
Abstract
Anaphylaxis is a severe, life-threatening, generalized, or systemic hypersensitivity reaction. The diagnosis is mainly based on a clinical ground. This study aimed to evaluate the records of both phone calls and medical visits for anaphylaxis managed by the Liguria Medical Emergency Service (MES) in a pediatric population, occurred during 2013. The phone call is managed at each center and classified according to a level of care intensity and a presumed level of criticality, according to established criteria. Criticality is then re-evaluated (detected criticality) at the end of the medical visit following the same score adding the black code for patients who died. Most of the phone calls (86) to the MES were recorded in summer (40.7%), followed by spring (26.7%), autumn (16.3%), and winter (16.3%). Forty-eight patients (55.8%) were male. Anaphylaxis was confirmed in about half of patients. In addition, almost all subjects (97.7%) were referred to the Emergency Room. In conclusion, the present study shows that anaphylaxis represents a serious and relevant medical problem in the pediatric population and should be ever carefully managed.
Introduction
Anaphylaxis represents a very relevant medical issue in the pediatric population, as it is a severe, potentially fatal, generalized, or systemic hypersensitivity reaction. 1 Anaphylaxis diagnosis is likely when any of the following three criteria are fulfilled: (1) acute onset of an illness with involvement of skin/mucosal tissue and airway compromise or reduced blood pressure or associated symptoms; (2) two or more of the following after exposure to known allergens for the patient: history of severe allergic reaction, skin/mucosal tissue, airway compromise, reduced blood pressure, gastrointestinal symptoms (for food allergy); (3) hypotension after exposure to known allergens for the patient. 2 The updated World Allergy Organization Guidelines re-evaluated the anaphylaxis diagnosis and its management. 3
It is to note that infants and teenagers have increased vulnerability to anaphylaxis in comparison with the general population. Co-morbidity with severe or uncontrolled asthma, mastocytosis, and concurrent use of some medications and exercise increase the risk of severe or fatal anaphylaxis. Food is the most important trigger in childhood. 4 Drugs, stinging insects, and latex are other triggers for anaphylaxis.
The diagnosis of anaphylaxis is based on a clinical approach. It should be considered the presenting signs and symptoms. Fortunately, only a few kinds of food, including eggs, milk, peanuts, fish, soybeans, and wheat, may be cause of anaphylaxis in children and adolescents. In this regard, there are some studies that addressed this topic, also including this clinical feature.4–7
A very recent study retrospectively analyzed the patients with anaphylaxis observed at the pediatric Hospital Istituto Giannina Gaslini of Genoa. 8 Therefore, this study aimed to evaluate the records of both phone calls and medical visits for anaphylaxis managed by the Liguria Medical Emergency Service (MES) in a pediatric population during 2013.
Materials and methods
Liguria is a northwestern Italian region, with about 1.6 million inhabitants and about 220,000 minors. MES is widespread, present in the territory with five centers and 18 medical stations. The service is available 24 hours.
The calls due to suspected anaphylaxis for pediatric population (ages 0–17 years) were evaluated during 2013.
The phone call is managed at each center and classified according to level of care intensity and a presumed level of criticality, according to established criteria (http://www.emergencydispatch.org/it). Care intensity is scored according to level, ranging from the less relevant Omega to the progressively more severe levels (Alpha, Bravo, Charlie, and Delta) until the most critical Echo. Presumed criticality is initially defined at the center on a scale based on colors: white (mild), green (moderate), yellow (severe), and red (life-threatening). Criticality is then re-evaluated (detected criticality) at the end of the medical visit following the same score adding the black code for patients who died.
Diagnosis of anaphylaxis was based on clinical criteria,1,2,3 such as: suggestive clinical history consistent with presenting symptoms, i.e. the demonstration of a cause/effect dependence between exposure to the potential causal trigger and occurrence of anaphylaxis clinical features (post hoc ergo propter hoc). Cardiovascular features were: hypotension, impairment of conscious state, pale and floppy presentation; respiratory features were: breathlessness, tongue or throat swelling, throat tightness, stridor, talking difficulty, wheezing, cough, and tachypnea; gastrointestinal features were: vomiting, colic, and diarrhea; skin features were: angioedema, urticaria, itching, and erythema.
