
Abstract
The purpose of our study was to critically evaluate the results obtained from a guided tissue regeneration technique after 12 months using a bocomposite poly (lactic-co-glycolic) acid/sub-micron size hydroxyapatite (PLGA/HA) with a rubber dam as a barrier in smoking and non-smoking patients. We selected 36 patients (18 current smokers and 18 non-smokers) diagnosed with chronic advanced periodontitis with a periodontal site (probing depth [PD] >5) amenable to regenerative surgery. Twelve months after surgery, the periodontal parameters were found to have statistically improved, when non-smokers were compared with smokers, in: PD reduction (6.3 ± 2.1 mm vs. 3.6 ± 1.9 mm); CAL gain (4.4 ± 1.1 vs. 2.8 ± 2.2 mm); recession (1.8 ± 1.4 mm vs. 0.8 ± 0.9 mm); and hard tissue fill (4.7 ± 0.8 mm vs. 2.8 ± 2.1 mm). Furthermore, since we found PD baseline differences between groups, smoking seemed not to influence the outcomes achieved (CAL gain and ΔREC) 12 months post surgery with respect to PD baseline. The use of PLGA/HA with a rubber dam significantly improved the periodontal parameters in both smoking and non-smoking subjects. This improvement was nevertheless lower in smokers than the non-smokers, confirming the negative impact of smoking on periodontal regeneration.
Keywords
The ideal goal of periodontal therapy is the regeneration of the periodontium compromised during active periodontitis. Many investigations demonstrated clinical improvements obtained with periodontal treatments for intrabony defects.1–4
Salama et al. 5 proposed the use of a rubber dam as an alternative material to extended polytetrafluoroethylene (e-PTFE) for guided tissue regeneration (GTR) technique, obtaining remarkable clinical results. Recently, Nagarale et al. confirmed that using a rubber dam as a barrier yields good results in clinical implications. 6
Stavropoulos et al. in 2004 7 documented the negative influence of smoking on regenerative procedures with resorbable membranes. In fact, smoking accelerates periodontal tissue destruction involving IFN-gamma production in gingival tissue 8 and it is associated with tooth loss in an exposure-dependent manner. 9 Furthermore, cigarette smoke reduced the self-healing capacity of periodontal tissues 10 and it is one of the factors that has a detrimental effect on periodontal treatment outcomes. 11 The hydroxyapatite-based biomaterials proved to promote periodontal regeneration and bone formation.5,12
Several studies have shown that biodegradable polymer/bioceramic composites can improve bone regeneration as compared with conventional composites by optimizing controlled resorption, osteogenesis, and osteointegration.13–16 Biocomposite poly (lactic-co-glycolic) acid hydroxyapatite (PLGA/HA)’s bone-like foam scaffold, osteoconductivity, and increased hydrophilic surface could provide an environment for the stimulation of bone re-generation. 13
There are no data regarding the effect of smoking on the clinical and radiographic outcomes from the guided tissue regeneration technique with PLGA/HA and a rubber dam as a barrier.
The purpose of this study was to compare the results obtained from a guided tissue regeneration technique using PLGA/HA with an alternative barrier like a rubber dam on smoking and non-smoking patients.
Materials and methods
Patients
Thirty-six patients affected by chronic periodontitis (21 men, 15 women; average age, 41.8 years ±12), 18 current smokers (20 cigarettes/day) and 18 who had never smoked, 17 were enrolled in the study after signing an informed consent.
Antibiotic therapy within the previous 6 months, pregnancy or lactation, periodontium-affecting drugs like cyclosporine, history of allergies, systemic complications, and periodontal surgery for periodontitis during the previous 2 years were considered grounds for exclusion, as were drug allergies or relevant pathologies potentially contraindicating periodontal surgery.
The inclusion criteria were evidence of one osseous defect at monoradicular teeth or at furcated teeth not involving the furcation area with a probing depth (PD) ⩾6 mm and osseous radiographic defect depth ⩾3 mm.
All patients received initial therapy including oral hygiene instruction, full-mouth scaling, and root planning utilizing 40 mg/mL of articain hydroclorid with 1:100,000 epinephrine and occlusal adjustment when indicated. Reevaluation examinations were accomplished 2 months after initial therapy to determine patient response to the therapy and to confirm the need for periodontal surgery.
