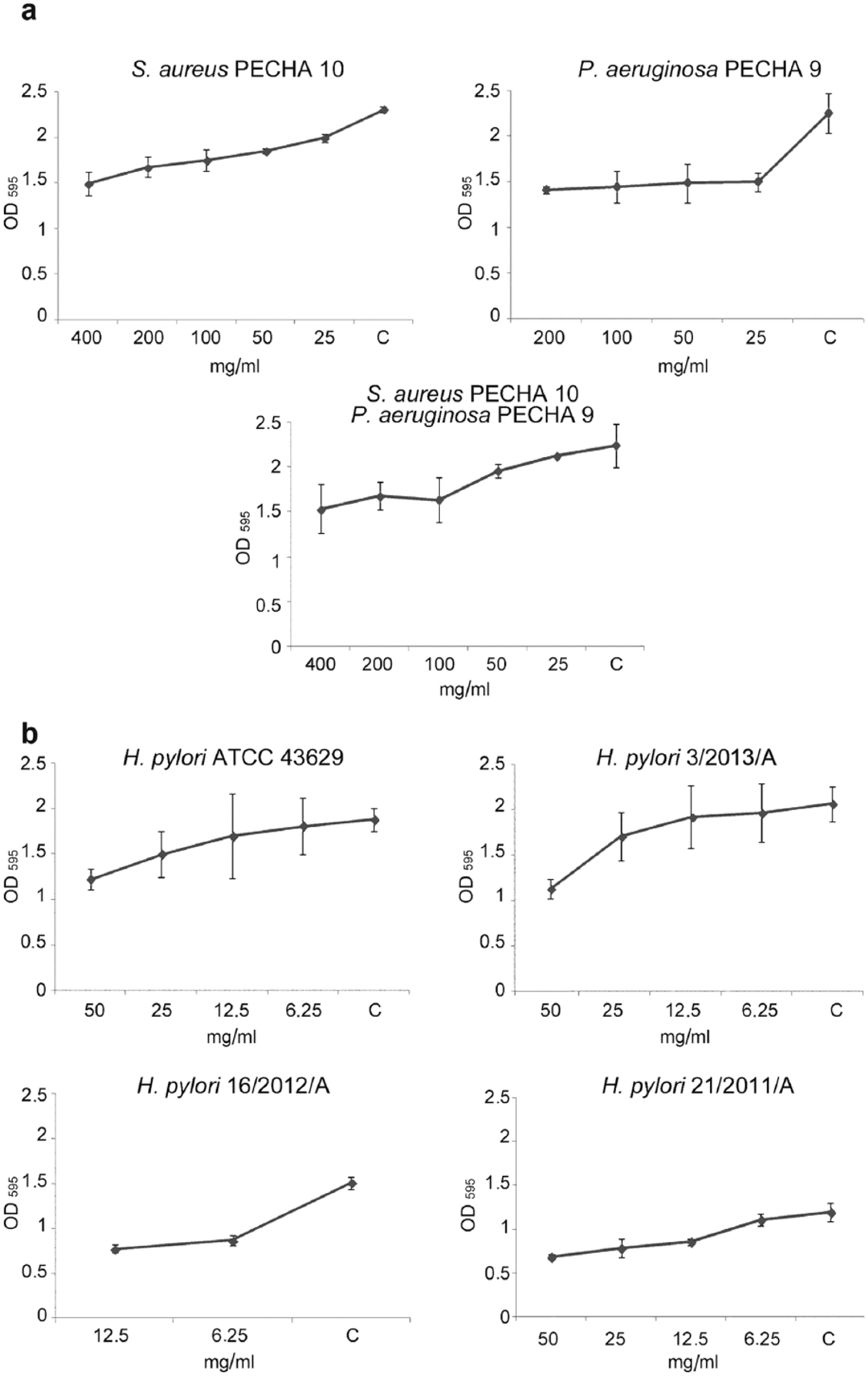
Effect of Aloe vera inner gel on biofilm formation of (a) S. aureus PECHA 10, P. aeruginosa PECHA 9, and their mixture biofilms; (b) H. pylori ATCC 43629, 3/2013/A, 16/2012/A, 21/2011/A. The formed biofilms were analyzed for the biomass production through the crystal-violet staining method. The results were expressed as average of OD595 values of two experiments in duplicate (mean value ± SD; C = control). Probability levels of <0.05 were considered statically significant.
For each analyzed microorganism, a reduction in biomass production was observed in presence of sub-MIC concentration of A. vera inner gel. In general, the sessile population decreased in an A. vera inner gel concentration-dependent-way, except for P. aeruginosa PECHA 9, in which an evident decrease in OD595 detection was already observed in the presence of 25 mg/ml of extract and this effect was not modified in the other tested concentrations.
In the case of H. pylori 3/2013/A, all obtained values compared to each other, using ANOVA, were statistically significant (P = 0.03).
A significant positive correlation between biofilm formation and sub-MIC concentration used resulted in all microorganisms tested (Figure 2), except in the case of the mixture of S. aureus PECHA 10/P. aeruginosa PECHA 9 and H. pylori 21/2011/A, where no significant correlation was observed (P = 0.1 and P = 0.14, respectively; Table 2).
