
Abstract
The present work aimed to investigate the cellular and immunochemical pattern of T cells population in biopsy material from chronic schistosomiasis haematobium Egyptian patients complicated with bladder cancer. Digital real-time quantitative photocytometry was applied to auto-analyze 29 stained tissue sections from cases and 17 controls using STAT4, GATA3, FOXP3, and CD8 markers specific for Th1, Th2, T regulatory, and T cytotoxic cells, respectively. Area percentage showed significant high level of GATA, followed by FOXP3 and low level of both STAT and CD8 was reported. Tissue samples from five healthy bladder tissues showed significant lower optical density (OD) values. Tissue samples from 12 non-bilharzial bladder cancers showed variable OD values, reflecting wide disparity in the control group.
Our results hypothesized an exclusive pattern of T population in long standing complicated schistosomiasis haematobium. Our cases were poorly controlled by unbalanced Th1/Th2 in which Th2 was dominated. FOXP3 increased significantly, however, failed to downregulate Th2, instead, the relation between Th1 and T cytotoxic was forcibly limited by the high level of FOXP3, resulting in loss of their power in defending the host against both parasite and carcinogenic changes. These results provide more clarification for the immune evasion process played by the parasite and tumor cells under the supervision of T regulatory cells. Additionally a critical role of FOXP3 is suggested in manipulating STAT4 and CD8 in favor of malignant transformation in this life-threatening parasite.
Introduction
Schistosomal infections affect more than 240 million people worldwide and Schistosoma haematobium accounts for nearly half of that number. 1 Although the symptoms are varied, the bulk of the morbidity and mortality of urogenital schistosomiasis can be eventually accredited to the host immune response against trapped Schistosoma eggs within the tissue, resulting in inflammation, granuloma, fibrosis, and bladder dysfunction. In addition, there is increase susceptibility to malignant transformation in schistosomiasis haematobium cases. 2
In fact, the annual deaths due to urogenital schistosomiasis induced complications are about 150,000 make S. haematobium one of the most life-threatening worms worldwide. 3 Bladder cancer is the only malignancy found to be associated with S. haematobium infection. It is the first among many tropical and subtropical areas including Egypt due to endemic distribution of the parasite. 4
Toxic products secreted by Schistosoma eggs offer antigenic stimuli for the immune response. Sequestration of these antigens is usually achieved by the effect of the granulomas through T-helper type 2 (Th2) response. In addition, regulatory T cells (Tregs) help in control of the granulofibrotic response hence minimize the damaging effect on the affected tissues. 5 Therefore, strict regulation of different T lymphocytes population is crucial to prevent the development of an excessive immune response and unnecessary pathology which would be detrimental to host survival. 6 Evidently, these immune-cellular factors play an essential role in determining the nature of the future events either in good turn of the host or against him. 7 However, there are not enough data concerning the fate of the different T cells population as the infection progresses into the late chronic phase, yet, Schistosoma infection remains a neglected and underestimated cause of serious morbidity. 8
About non-bilharzial bladder cancer (BC), Sharma et al. 9 documented the presence of CD8 in non-BC and concluded that such cellular population implies an immunologically protective mechanism that confers a survival benefit. Controversial observations were reported concerning GATA3 (Th2 marker), where a significant decrease in its expression was seen by Miyamoto et al. 10 in urothelial neoplasms compared to benign urothelium. While, Liu et al. 11 recorded high expression in GATA3 and recommended its use as a sensitive and specific marker for the diagnosis of bladder carcinomas. Appling T regulatory marker, it was found that FOXP3 expression in urethral BC cells is associated with decreased long-term survival in BC invading muscle. 12
Regulatory T cells (Treg), formerly called suppressor T cells, are a subset of T lymphocytes that play a central role in inducing and maintaining immunologic tolerance and in the termination of immune responses. 7 Regulatory T cells are among the most powerful mechanisms for achieving a balanced immune response. 13 FOXP3 (forkhead/winged helix transcription factor) is considered the most accurate marker for naturally occurring T regulatory cells. 14
The present work aimed to study the cellular and immunochemical patterns of T cells population, T-helper 1 (Th1), T-helper 2(Th2), T regulatory (Treg), and CD8 in biopsy material taken from Egyptian patients suffering from chronic schistosomiasis haematobium and complicated by bladder cancer, using specific imunohistochemical markers (STAT4, GATA3, FOXP3, and CD8), respectively, performing digital real-time image photocytometry. The present study also aimed to identify the dominating T cell upon which the subsequent events had been built.