Surgical therapy was planned only once plaque control was found to be ⩽10% based on the O’Leary plaque index. 18 The study was approved by the Ethics Committee of Polytechnic University of Marche, Torrette, Ancona, Italy. Clinical measurements and radiographic examination were described in our previous study 1 and were recorded by the same examiner (SDA). Briefly, the following measurements were expressed in mm: PD; clinical attachment level (CAL); gingival recession (REC); distance cemento-enamel junction (CEJ)-base of the defect (BD) or CEJ-BD; distance CEJ-alveolar crest (AC) or CEJ-AC; and distance AC-BD.
The differences between 12 months and baseline clinical values for PD, CAL, and REC were PD reduction, CAL gain, and ΔREC, respectively. The differences between 12 months and baseline radiographic values for CEJ-BD, AC-BD, and CEJ-AC indicated the amount of the bone gain, also defined as hard tissue fill (HTF), base defect resolution (BDR), and bone resorption, respectively.
Surgical procedure and follow-up
The same surgeon performed all operations. After mucoperiosteal flap access, soft tissue debridement and root planning were accomplished with hand/ultrasonic instruments, rotating diamond stones and finishing bars. After root conditioning with 24% ethylenediaminetetraacetic acid pH 6.7 (Prefgel, Straumann Biologic Division, Waltham, MA, USA) for 2 min, the surgical area was thoroughly irrigated with sterile saline solution, as described previously. 1 For all surgical sites, PLGA/HA (ReOss®, Intra-lock System Europa S.p.A., Salerno, Italy) was used to support the rubber dam. PLGA/HA has a multi-pore three-dimensional architecture that created an environment for new bone growth. The scaffold also provided a hospitable adhesive substrate used as strong physical support for the infusion and growth of blood and bone cells. The entire structure was an intricate, highly interconnected matrix with enhanced hydrophilic properties. Through a patented process utilizing barosynthesis, the biomaterial’s highly porous, synthetic polymer foam was permeated with osteoconductive sub-micron sized particles of hydroxyapatite. 16 The rubber dam (Nic Tone ® Rubber Dam, Dental Continental S.A. de C.V, Zapopan, Jalisco, Mexico) was prepared according to Cortellini and Pini-Prato in the 1984 protocol for proper disinfection; 19 it was then trimmed and fit onto the periodontal defects with the aid of as many holes as the number of teeth involved in the area required, allowing its insertion around them. Lubricated dental floss (GUM-Sunstar, Etoy, Switzerland) was used to help position the barrier. At this point the barrier was stabilized and the buccal and lingual/palatal barrier wings were easily sunk underneath the gingival tissue, ensuring that the defects would be covered entirely with its margins reaching at least 3 mm beyond the defect rims (Figure 1a). No suture was needed for barrier stabilization. The flaps were released through horizontal periosteal incision at the base and sutured in a tension-free fashion with a 5.0 undyed absorbable polyglycolic acid suture (Bondek® Plus, Teleflex Medical Europe Ltd., Athlone, Ireland; previously distributed by Butterfly Italia, Milan, Italy) (Figure 1b). Every patient was prescribed antibiotic bacampicillin hydrochloride 1,200 mg twice a day × 5 days (BACACIL, Rottapharm SpA, Monza, Italy), starting 1 day prior to surgery; anti-inflammatory agent Piroxicam 20 mg/daily for 10 days (CICLADOL, Farmaplanet, Venice, Italy); 500 mg vitamin C, two tablets per day (CEBION, Bracco Group, Milan, Italy). Patients used mouthwashes with 0.20% chlorhexidine gluconate (Corsodyl, GlaxoSmithKline, Verona, Italy), for 60 s, three times daily for the first 2 weeks following surgery. In addition, they were instructed not to brush or floss in the areas where surgery had been performed for at least 10 days. Check-up visits were carried out weekly until barrier removal. No adverse reactions were noted in any patient; recession occurred in all treated cases, becoming more evident at the second postoperative week leaving part of the barrier exposed. After 4–6 weeks, the barrier was easily removed, leaving an abundant magenta red, gelatinous tissue that was preserved by coronally repositioning of the flaps as much as possible such that the maturation of the newly formed tissue would proceed undisturbed (Figure 1c). Every 3 months, a supportive periodontal treatment was provided to maintain a healthy periodontal state. Twelve months after surgical therapy, the clinical parameters were re-evaluated (Table 1) and radiographs were taken.