Statistical analysis
Epidemiological, demographic, and clinical profiles of patients are reported as count and percentage within each category. The annual incidence of the calls for suspected anaphylaxis was calculated by referring to the total number of Ligurian pediatric population in the year 2013.
Results
Table 1 shows the demographic and clinical characteristics of patients reporting anaphylaxis. Globally, 86 calls occurred during 2013.
Descriptive analysis of the total sample (n = 86), and for age subgroups. Frequency data are expressed as count and percentage within each category.
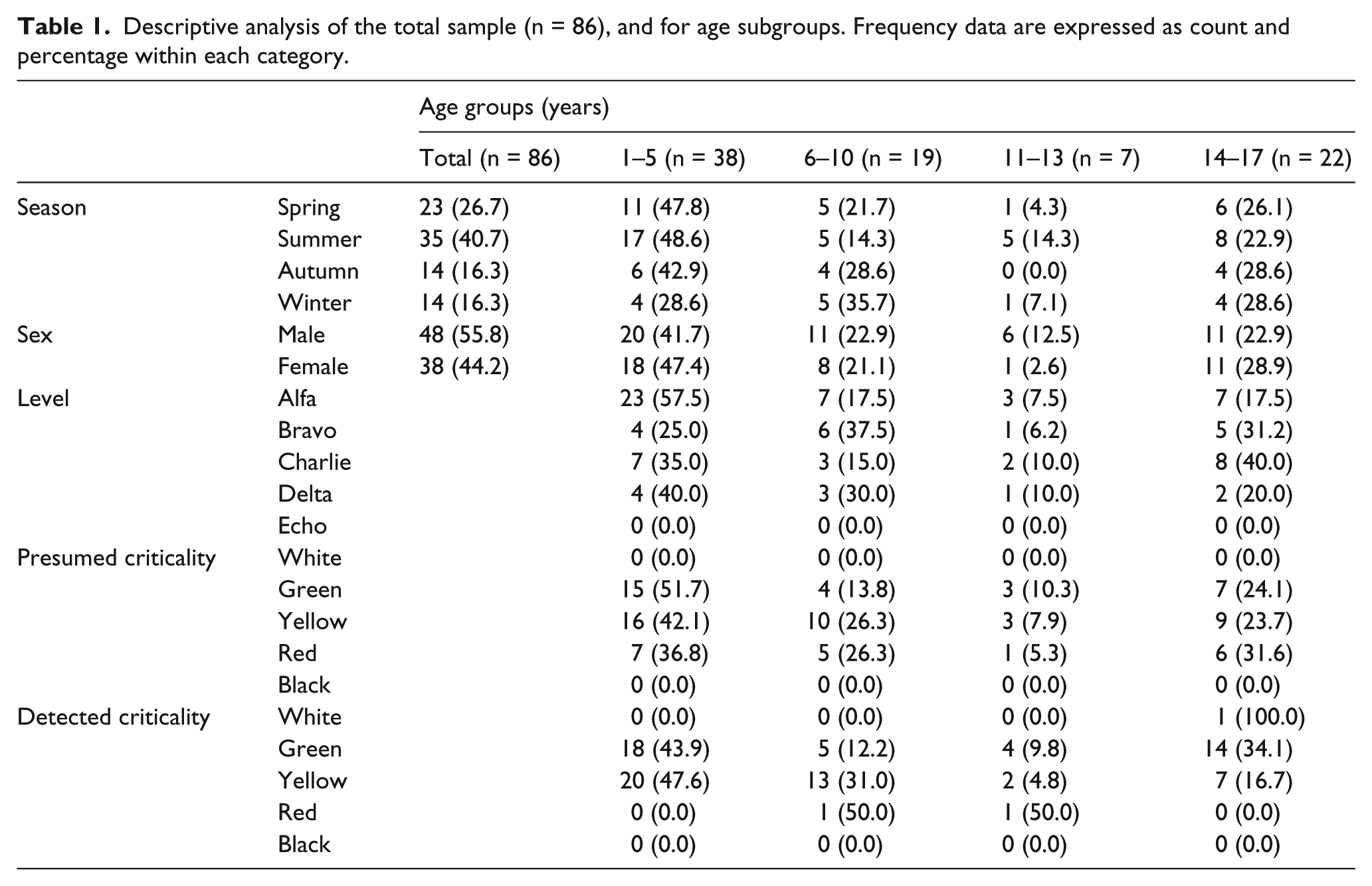
Most of the phone calls to the MES were recorded in summer (40.7%), followed by spring (26.7%), autumn (16.3%), and winter (16.3%). Forty-eight patients (55.8%) were male, and the mean age was 8.1 ± 5.38 years.