Methodology
Subjects
The present study was carried out on 29 samples of chronically infected subjects by Schistosoma haematobium and complicated by bladder cancer over the period from December 2012 to February 2014. The cases were inpatients admitted in the Urosurgery Department at Kasr Al-Ainy University, Faculty of Medicine, Cairo University. These cases were diagnosed according to their clinical, radiological, and histopathological examinations. Their inclusion criteria were based on the availability of biological material and their Egyptian nationality. The recruited patients comprised 25 men and four women (age range, 38–84 years; median age, 62 years). Tissue samples were taken from schistosomiasis cases after cystectomy and five healthy bladder tissues (taken at autopsy as a control group) in addition to tissue samples from 12 non-bilharzial bladder cancers as a second control group. All the tissue specimens were used to prepare paraffin blocks for further histopathological examination.
Light microscopy and immunohistochemical examination for tissue samples
Preparations for histological examination were performed by cutting serial sections of the paraffin blocks and staining with Hematoxylin and Eosin. 15 Epitope retrieval was performed using the Tris-EDTA buffer epitope retrieval method. The slides were incubated in Thermo Scientific Ultra Vision hydrogen peroxide block for 10 min. They were then washed twice in a buffer. Ultravision Protein Block (TA-xxx-PBQ) was applied and incubated for 5 min to block non-specific background staining. Primary antibodies for the individual markers were applied: (1) Mouse anti-human GATA3 (GATA binding protein 3): purified recombinant fragment of human GATA3 expressed in E. coli; (2) Mouse anti-human Foxp3: purified recombinant fragment of human Foxp3 expressed in E. coli; (3) Rabbit anti-human STAT4 (Signal Transducer and Activator of Transcription 4 [STAT4]): synthetic non-phosphopeptide corresponding to human STAT4 around the phosphorylation site of tyrosine 693(K-G-YP-V-P); (4) CD8 Ab-1: A13 amino acid synthetic peptide from the C-terminal cytoplasmic domain of alpha chain of human CD8 molecule.
Secondary antibody (Ultra Vision Large Volume Detection System Ant-polyvalent, HR), biotinylated goat anti-polyvalent was then applied and incubated for 10 min at room temperature. After each step the sections were washed four times in phosphate-buffered saline. One or two drops of 3,3’ Diaminobenzidine DAB Chromagen were added to 1 mL of DAB substrate, mixed by swirling and applied to the tissues, which were then incubated for 5–15 min, depending on the desired stain intensity. All chemicals were supplied from Biological, PO Box 261, Swampscott, MA, USA.
Image analysis by real-time quantitative morphocytometry
The pathological and morphometric analysis was performed using the Leica Qwin 500 Image Analyzer (LEICA Imaging Systems Ltd., Cambridge, England). The slide was examined at power magnification (100× and 200×). Optical density (OD) was automatically measured in 10 fields. Area percentage of each marker was measured in 10 fields as well on a real-time image from the microscope that was connected to a video monitor (Figure 1). The different values were saved for further analysis.

Auto-calculation of OD or area % during image analysis by real-time quantitative morphocytometry.
