
Abstract
Experimental studies, epidemiological data, and clinical observations suggest that the gender factor is involved in the development and manifestation of IgE-dependent allergic diseases. We intend to answer the question if sex-related factors may play a role in Hymenoptera venom allergy (HVA). In the majority of recent studies the frequency of HVA symptoms with respect to both LL and SYS reactions is similar for men and women, while proven sensitization to insect venom is less frequent in women. Studies assessing clinical reactivity in HVA indicate that male sex and vespid venom allergy are factors increasing the risk of severe allergic reactions. Regarding the risk of adverse events associated with gender in the course of venom immunotherapy (VIT), the results of two large EAACI multicenter studies are discordant. In the first study, women showed increased risk of VIT adverse events. In the latter, systemic allergic side effects were not associated with gender. Despite theoretical premises and certain clinical observations indicating an important role of estrogens in allergic diseases, their influence on stinging insects’ venom hypersensitivity is not unequivocal and remains still open. Further studies on the safety of VIT in females seem to be advisable.
Introduction and objective
Sex steroid hormones, primarily estrogens, have been suggested to be responsible for the sex-dependent differences in the prevalence and clinical pictures of allergic diseases, which can be confirmed by the following observations based on epidemiological studies:
The male sex is a risk factor for asthma in childhood. At the age of 23–32 years, asthma incidence rates are equal for both sexes but are radically reversed in later adulthood when the prevalence of asthma is greater in women than in men. 1
Chronic urticaria with or without angioedema affects predominately women. 2
More women than men report the symptoms of food allergy; and the occurrence of severe symptoms of food allergy shows a female over male predominance in adolescence and adulthood of 60/40. 3
Food-associated, exercise-induced anaphylaxis is most common in female patients aged 15–35 years. 4
In most studies women outnumber men in the incidence of anaphylaxis.5,6
It has been documented that sex can be a factor determining not only the prevalence of particular allergic diseases but also their severity. It has been shown that female hormones’ fluctuations, characteristic of puberty, the premenstrual stage of the cycle, pregnancy, and menopause affect temporarily the severity of those diseases.
The abovementioned data and observations invite a consideration of gender-related prevalence rates of another allergy manifestation, i.e. hypersensitivity to Hymenoptera venoms. Hymenoptera venom allergy (HVA) occurs worldwide. Insect stings may cause local and systemic allergic reactions which are mostly IgE-dependent and largely represent the typical immediate hypersensitivity clinical picture. In Europe, sting allergy reactions are most frequently induced by social insects like honeybees, wasps, and hornets, which represent the order Hymenoptera and class Insecta. In sensitive persons, Hymenoptera stings bring about: large local reactions (HVA-LL) and systemic reactions (HVA-SYS) manifested by urticaria, angioedema, bronchospasm, cardiovascular symptoms, and anaphylactic shock. Some insect venom allergic patients develop life-threatening anaphylactic reactions which can be fatal. For adult patients suffering from all types of systemic reactions and for children experiencing respiratory and cardiovascular symptoms due to Hymenoptera venom hypersensitivity, EAACI ( European Academy of Allergy and Clinical Immunology) and AAAAI (American Academy of Allergy, Asthma and Immunology) guidelines recommend venom specific immunotherapy (VIT). VIT is established as a highly effective protection from further stings. The main limitations of this treatment are systemic adverse reactions (VIT-SAR) that affect 2.8% of wasp- and 14.2% of bee-venom desensitized patients. 7
The problem of the influence of the sex-related factor on the prevalence of HVA, the clinical reactivity to venom, and the tolerance of venom immunotherapy is complex and worth performing a comprehensive literature survey. It may have important implications for clinical practice.
Description of the state of knowledge
Gender and the prevalence of insect hypersensitivity reactions
Many clinical studies have been conducted to assess the epidemiology of HVA and specific predictors of allergic reactions to Hymenoptera venoms, but only very few of them have estimated the prevalence of such reactions for either sex separately.8–15 While analyzing the data obtained from the latter investigations, it is important to consider gender in the context of other factors affecting the incidence of HVA, reflecting the degree of exposition, such as: age (child/adult), place of residence (industrialized/rural areas), and sting rate (rarely/frequently).