(a) Positioning of the rubber dam barrier after flap elevation (arrows); (b) flap closure in a tension-free fashion with suture (arrow); (c) abundant gelatinous tissue (arrow) 4–6 weeks after positioning of the rubber dam barrier.
Mean ± SD of clinical and radiographic parameters (Baseline and after 12 months) and statistical analysis.
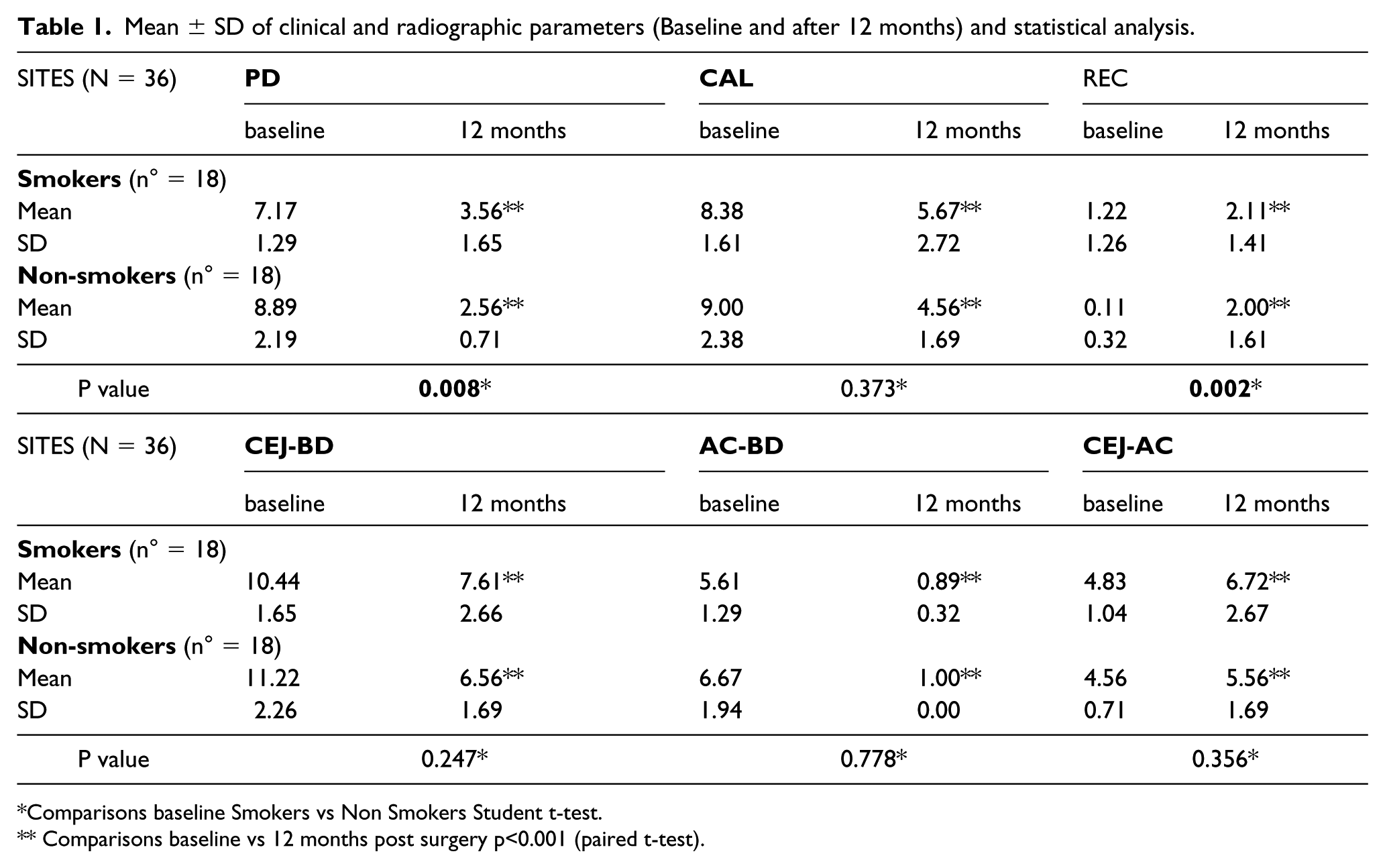
Comparisons baseline Smokers vs Non Smokers Student t-test.