The most important levels of care intensity were Alpha (46.5%) and Charlie (23.3%). Regarding the distribution of presumed criticality, the yellow score was the most frequent (44.2%) followed by green (33.7%) and red (22.1%). On the other hand, regarding the detected criticality, yellow score was the most frequent (48.8%) followed by green (47.7%) and only two patients with a red code.
Figure 1 shows the distribution of patients’ ages. Interestingly, there are no child aged 11 years. The sample was subdivided into four sub-groups on the basis of four age ranges: 1–5 years (preschoolers), 6–10 years (primary school), 11–13 years (junior high school), and 14–17 (senior high school) as reported in Figure 1. The highest frequency corresponded to preschoolers (44.2%), followed by adolescents (25.6%), primary school children (22.1%), and junior high school children (8.1%). Male children were predominant in all sub-classes but in the adolescent sub-group.
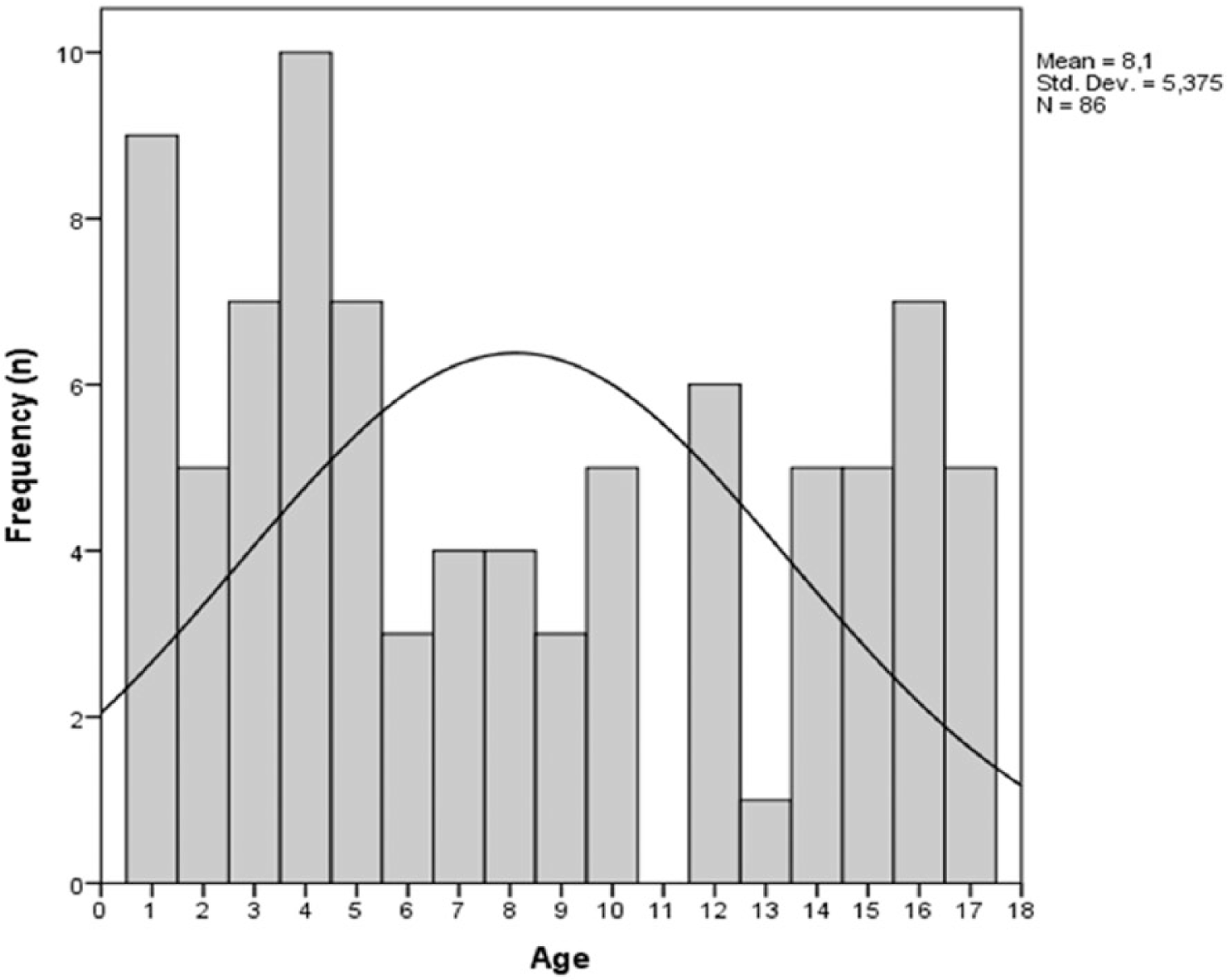
Distribution of cases according to age.

Distribution of cases according to age and gender.
There was no death for anaphylaxis during 2013 in Liguria.Eighty-four patients (97.7%) were transported to the Emergency Room.
Intramuscular adrenaline was injected in all yellow and red cases, usually associated with systemic corticosteroids.
Discussion
The present survey demonstrates some interesting findings. First, the highest frequency of phone calls for anaphylaxis occurred during summer (40.7%) and spring (26.7%), more than two-thirds of the global sample. This fact might be dependent on the prevalence of outdoor activities in these seasons and the abundance of potential triggers, such as fruits and insects. In addition, male predominance is consistent with previous studies.4–9