A critical selective survey of epidemiological HVA investigations which consider the gender factor, both older and more recent, carried out on populations of young individuals and adults, reveals a prevailing lack of agreement among investigators as to whether the incidence of HVA reactions differs with respect to sex (Table 1). An epidemiological report of the Insect Allergy Committee of the American Academy of Allergy concludes that, under the age of 20 years, HVA-SYS reactions are less frequent in girls than boys. 16 In later studies by Settipane et al. the prevalence of HVA-SYS was comparable for girl guides and boy scouts aged 11–16 years. 17 Similarly, no significant gender-specific differences in HVA-SYS prevalence were found in a population of 10,021 schoolchildren in Israel, aged 13–14 years. 12 The prevalence rates of mild and severe systemic reactions were similar, although the boys were stung more often than girls.
Prevalence of Hymenoptera venom allergy in men and women: epidemiological studies since 1999.

Sex-related clinical aspects in insect venom anaphylaxis.
LL, local reactions; SYS, systemic reactions.
A study conducted in 1995 on the population of adult Swedes (672 men, 727 women) asserted that the prevalence of HVA-SYS was similar for both sexes for bee and wasp venoms. 18 More recent investigations, carried out roughly in the last decade (Table 1), do not settle the question if there are significant differences in HVA prevalence between the sexes as their results are often contradictory.
Some authors reported that women experienced HVA reactions less frequently than men.13,15 The reported higher incidence of anaphylaxis to Hymenoptera venom in men in these studies can probably result from differences in the degree of exposure. As more adult men than women work outdoors and do sports, they are stung more frequently than women and might therefore be at a higher risk of allergic reactions. Others investigators, conversely, found out that women are more often affected by HVA than men. 14
In the majority of recent studies, however, women’s HVA prevalence rate is viewed as similar to men’s, with respect to the incidence of both LL and SYS reactions.9–13 Comparable results estimating the prevalence of HVA as relatively equal were presented by three Spanish studies and a Polish one, performed on large populations living in industrialized urban areas of Europe.8–11 Since the European investigations were conducted in one type of environment – industrial agglomerations – their results seem to be clinically valid as the degree of exposition to stinging insects should be the same for women and men.
Gender and Hymenoptera venom sensitization
Venom sensitization, detected by the presence of specific IgE antibodies, assessed by blood test and/or skin prick test, is an indicator of possible clinical reactivity.
Very little is known about sex distribution with respect to Hymenoptera venom sensitization and our current knowledge of the issue is inconclusive. No gender difference in the sensitization ratio, confirmed by positive skin prick test to Hymenoptera venoms, was documented in a multivariate regression analysis performed on a sample of 1175 Italian children aged 74–162 months. 19 Differently, in Golden’s and Bjornsson’s studies carried out on adult populations, sensitization to bee or wasp venom was reported to be significantly less frequent in women.18,20 In the case of sensitivity to inhalation allergens the reverse has been noticed: greater incidence in teenager and adult men than in counterpart age groups of female individuals. 21
Gender and the severity of Hymenoptera venom allergy
The severity of HVA, that is the degree of clinical reactivity to insect sting in untreated persons, is determined by several identified factors such as: baseline serum tryptase concentration, degree of earlier systemic sting reactions, age, medication with ACE inhibitors, and cardiovascular co-morbidities. Undoubtedly it correlates with general immunological reactivity but not with the degree of venom sensitization. The variability of immunological reactivity at the time of the sting may be the consequence of doing physical activity, concurrent infections, additional temporary medication, alcohol consumption, or hormonal factors.
No gender difference in the severity of systemic reactions (all degrees of severity) to bee sting was found by Kalyoncu et al. investigating 786 cellulose paper factory employees and their family members aged older than 16 years. 22 Similar results were reported by Stoevesandt et al. In this single-center, retrospective, observational study conducted in a group of 657 patients with HVA (361 men, 296 women), the authors investigated the indicators and risk factors for severe anaphylaxis due to Hymenoptera stings. No relationship could be found between gender and the severity of anaphylaxis (P = 0.86). 23 Interpreting this result, the study’s retrospective approach as well as the incompatibility of field stings and challenge sting, have to be considered as a disadvantage.