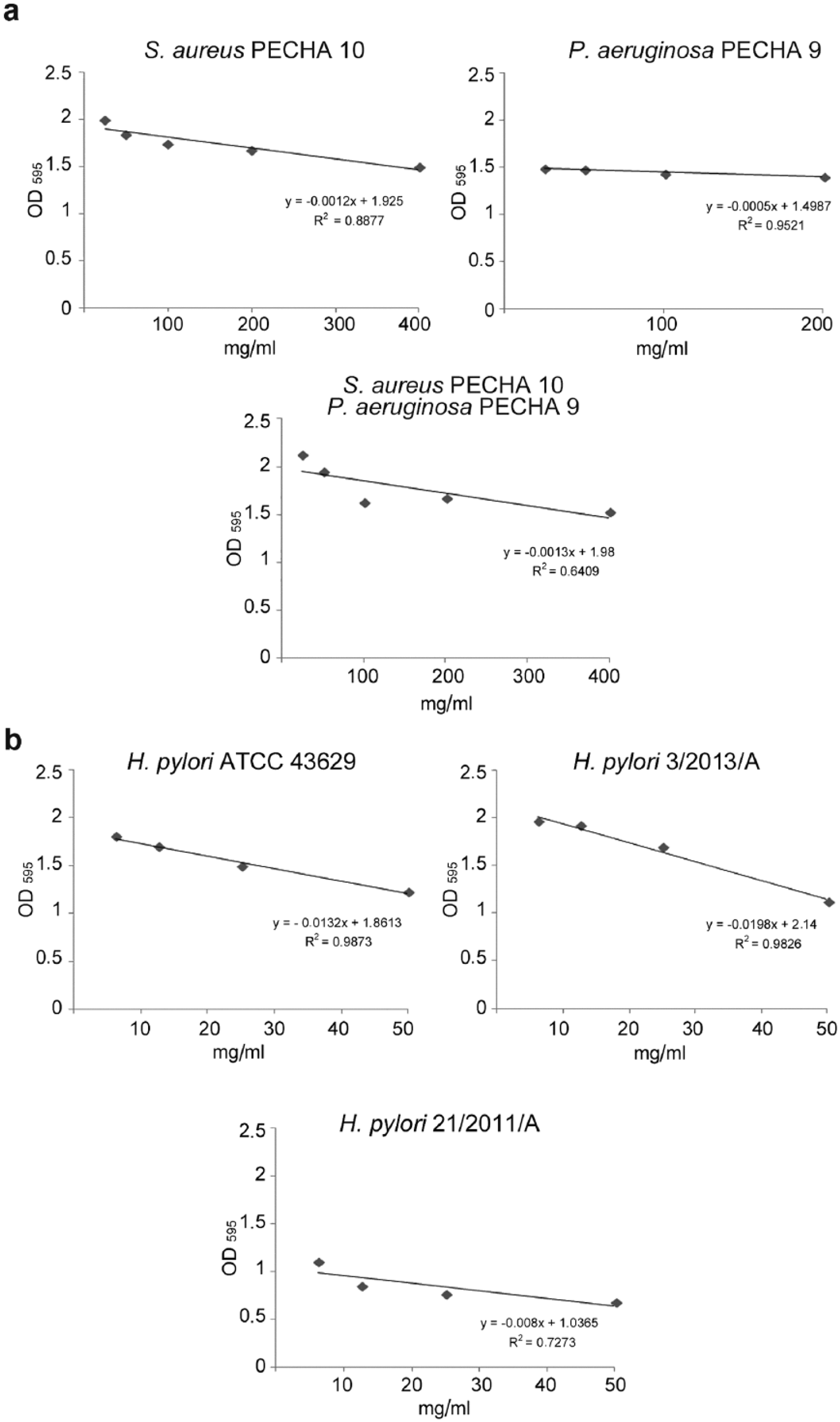
Correlation between biofilm formation and the sub-MIC level of Aloe vera, obtained from method of linear regression analysis, of (a) S. aureus PECHA 10, P. aeruginosa PECHA 9, and their mixture biofilms; (b) H. pylori ATCC 43629, 3/2013/A, 21/2011/A.
Estimation of linear regression parameters.