Comparisons baseline vs 12 months post surgery p<0.001 (paired t-test).
Statistical analysis
Results were expressed as means ± standard deviation (SD). Univariate analyses were performed by two-tailed Student’s t-test at baseline between test and control groups. The values of baseline parameters were compared with the values of 12-month post-surgery parameters for each group by two-tailed paired t-test. Delta values of clinical and radiographic parameters between test and control groups were compared by the Student’s t-test.
The test and control groups of clinical and radiographic parameters were compared using one covariate (PD baseline) by ANCOVA to assess the effect of the PD baseline to smoking. Furthermore, since we found PD baseline differences between groups, we studied the effect of this variable on the outcomes achieved in respect to smoking.
Statistical analysis was performed with SPSS ver17.0 (SPSS Inc., Chicago, IL, USA) and the significance was accepted if the null hypothesis was rejected at P <0.05.
Results
All the enrolled subjects completed the study. All sites healed uneventfully. At 12 months post surgery, we found a statistically significant improvement of the periodontal parameters for the 36 treated sites in both smokers and non-smokers, as shown in Table 1. No significant complications, such as infection, unusual pain, or purulence, emerged.
When comparing the baseline CAL, CEJ-BD, AC-BD, and CEJ-AC between the study groups, no statistically significant difference emerged, except for the PD and REC. A comparison of patients within their respective study groups showed that the treatment of intrabony defects with allograft and an alternative dam, in both smokers and non-smokers, led to an overall clinical improvement in the PD and CAL. At 12 months, the PD decreased in the smokers and non-smokers from 7.17 to 3.56 mm and from 8.89 to 2.56 mm, respectively, compared to the baseline (Table 1). In fact, the reduction in PD was 3.61 mm in the smokers and 6.33 mm in the non-smokers, demonstrating a greater statistically significant PD reduction at 12 months in non-smokers compared to smokers (Table 2).