A different view on that issue was presented in a recently published, multicenter prospective, European study of 962 Hymenoptera venom-sensitive patients. 24 The authors presented results indicating that male sex and vespid venom allergy were independent risk factors for severe allergic reactions to sting. Out of 962 patients, 202 (26%) had severe anaphylactic incidents following a field sting: grade 3 (anaphylactic shock, loss of consciousness) or grade 4 (cardiac arrest, apnea). Severe systemic reactions were significantly less common in women (OR = 0.553, 95% CI 0.38–0.79, P <0.001). The authors of the study interpret their results bringing up the argument that men’s greater exposure to sting may result in higher prevalence of HVA in this group of patients as well as in higher incidence of severe reactions. A possible explanation of this phenomenon can be the ‘booster effect’. The experimental and clinical studies have pointed out booster effect in other allergic diseases such as asthma. Okano et al. demonstrated that repeated intranasal sensitization to bee venom allergen (PLA2) induced serum total IgE and PLA2-specific IgE production in sensitized mice. 25
Then, whether the gender factor is decisive in HVA still remains to be resolved. Yet, if future investigations were to confirm that HVA manifests comparably frequently in men and women but men are in danger of more severe reactions, the fact could mean that female sex is ‘protected’ against severe reactions to insect venom.
These observations stand in contrast to drug induced anaphylactic reactions in which female subjects appear to be at higher risk of anaphylaxis. A significant female predominance in anaphylactic reactions was observed in IgE-mediated drug anaphylaxis induced by: penicillin, neuromuscular blocking agent suxamethonium, or gadolinium (intravenous contrast medium) in adult and pediatric patients.4,26 Similarly, more women than men manifest symptoms of anaphylaxis induced by different etiological factors, e.g. food and exercise.5,6
The predictors of VIT-SAR were analyzed in three large studies: an EAACI multicenter study, a prospective study of the Interest Group Insect Venom Allergy of the European Academy of Allergy and Clinical Immunology (EAACI) and a large single-center observational study cohort study by Stoevesandt et al.27–29 Regarding the risk factor associated with gender, the results of both studies are discordant. In the former, Mosbech et al. study, in which the incidence of systemic allergic side effects amounted to 21.2%, women showed increased risk of this kind of adverse events. 27 In the latter of the large EAACI studies by Rueff et al., SAR-VIT were reported in 8.4% (57/680) of patients and they were not associated with gender (P = 0.157). 28 Rueff et al.’s finding that the risk of serious side effects during venom immunotherapy is not associated with gender was confirmed by Muller et al. who analyzed the influence of H1 antihistamine preventive medication on honeybee venom immunotherapy (BVIT). 30 In Mueller’s study female gender was not a risk factor as calculated for all side effects and for serious side effects (requiring medication) during the increasing dose phase of BVIT. Recently Stoevesandt et al. published a study conducted in a group of 743 individuals who had 775 cycles of venom immunotherapy. 39 While the rate of objective systemic reactions was low (3.0%), subjective systemic reactions were reported more frequently (11.7%). Female sex and the incidence of VIT-SAR were not significantly related; data indicating a higher frequency of any documented VIT-SAR (objective and subjective) in women (P = 0.059) were not statistically significant.
In view of the varying conclusions of the above discussed studies and studies presented in Table 2, one aspect deserves an additional comment: their results are difficult to compare because of methodological differences in: study design, recruitment of patients, age range, the use of antihistamine premedication, gender balance, and the insect species to the venom of which patients were allergic.
Prevalence of allergic side effects during VIT in men and women in studies since 1999.