Statistical methods
Data were analyzed using IBM SPSS advanced statistics version 20 (SPSS Inc., Chicago, IL, USA). Numerical data were expressed as median and range or mean ± standard deviation. Chi-square test (Fisher’s exact test) was used to examine the relation between qualitative variables. For quantitative data, comparison between two groups was done using Mann-Whitney test (non-parametric t-test). Comparison between four groups was done using Kruskal-Wallis test (non-parametric ANOVA) then post-Hoc ‘Schefe test’ on variable rank was used for pair-wise comparison. A P value <0.05 was considered significant.
Results
Histopathological examination
Histopathological examination revealed different types of bladder cancer associated with bilharzial lesions: 18 sections were squamous cell carcinoma (SCC) (62.1%), seven were transitional cell carcinoma (TCC) (24.1%), and four sections were diagnosed as papillary cell carcinoma (PCC). Twenty-one cases out of the 29 cases were of high grade cancer, while eight cases were of low grade cancer. Many scattered calcified and degenerated Schistosoma haematobium eggs with their characteristic terminal spines were observed in between cancer cells. Remains of degenerated eggs was observed as well. Loose granulomas deficient in fibrous tissue with scattered lymphocytes in addition to patchy granulomas variable in size were noticed around many calcified and degenerated Schistosoma eggs (Figure 2).

(a) Loose granulomas surrounding Schistosoma haematobium eggs (arrow), remains of degenerated egg (arrow head) (Haematoxyline and eosin ×400). (b) Multiple loose granulomas in the region of degenerated, calcified Schistosoma haematobium eggs (arrow). Note the terminally located spine characteristic for Schistosoma haematobium eggs (arrow head) (Hematoxyline and eosin ×200). (c) Patchy granulomas in the region of Schistosoma haematobium eggs near cancer cells invading the muscles (Haematoxyline and eosin ×100).
Immunohistochemistry and real-time cytophotometry
Immunohistochemical patterns of GATA3, FOXP3, STAT4, and CD8 are symbolized in Figure 3. Concerning transmittance expression of different markers represented by the OD value, it was collectively 0.41 ± 0.23, reflecting more or less akin concentration in positive fields. However, when area percentage (degree of extension or horizontal broadening) of each marker was calculated, variable patterns were noticed: GATA3 and FOXP3 recorded significant superior quantity than STAT4 and CD8 (P <0.05), while no statistical significant difference was reported between STAT4 and CD8 or GATA3 and FOXP3 (P >0.05). There was no statistical significant difference in different markers when linked to tumor grade or type (P value concerning tumor type = 0.792, 0.562, 0.429, and 0.140 for GATA3, STAT4, OXP3, and CD8, respectively). With regard to tumor grade, P = 0.351, 0.452, 0.390, and 0.260 for GATA3, STAT4, OXP3, and CD8, respectively (Figures 4 and 5, Tables 1 and 2). Tissue samples from the 12 non-bilharzial bladder cancer cases showed variable OD values (median value of 0.43, 0.78 maximum and 0.09 minimum), reflecting wide disparity in this control group of cases (non-bilharzial cancer).

Immunohistochemical expression of different markers around an old Schistosoma egg (magnification power ×400).