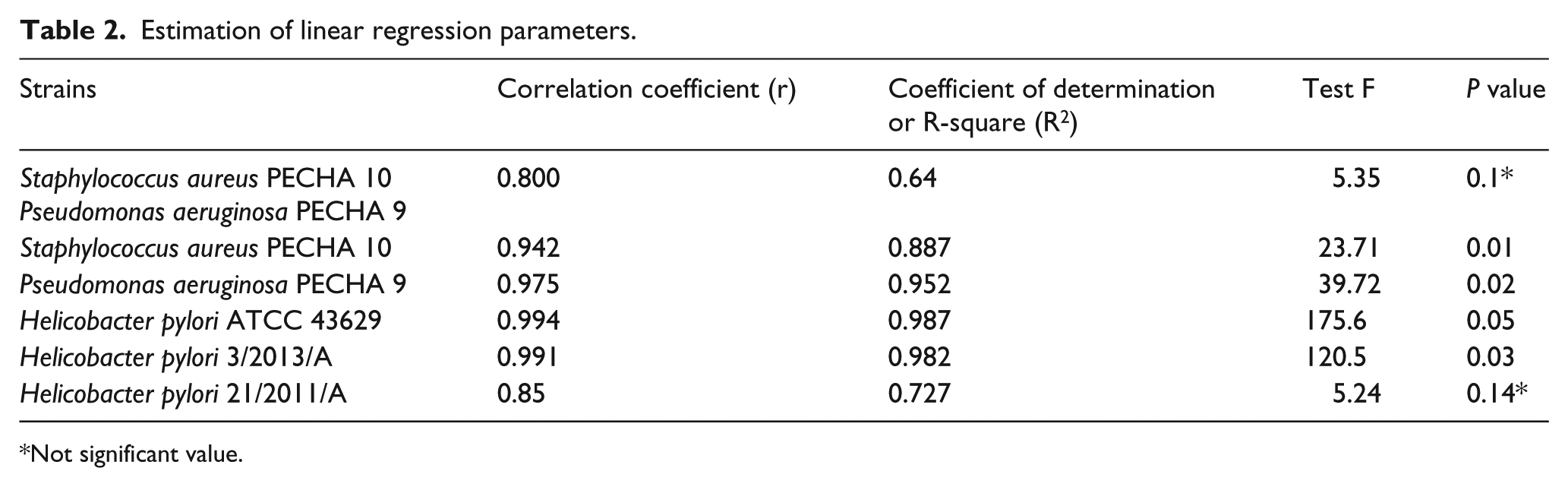
Not significant value.
Discussion
In this study, the effect of A. vera inner gel was performed against planktonic and sessile microbial populations. A. vera inner gel expressed its prevalent activity against Gram-negative bacteria and C. albicans in respect to Gram-positive bacteria grown in planktonic phase. This antibacterial activity could be attributed mainly to aloin and aloe-emodin, the most abundant compound identified from previously qualitative and quantitative analyses of A. vera inner gel samples. 10 These active compounds are anthraquinones that have polyphenolic structures analogue of tetracycline. It is believed that they exercise, as well established for tetracyclines, the antimicrobial activity inhibiting bacterial protein synthesis by preventing the association of amino-acyl-tRNA with the bacterial ribosome. 4
The extracted A. vera inner gel displayed also an antibiofilm activity with a general decrease of bacterial biomass. It is well known that the development of chronic infections depends strongly on the ability of microorganisms to form biofilm and, in the wound infections, biofilms produced by Staphylococcus spp. and Pseudomonas spp. increase the tolerance against antimicrobials. 11 Thus our results could give an important contribution to the management of these infections. Recent studies made by Moghazy et al. 16 demonstrated no bacterial growth on leg ulcers infected with multi-drug-resistant microorganisms after the treatment with topical A. vera gel.
In addition, Banu et al. 9 studied the cost-effectiveness of A. vera gel dressing in the treatment of diabetic foot ulcers and found that complete healing was significantly achieved in the patients together with a decrease in size and healthy granulation.
Hence, although the MIC values obtained in our study may seem high, we believe that regular application and correct concentrations of topical A. vera inner gel should affect clinical improvement with decrease in bacterial growth and restore healthy granulation tissue.
A. vera inner gel was also active against the sessile phase of clinical H. pylori strains including multi-drug-resistant strains. The anti-H. pylori properties of A. vera inner gel point to the need to find new natural therapeutic substances as adjuvant in the traditional therapies. As suggested by Pandey and Mishra, 4 A. vera inner gel could be more effective when taken orally, because, in vivo, both acemannans and anthraquinones are capable of guaranteeing their full activity. Moreover, several studies show additive and synergistic in vitro effects of plant extracts in combination with different antibiotics against H. pylori strains. 17 A. vera inner gel components, as carbohydrates, play an important role in bacterial adhesion to the host, and some oligo/polysaccharides have been reported to be effective for the inhibition of H. pylori adhesion on gastric cells. 18 This anti-adhesive effect exhibited in vitro by A. vera on gastric cells together with the antimicrobial activity against H. pylori could represent an efficacious combination to counteract the bacterial infection. An innovative floating tablet with A. vera in combination with amoxicillin by Ranade et al. 19 was developed to contrast the H. pylori-induced peptic ulcer, showing that A. vera could improve the amoxicillin adsorption through its retention in the gastric mucosa.
In conclusion, with the increasing development of antimicrobial resistance in Gram-positive and -negative bacteria being a worldwide concern, A. vera inner gel could be used in combination with antimicrobials to improve the management of the H. pylori therapy, especially in cases of multi-drug-resistance, and for an effective wound dressing.
Further studies are also required to determine the active properties of numerous other A. vera constituents and to explore the competitive or synergistic actions of particular combinations of ingredients.
Footnotes
Acknowledgements
We thank Silvia Di Lodovico and Roberta Rapini for their technical assistance. University Grant for Scientific Research (ex 60%) to Dr. Mara Di Giulio
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.