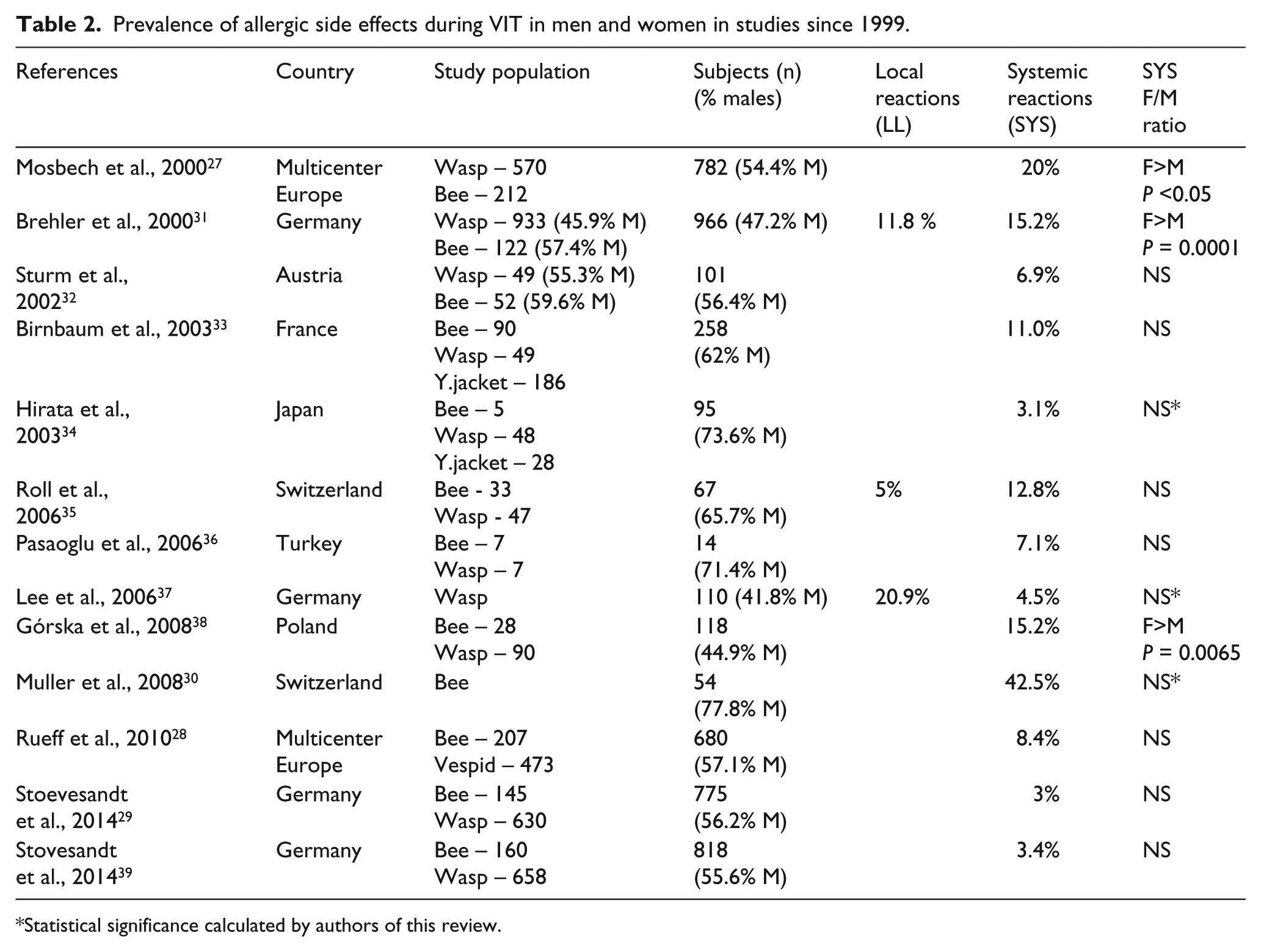
Statistical significance calculated by authors of this review.
Additionally, investigators did not use uniform definitions and classification systems of VIT-SAR as the basis for their studies; for example in the former Mosbech et al. study, all systemic allergic symptoms were assessed, while in the Rueff et al. study only those that required pharmacological interventions and which occurred during the initial phase of VIT.27,28 In turn, Stoevesandt et al. reported both objective and subjective SAR-VIT. 29 In the future, if a multicenter approach is to be assumed, it seems necessary to adopt a uniform classification system for VIT-SAR as a prerequisite to define risk factors with reference to both SARs’ general incidence and the incidence of their most severe anaphylactic manifestations.
Conclusions
Summing up, despite theoretical premises and certain clinical observations indicating an important role of estrogens in allergic diseases, their influence on stinging insects’ venom hypersensitivity is not unequivocal. There is no undisputable evidence in favor of the assertion that women are more often affected by insect venom allergy. Similarly, the data linking the prevalence of adverse events during venom immunotherapy to either sex are far from being conclusive. Despite this ambiguity, the issue of the role of estrogens in insect venom allergy is still open and in need of further investigation because estrogens actions, estrogens receptor expression and activity can be dependent by variations in hormone levels (menstrual cycle, menopause), hormone’s concentration, progesterone levels, or other exogenous influences.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.