Δ values (mean ± SD) and adjusted means of Δ values for PD baseline (ANCOVA test) between baseline and 12 month post-surgery and statistical analysis.
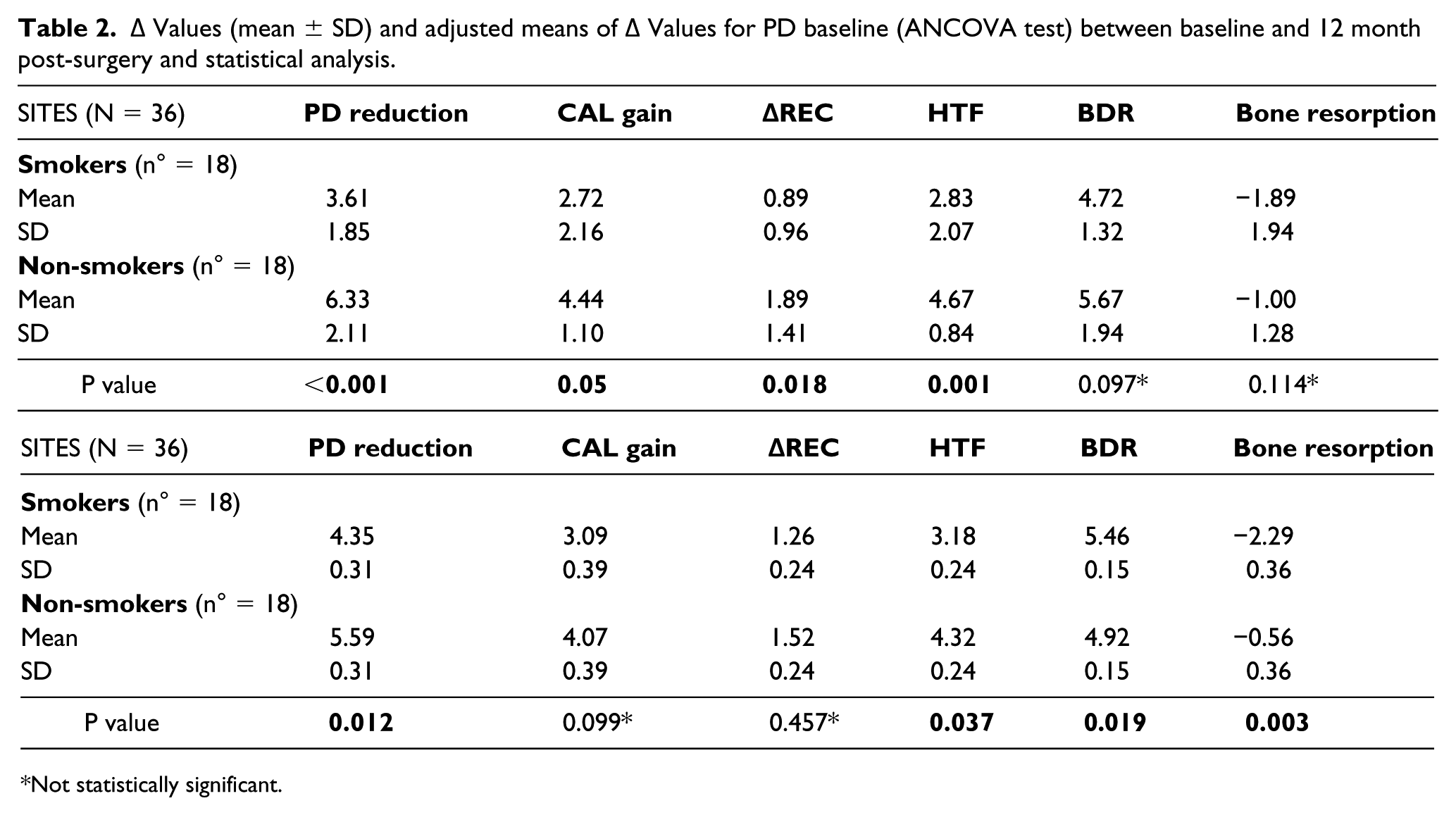
Not statistically significant.
At 12 months, there was a significant decrease in CAL in both study groups, compared to baseline (Table 1). In fact, in the smoking and non-smoking subjects, CAL was decreased from 8.38 to 5.67 mm and from 9.00 to 4.56 mm, respectively. Then, compared to the baseline, the CAL gain was 2.72 mm in smokers and 4.44 mm in non-smokers (Table 2), with a greater statistically significant CAL gain and ΔREC at 12 months in the non-smoking group compared to the smoking group (Table 2).
Compared to the baseline, the radiographic CEJ-BD and AC-BD at 12 months showed a statistically significant decrease in both study groups (Table 1). At 12 months, the HTF and BDR were 3.18 mm and 5.46 mm in the smoking group and 4.32 mm and 4.92 mm in the non-smoking group, respectively. The radiographic bone change did not statistically differ between the groups, except for HTF which was greater among non-smokers (Table 2).
The clinical and radiographic Δ values (baseline to 12 months), in non-smoking and smoking individuals, were presented as box and whisker plots in Figure 2.

Box and whisker plots of clinical and radiographic Δ (baseline to 12 months) values in non-smokers and smokers.
Table 2 shows the comparison of Δ values adjusted for the covariate PD baseline between the smoking and non-smoking groups. ANCOVA was performed to evaluate whether the differences found between study groups could depend on the covariate PD baseline rather than on smoking. Compared to the baseline, the PD reduction and CAL gain were 4.35 mm and 3.09 mm in smokers, and 5.59 mm and 4.07 mm in non-smokers, respectively. Furthermore, the differences in CAL gain and ΔREC at 12 months were not statistically significant between smokers and non-smokers, whereas the PD reduction was statistically significant.
All radiographic bone changes were found to be statistically different between the groups in ANCOVA (Figure 3).

Pre- and postoperative radiographs highlighting osseous regeneration at 12-month follow-up.