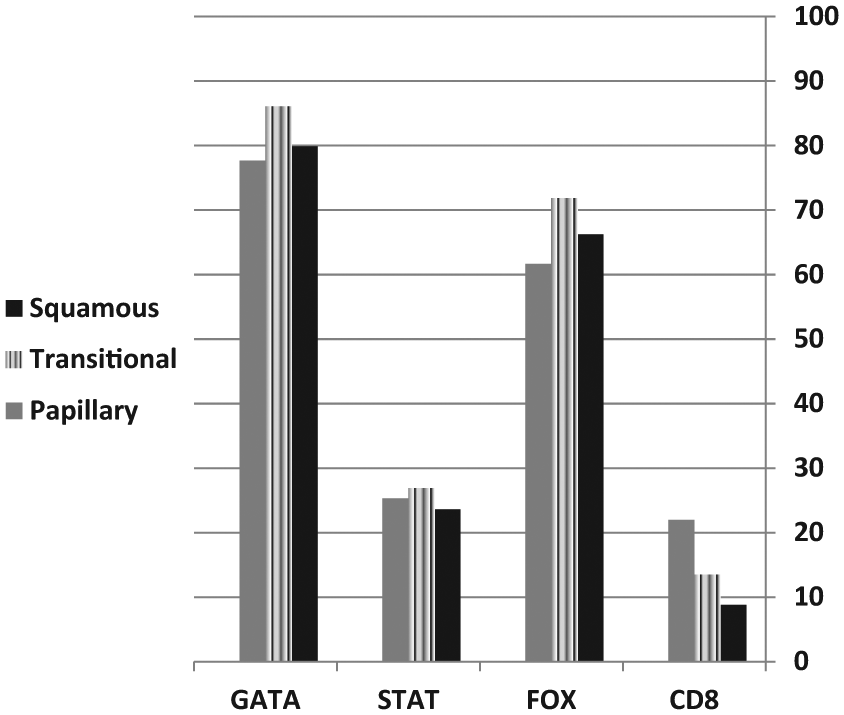
Mean area % of different markers in different tumor types.
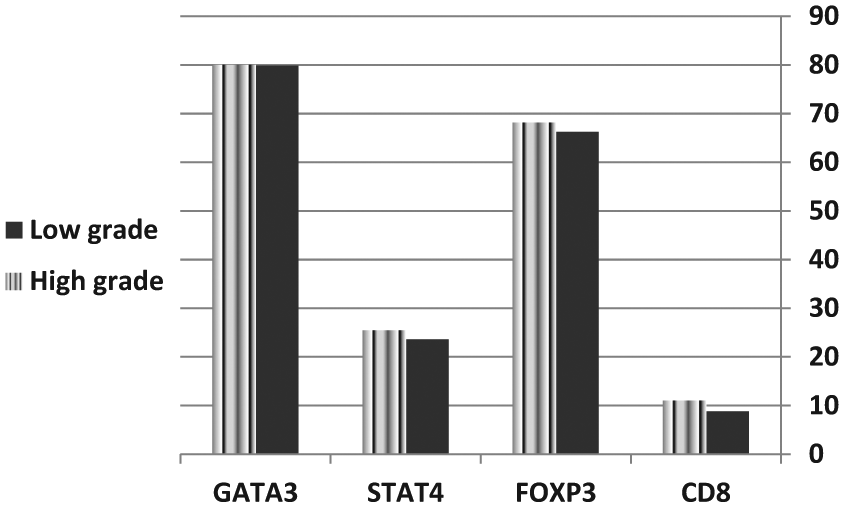
Mean area % of different markers in relation to tumor grades.
Mean ± standard deviation (SD) and P values of T cells markers in different tumor types.

Mean ± standard deviation (SD) and P values of T cell markers in relation to tumor grades.

Discussion
The more or less equivalence in the degree of transmittance (OD) in different markers recorded in the current work in bilharzial associated neoplasm in contrast to the disparity observed in non-BC suggested an exclusive pattern for the earlier. In addition, the controversial observation recorded in previous studies regarding T cells population9–12 may possibly support our hypothesis.
Concerning area percentage, results of the current study demonstrated that the horizontal infiltration of GATA3 and FOXP3 was significantly higher than STAT4 and CD8 regardless tumor types and grades. For that reason, the Th1/Th2 relation was in favor of Th2 cells domination in this late complicated phase of schistosomiasis haematobium in the 29 cases included in this work. GATA3 is a member of a transcription factor family binds to DNA sequence [A/G] GATA [A/T], hence its name. It plays an important role in promoting and directing cell proliferation, development, and differentiation in many tissues and cell types including lymphocytes. 11 Zheng and Blobel 16 recorded that in humans, GATA3 mRNA levels increased only under Th2-inducing conditions. GATA3 has already been shown to negatively regulate the development of naïve T cells into Th1. 17 This explains the down expression level of STAT4 recorded in the present study.
