
Abstract
Non-cystic fibrosis bronchiectasis (nCFb) is an acquired condition of variable etiology. An impaired mucociliary clearance seems to be one of the mechanisms behind nCFb, and treatment involves antibiotics, mucoactive agents, and airway clearance techniques (ACTs). Traditional ACTs have four components: postural drainage, percussion, vibration of the chest wall, and coughing. Reviewing the international medical literature on the use of ACTs for patients with nCFb from 1989 to the present day, we retrieved 93 articles, of which 35 met our selection criteria for this analysis. We reviewed active cycle of breathing techniques (ACBT), forced expiration techniques (FET), autogenic drainage, postural drainage, oscillating positive expiratory pressure (OPep), high frequency chest wall oscillation (HFCWO), and exercise or pulmonary rehabilitation. Overall, ACTs appear to be safe for individuals (adults and children) with stable bronchiectasis; where there may be improvements in sputum expectoration, selected measures of lung function, and health-related quality of life. Unfortunately, there is a lack of RCTs in nCFb patients, especially in children. Moreover, none of the studies describes long-term effects of ACTs. It should be noted that a single intervention might not reflect the longer-term outcome and there is no evidence to recommend or contest any type of ACTs in nCFb management. Multicenter RCTs are necessary to evaluate the different techniques of ACTs especially in children with nCFb.
Bronchiectasis is a progressive condition characterized by early focal destruction of elastic tissue, damage of muscle layers and eventually destruction of the supportive cartilage and airway dilatation as shown on computed tomography (CT) scan in association with clinical symptoms of cough and sputum production. 1 Bronchiectasis can be focal or diffuse and permanent or reversible. Usually they are caused by recurrent or chronic infections or inflammations, anatomic airway obstruction, or underlying congenital disease that predisposes to bronchiectasis. The pathophysiology of bronchiectasis causes a vicious circle of airway infection and inflammation, impairing mucociliary clearance by alteration of the cilia. 2
Cystic fibrosis (CF) is the most common cause of bronchiectasis in children and is extensively studied. The global prevalence of non-CF bronchiectasis (nCFb) is not well described in the literature; but includes a variety of disease processes, most of which includes a combination of bronchial obstruction and infection. 1
Treatment methods, which improve mucus clearance, are considered essential in optimizing respiratory function and reducing the progression of lung disease. For this reason, oral or inhaled drugs 3 and chest physiotherapy are used, alone or in association, to remove secretions from the lower airways.1,4
Normal airway clearance is accomplished by the mucociliary clearance system and cough. The first depends on the methacronal wave generated by beating cilia and by the mucus layer, the physical properties of which can influence the methacronal wave. Coughing, the most efficient reserve mechanism in the central airways, relies on a high linear airflow velocity generated by ample flow and airway narrowing with a two-phase, air-liquid flow regime. The failure of one of the mechanisms may lead to sputum retention in the airways, leading to local infection and/or inflammation. 5