Discussion
The data presented here indicate that cigarette smoking is associated with an impaired healing response following GTR with PLGA/HA in conjunction with the rubber dam as a barrier. A rubber dam, a non-reabsorbing-type of barrier, was proposed in order to aid periodontal apparatus regeneration through the GTR technique. Our clinical results revealed a significant improvement of all clinical and radiographic parameters. Ethical reasons prevented us from obtaining a histological evaluation to validate a ‘true regeneration’. However, a careful examination of the periodontal parameters revealed similarities to those presented in many studies published in the past 20 years on GTR technique20,21 representing, therefore, our control for comparison. We certainly welcomed the advent of resorbable membranes that made an additional surgical procedure for membrane removal unnecessary. Comparing absorbable versus non-resorbable membranes, we found similar changes on periodontal parameters, such as CAL gain, and bone gain and PD reductions. 22 The use of a rubber dam as a barrier was first presented by Salama et al. 5 and Cortellini and Pini-Prato 19 who showed a significant CAL and bone gain in addition to a PD reduction; Paolantonio et al. 23 found similar results comparing the rubber dam with e-PTFE membrane. An animal study presented a histological evaluation of experimental periodontal defects treated with a Modified Widman Flap, copolymer membrane, e-PTFE membrane, and rubber dam showing a ‘true regeneration’ for both. 24 Slightly more tissue recession and alveolar crest resorption was constantly found in the rubber dam sites compared with the e-PTFE ones.
Overall, our clinical parameters were in line with those highlighted in the literature when adopting the rubber dam-based technique for periodontal regeneration.
Premature rubber dam exposure was noted in 100% of cases, as shown in other publications on rubber dam.5,23 Although the exposure rate was in the range of 50–80% 25 in non-resorbable membranes and 65% for resorbable membranes, this event does not seem to jeopardize the regenerative process. 26 Speculatively, the impermeability of the membrane may not allow an easy passage of bacteria to the subjacent newly forming tissue or a membrane colonization as notoriously occurs with the porous e-PTFE 27 or resorbable membranes, 25 resulting in infection and, in turn, a limited periodontal regeneration. In line with other publications,5,19,23 a possible ‘protective effect’ against bacteria might explain the positive outcomes, including an uneventful healing overall regardless of the membrane exposure. This issue needs further investigation to be clarified perhaps through in vitro studies.
In this study, different outcomes between smokers and non-smokers could be due to differences in defect characteristics at baseline as shown by Tonetti et al. 28 The depth of the intrabony component was the major determinant. 28 Preoperative PD positively correlated with the amount of CAL gain and bone formation, following GTR procedures in mandibular Class II furcation defects. 26 Furthermore, CAL gain was significantly related to preoperative PD. 29 Non-homogeneous PD baseline values were observed between the smoking and non-smoking groups. Deeper PD baselines were present in the non-smoking group, and this difference reached statistical significance. To avoid this potential bias, the ANCOVA corrected for the effect of the PD baseline. The analysis resulted in no statistical difference for CAL gain and ΔREC between non-smokers and smokers. Hence, it seems that the PD baseline could have a causative role for CAL gain values with respect to smoking. For PD reduction and other bone parameters, smoking became the most important factor affecting the periodontal healing response. Our findings are in line with considerable literature,6,27 highlighting the negative effects of smoking on bone metabolism. Some studies also found that cigarette smoking was associated with a reduced healing response after GTR treatment.29,30 After correcting for the oral hygiene level and the depth of the intrabony component, smoking was a significant factor for the clinical outcome. 6
It has been demonstrated that smoking impairs the healing outcome of GTR treatment of intrabony defects with bioresorbable membranes 12 months after surgery, 31 even if, conversely, it did not seem to influence the clinical outcomes achieved from 1 to 6–7 years from treatment. 32
Harris et al. found no difference in terms of CAL gain and the PD reduction in smokers versus non-smokers treated with enamel matrix protein, demineralized freeze dried bone allograft, and collagen membrane. 31
Our analysis seems to indicate that smoking itself significantly determined a patient’s healing response, even if the PD baseline values had a superior impact on affecting the CAL gain magnitude.
In conclusion, smoking, as shown in other publications, is confirmed as a detrimental factor to bone regeneration. Furthermore, since we found differences for PD values at baseline between groups, smoking does not seem to influence the outcomes achieved (CAL gain and ΔREC) 12 months post surgery in respect to PD baseline.
Based on our clinical observations and measurements and within the limitations of this study, due to a small sample size and the lack of histology and controls, PLGA/HA in conjunction with the rubber dam barrier could be used for treatment of periodontal intrabony defects. Major advantages of the rubber dam were related to a minimal cost, ease of handling and positioning, no need for stabilization while in place, easy removal, and virtually no significant postoperative sequelae if properly managed.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.