Despite the upregulated and dominated GATA3 in the existing study, loose and patchy granulomas, variable in size, were observed around many Schistosoma eggs. This finding raise inquiry concerning an important and uncertain issue related to the fate of the Th2 cells population as the infection progresses into the late chronic phase. The previous finding possibly explained by different theories as of Nausch et al. 8 who concluded that, repeated antigenic stimulation of T cells is recognized to result in the development of a hyporesponsive state (T cell anergy), in which Th2 cells are present but rendered inactive. 18 Several researchers have reported increased Th cell apoptosis during infection.19,20 Other groups have suggested that this observable fact possibly as a result of extrinsic factors, such as altered antigen presentation. 21
On the other hand, Wu et al. 22 reported that, antigen stimulated T cell proliferation or cytokine secretion peaks early and then declines despite ongoing infection. This process is referred to as immune-modulation status which seemed to be failed in the 29 cases included in this work and might be the cause behind malignant transformation in these cases. 23 Patchy, granulomatous lesions of variable size in the region of the trapped Schistosoma eggs were observed in the current work, and that may possibly explain the rise and fall of the Th2 response during the longstanding chronic infection in our cases.
Certainly, successful treatment of Schistosoma infection grantees sequestration of the parasitic eggs and protection of the host supported by functional immune-modulatory mechanism while the rise and fall in Th2 in the present study reflects a state of instability in immune response which may be a result of absence of treatment, failure of treatment, or repeated infection that was quite expected in our cases. In contrast, treatment failure or repeated infection caused continuity of toxic secretions from recurrently deposited eggs resulting in such fluctuation in Th2 cells.
Silva et al. 24 recorded that peripheral blood mononuclear cells from cured patients remaining highly responsive in vitro to schistosome antigen for decades following chemotherapy indicates the powerful effect of Schistosoma egg antigen. Therefore, the present work suggests that the patients in the present work were probably under the continuous powerful impact of Schistosoma antigens. Most likely, more than one factor at a time might exist in the cases included in the current research.
On the other hand, Watanabe et al. 25 recorded a decrease in T regulatory cell levels in people infected with Schistosoma mansoni after effective treatment. The significant high expression of FOXP3 (T regulatory marker) in the present work may reinforce the previous suggestion that our cases were not treated efficiently. Therefore, more work is required about the relation between anti-bilharzial therapy and the risk of development of malignancy, besides the perspective effect of chemotherapy on the stability of the immune response and on the progression or regression of severe morbidity.
Winerdal et al. 12 studied FOXP3 expression in tumor specimens from 37 cystectomized patients with non-bilharzial urinary bladder cancer and he found the FOXP3 expression among high grade tumors, invading the muscles and associated with decreased long-term survival. In our study, however, no significant difference was observed in FOXP3 expression between invading and non-invading carcinomas. It was recorded that FOXP3 expression was negatively regulated by Th2 cells. 26 Moreover, Wu et al. 22 assumed that over-expression of GATA3 in T cells led to deficient FOXP3 induction. The contrary was observed in our work in which no significant difference was recorded between values of both markers. This may support our belief in the Th2 hyporesponsive theory of Nausch et al. 8
Accumulating evidence indicates that T regulatory subset goes through expansion process during chronic inflammation and may contribute to an inadequate immune response, leading to persistent infection. 27 This explains the condition in our cases, where upregulated, expanded T regulatory cells represented by FOXP3 resulted in failure of the immune system that affected the parasitic stages or prevented the neoplastic changes.