Traditional airway clearance techniques (ACTs) have four components: postural drainage, percussion, vibration of the chest wall, and coughing.
Due to the lack of literature on ACTs in patients with non-CF bronchiectasis, their indication is often extrapolated from other research such as CF and chronic obstructive pulmonary disease (COPD). Although understandable, such extrapolation should be performed with caution and the physiologic differences in the conditions considered carefully. Expert clinical opinion recommends that ACTs are important in nCFb to enhance mucociliary clearance, improve ventilation, manage breathlessness, and reduce cough frequency.
There are various ACTs utilized in clinical practice that range from positioning, gravity-assisted drainage, manual techniques, various breathing strategies, directed coughing, positive expiratory pressure (PEP) devices, airway oscillating devices, and mechanical tools that are applied to the external chest wall. The ACTs may be used as an isolated technique or in combination. 5
In the last 25 years (1989–2014), 93 randomized controlled trials (RCTs), uncontrolled observational studies, or case reports, reporting efficacy data of ACTs on children aged 0–18 years or on adults with nCFb were described in the international literature: PubMed Medical Subject Headings (MeSH): ‘active cycle of breathing techniques’ (ACBT), ‘forced expiration techniques’ (FET), ‘autogenic drainage’ (AD), ‘postural drainage’ (PD), ‘oscillating positive expiratory pressure’ (OPep), ‘high frequency chest wall oscillation’ (HFCWO), ‘exercise’, ‘pulmonary rehabilitation’, and ‘humidification’, each of them combined to ‘bronchiectasis’).
However efficacy between different techniques of ACTs have been compared, there is no published evidence to indicate which ACTs should be implicated in nCFb and which patients may benefit from the different ACT devices. However, it is widely believed that a routine airway clearance regimen is an important component of the management of nCFb in order to improve mucociliary clearance and reduce cough frequency. 1
In this review we have evaluated 93 articles, 58 of which were rejected on the strength of our analytical criteria, while 35 on nCFb were considered eligible for this review (Figure 1).
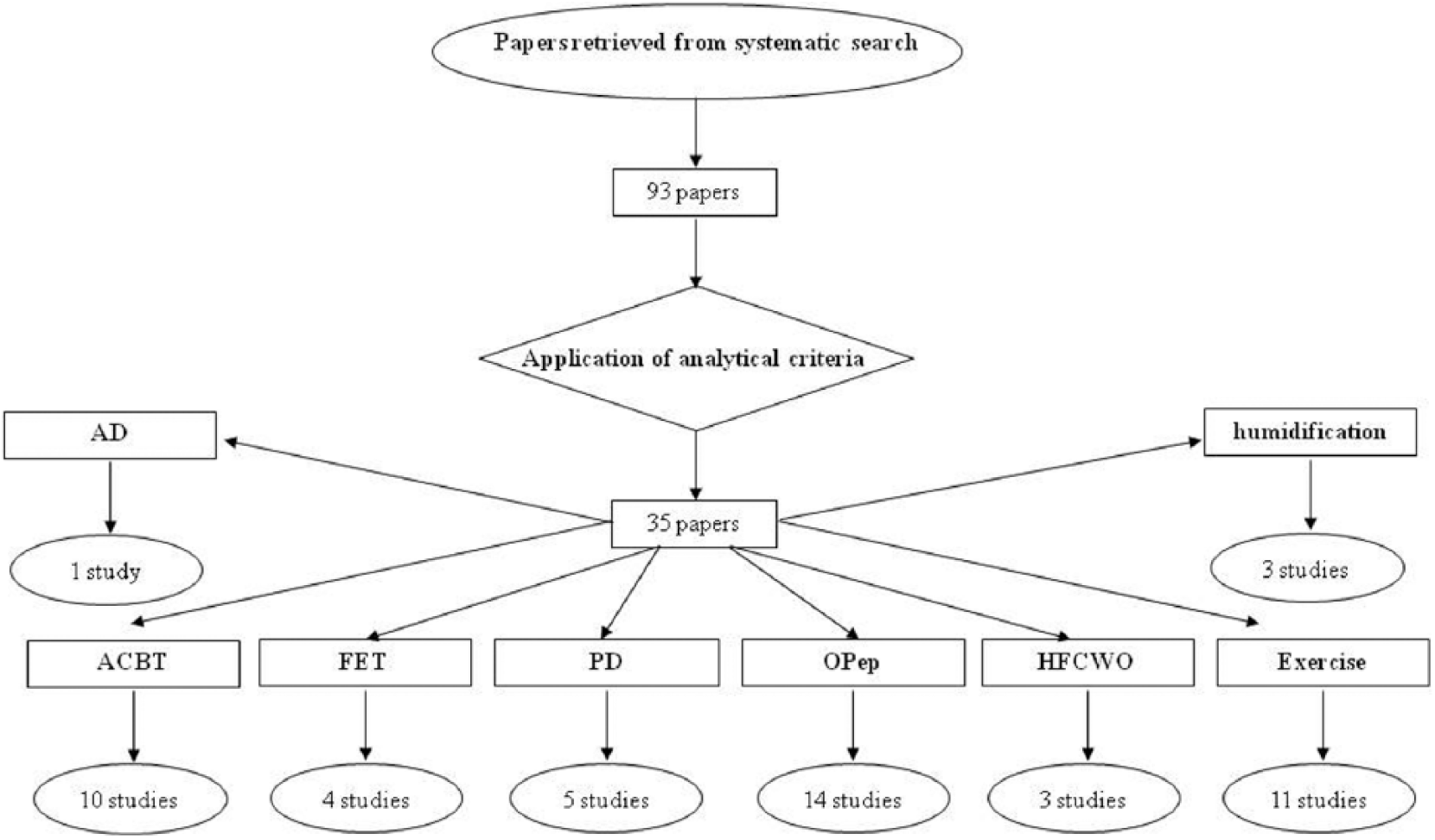
Flow chart of literature review on nCFb and ACTs. Results of the systematic literature search on pediatric nCFb in the English-language medical literature from 1989 to 2014. ACT: airway clearance techniques; ACTB: active cycle of breathing techniques; AD: autogenic drainage; FET: forced expiration techniques; HFCWO: high frequency chest wall oscillation; nCF: non-cystic fibrosis bronchiectasis; OPep: oscillating positive expiratory pressure; PD: postural drainage.
ACBT is frequently utilized in nCF bronchiectatic patients.1,5 –15 It can be used in conjunction with manual techniques (e.g. chest clapping and shaking) and postural drainage. The studies on the efficacy of ACBT in patients with nCFb (Table 1) show that ACBT improves lung sounds, sputum expectoration, and reduces perceived breathlessness. ABCT have a more acute efficacy in adults in comparison with OPep devices as show in four RCTs.9,10,13,15 No trials on children have been reported in nCFb.
Studies on the effect of ACBTs on nCFb.