Second, the younger children have anaphylaxis more frequently than older patients. This outcome is particularly relevant form a clinical point of view. This outcome substantially confirms the literature data and might depend on the predominance of egg and milk allergy during infancy. On the other hand, anaphylaxis in adolescents might depend on different dietary habits, including hidden and dangerous foods.
Third, anaphylaxis was confirmed in about half of cases, corresponding to red and yellow scores. In particular, it is to note that there is a trend to overestimate the clinical severity by patients or observers. In fact, the severity of the red code was confirmed only in about one-tenth of cases. On the other hand, about half the calls corresponded to less severe allergic or non-allergic reactions. However, almost all subjects (97.7%) were referred to the Emergency Room. This aspect underlines the relevance that deserves this issue.
The limitations of this study are the lack of details concerning the clinical presentation and the lack of triggers definition, such as allergy diagnosis, including tryptase assay. These shortcomings depend on the particularity of medical records used by MES and, of course, on the peculiarity of MES deputed to emergency care.
On the other hand, the studies conducted in Italy about anaphylaxis addressed specific causes of anaphylaxis, such as food or hymenoptera allergic reactions, or concerned the experience of single Emergency Department. Therefore, the present study is, to the best of our knowledge, the first report concerning anaphylaxis management by a regional Italian MES. Obviously, further studies should be conducted addressing the limitations of the present survey, mainly concerning the ER documentation and allergen-specific causality.
In conclusion, the present study shows that anaphylaxis represents a serious and relevant medical problem in the general population at any age and should always be carefully managed.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.