On the other hand, STAT4, a Th1 marker (signal transducers and activators of transcription) is a family of transcription factors that regulates cell growth and differentiation. STAT4 has been demonstrated to be crucial for T cell mediated anti-tumor immune responses. 28 This response is represented in the form of cytokines released from Th1 to help the differentiation of cytotoxic T lymphocytes (CTL) and increase the expression of major histocompitability complex on affected cells, to be more sensitive to lysis by CTLs. 6 Furthermore, Th1 activates NK cells and maximizes the killing efficacy of the macrophages and the proliferation of cytotoxic CD8 T cells, thus Th1 prevent rather than promote cancer. Off course this protective function of STAT4 was deficient within the tissue specimens of our cases, since STAT4 recorded significant low expression level, consequently affects the expression of CD8 which showed as well significant low level in the current study. The presence of CD8 is recorded to be of value in the protection against malignant transformation and gives a survival benefit, in this way it may have a prognostic value in bladder cancer patients. 9
This may clarify the inhibitory role of Treg cells recorded in our study upon the cell mediated immunity against malignant transformation. Therefore, malignant cells by this time have a good chance of evading the immune system. The previous findings proposed a powerful role of FOXP3 during longstanding complicated schistosomiasis infection by the inhibitory effect of T regulatory on Th1 (STAT4) and, hence, T cytotoxic (CD8).
Our findings possibly support the immuno-editing theory reported by Pancione et al. 29 who suggested that the immune system is able to recognize and eradicate subclinical tumors, but some point of equilibrium has to be reached to affect tumor cells and remains in situ, in a state of balance with a partially efficacious response. Unfortunately, many tumors escape from this equilibrium state, and cancer becomes clinically apparent, as recorded in our cases, in which imbalanced immunological response was evident. The findings of the present study suggested that FOXP3 may be the key factor in this process which makes matters worse in longstanding bilharzial infection and the pattern seen in our cases is perhaps related to bilharzial-associated BC.
In conclusion, the present study focused on the longstanding chronically infected bladder tissue with Schistosoma haematobium and the superimposed malignant tissues to determine which prototype of T lymphocyte had been increased and led to the escape from the control of the immune system. The expected immune-modulatory mechanism between the chief phenotype of T cells (Th1/Th2) did not occur in our cases. Therefore, longstanding complicated schistosomiasis haematobium infection appears to be poorly controlled by unbalanced Th1/Th2 in which Th2 was upregulated and dominated. The high expression of Treg (FOXP3) and the low level of both Th1 (STAT4) and T cytotoxic (CD8) give more clarification for the immune evasion process played by the tumor cells under the supervision of Tregulatory cells.
It has become clear that T cell activation and differentiation is a relatively complex process regulated by a network of transcription factors and is in general somewhat understood. However, this regulatory effect plays a critical role in generating an adaptive anti-parasitic and anti-neoplasm immune response. Taken together, these new insights into T cell population in longstanding schistosomiasis infection may offer multiple novel possibilities for interventions in terms of generating valuable, practicable, and affordable anti-parasitic and anti-neoplasm therapies. Consequently, this may be considered as a step forward in the control of urinary schistosomiasis.
Further studies directed toward more complete understanding of the cellular and immunological components and their role in immunomodulation during longstanding chronic schistosomiasis are certainly needed. These issues will generate new insights into the processes that allow the regulation of different T cell responses, in addition to their important role in the development of rational and efficacious immunotherapies in the future. The current situation of this serious disease and its causative agent has to be further investigated in Egypt, especially those targeting children who are at a higher risk for infection and are more vulnerable to the development of neoplastic changes later in life due to the acquisition of infection at a young age. More work is needed on the effect of anti-bilharzial chemotherapy on the balance of the immune response, in the context of its effects both on the subsequent expression of immunity, and on the progression or regression of severe morbidity.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the National Research Committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Permission to conduct this study and ethical approval was received from the Deanship of Higher Education and Scientific Researches, Faculty of Medicine, Cairo University. The present study was conducted only on tissue biopsies of the selected cases after cystectomy. All patients were monitored regularly in the oncology outpatient clinics according to the current protocol.
Funding
Thanks for the Deanship of Higher Education and Scientific Researches, Faculty of Medicine, Cairo University for supporting and funding this research.
Informed consent
Informed written consent was obtained from all individual participants included in the study.