Author’s name and reference number in brackets under the year.
ACT: airway clearance techniques; ACTB: active cycle of breathing techniques; ACBT-PD: ACBT plus postural draining; AD: autogenic drainage; ELTGOL: l’expiration lente totale glotte overte en decubitus lateral; FRC: functional residual capacity; HS: hypertonic saline; IS: isotonic saline; PD: postural drainage; Pep: positive expiratory pressure; RCT: randomized controlled trial; RV: residual volume; TIRE: test of incremental respiratory endurance; TLC: total lung capacity.
FET or ‘huffing’ is considered an alternative to coughing for the removal of lung secretions and airways clearance. It is supposed to reduce transpulmonary pressure compared with cough, avoiding airway compression and closure. The four articles in this review7,15–17 show that FET is an effective ACT mainly when preceded by inhalation therapy; however, no control studies with other ACTs in nCFb have been reported (Table 2).
Studies on the effect of forced expiration techniques in children and adults with nCFb.

Author’s name and reference number in brackets under the year.
ACTB: active cycle of breathing techniques; AD: autogenic drainage; ELTGOL: l’expiration lente totale glotte overte en decubitus lateral; FRC: functional residual capacity; Pep: positive expiratory pressure; PD: postural drainage; RCT: randomized controlled trial; RV: residual volume; TLC: total lung capacity.
AD is an ACT that employs controlled expiratory airflow during tidal breathing to mobilize secretions in the peripheral airways and distribute them centrally, in order to facilitate its elimination. Its efficacy has been briefly studied in CF patients, but only one article on AD has been published in patients with nCFb. 15
PD has been reported in patients with nCFb in five RCTs,8,9,10,14,18 especially in combination with ACBT, increases sputum yield (Table 3).
Studies on the effect of postural drainage in children and adults with nCFb.

Author’s name and reference number in brackets under the year.
ACT: airway clearance techniques; ACTB: active cycle of breathing techniques; ACBT-PD: ACBT plus postural draining; AD: autogenic drainage; OPep: oscillating positive expiratory pressure; PD: postural drainage; RCT: randomized controlled trial; TIRE: test of incremental respiratory endurance.
OPep techniques increase clearance of pulmonary secretions, improve exercise capacity, and reduce cough severity (Table 4). In literature on nCFb, these devices consist in Acapella®, Flutter®, and UNIKO®, and habitually are preferred over regular ACTs such as ACBT and PD.7,10,13,15,18–27
Studies on the effect of oscillating positive expiratory pressure in children and adults with nCFb.

Author’s name and reference number in brackets under the year.
ACT: airway clearance techniques; ACTB: active cycle of breathing techniques; ACBT-PD: ACBT plus postural draining; AD: autogenic drainage; ELTGOL: l’expiration lente totale glotte ouverte en decubitus lateral; FEF25-75: forced expiratory flow at 25–75% of FVC; FRC: functional residual capacity; FVC: forced vital capacity; MEP: maximum expiratory; MIP: maximum inspiratory pressure; OPep: oscillating positive expiratory pressure; PD: postural drainage; Pep: positive expiratory pressure; PFT: pulmonary function tests; PR: pulmonary rehabilitation; RCT: randomized controlled trial; RV: residual volume; SGRQ: St George’s Respiratory Questionnaire; TIRE: test of incremental respiratory endurance; TLC: total lung capacity.
HFCWO refers to the application of positive pressure air pulses to the chest wall usually by means of inflatable vest. There are few published studies (Table 5) available to evaluate its indications and benefits in patients with nCFb,28–30 but its use shows a trend in reduction of sputum expectoration and an improvement in symptoms and quality of life.
Studies on the effect of high frequency chest wall oscillation in children and adults with nCFb.

Author’s name and reference number in brackets under the year.
Reduced exercise tolerance may be a problem for children with non-CF bronchiectasis. On the other hand, physical training has been shown to improve exercise tolerance and reduce symptoms of breathlessness in many patient populations including CF and COPD (Table 6). There is little information regarding the benefits of physical training in bronchiectasis: however it is probable that the benefits of physical training in bronchiectasis are at least comparable to benefits demonstrated in other respiratory conditions.20,31–40
Studies on the effect of exercise in children and adults with nCFb.

Author’s name and reference number in brackets under the year.
Humidification is used as an adjunct to chest physiotherapy (Table 7), showing even just humidificated air improves effects of ACT in patients with nCFb, increasing sputum yield and improving mucociliary clearance and lung function.16,17,41
Studies on the effect of humidification children and adults with nCFb.

Author’s name and reference number in brackets under the year.
From a recent survey in Italy among children with PCD (primary ciliary dyskinesia), PEP techniques are the most frequently prescribed ACTs; variable from normal PEP devices to OPeps.
Overall, ACTs appear to be safe for individuals (adults and children) with stable bronchiectasis, where there may be improvements in sputum expectoration, selected measures of lung function, and health-related quality of life.
Unfortunately, there is a lack of RCTs in nCFb patients, especially in children. Moreover, none of the studies describes long-term effects of ACTs. It should be noted that a single intervention might not reflect the longer-term outcome and there is no evidence to recommend or contest any type of ACTs in nCFb management. Multicenter RCTs are necessary to evaluate the different techniques of ACTs, to improve indication and be able to select best ACTs for every patient, especially in children with nCFb.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This review has been funded by the Italian Health Ministry (RF-VEN-2008-1201767).