
Abstract
Anti-TNFα drugs have strongly changed the way in which we deal with moderate and severe psoriasis. However, it is debatable whether biological drugs could increase the risk of developing cancer. The correlation between anti-TNFα drugs and lymphomas is well-known and is reported in all the technical details of biologic drugs. However, the association between anti-TNFα agents and solid tumors is still controversial. The authors report a case of bilateral salivary gland tumor in a psoriatic patient treated with several immunosuppressive therapies including anti-TNFα inhibitors.
The use of anti-TNFα drugs for the treatment of psoriasis is increasing in medical practice. One of the most debated adverse effects of biological therapy with TNFα inhibitors is an increased risk of developing cancer, as reported in scientific journals, especially in patients suffering from chronic inflammatory diseases such as rheumatoid arthritis and inflammatory bowel diseases. For this reason, we deducted a higher tumor incidence also in psoriatic patients treated with anti- TNFα inibithors. 1 In fact, TNFα is a cytokine which plays a key role in the control of infections and tumors. The correlation between anti-TNFα drugs and lymphomas is evident and has been reported in all the technical details of biologic drugs. However, the association between anti-TNFα agents and solid tumors is still controversial. We report a case of bilateral salivary gland tumor in a psoriatic patient treated with etanercept.
Case report
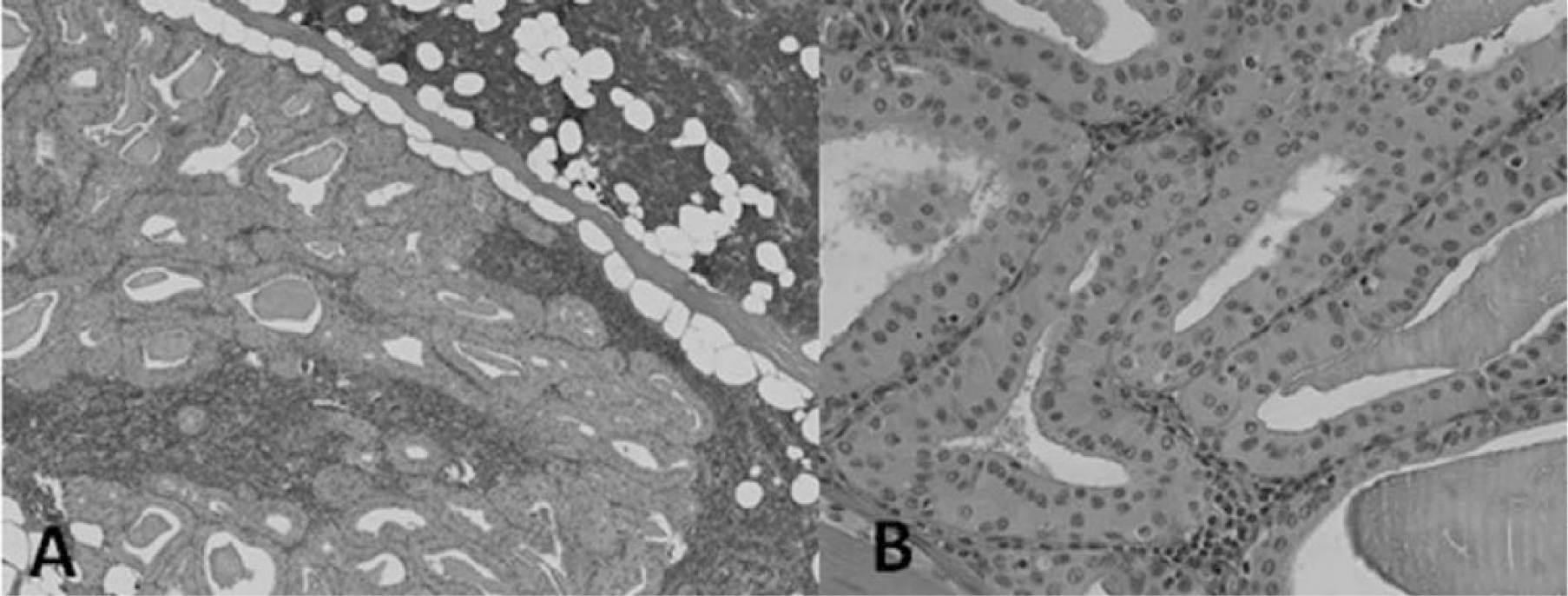
We report the case of a 59-year-old man affected by psoriasis since 1997. The patient had a history of smoking and suffered from hypertension. No malignancies were referred. The patient was treated for psoriasis with topical treatment until 2005 when his disease deteriorated, reaching a Psoriasis Area and Severity Index (PASI) of 15. 2 For this reason, Acitretin 0.5 mg/kg/daily was administered. After 6 months, because of a severe xerosis and scarce results (PASI 13), acitretin was interrupted. Hence, we carried out ordinary exams, and cyclosporine (CsA) was administered with a dose of 3 mg/kg/daily, reaching a PASI of 5. After 3 months, some blisters appeared on the patient’s arms and legs and, consequently, a biopsy was performed. Histology showed sub-epidermal blisters with eosinophylis and neutrophylis, direct immunofluorescence revealed linear deposits of IgGs, and indirect immunofluorescence revealed linear IgG at the dermo-epidermal junction (title 1/40). The classical clinical aspect of bullous pemphigoid (BP) and the immunofluorescence results confirmed the diagnosis of BP. CsA was interrupted and we began a combined therapy with prednisone (25 mg/daily tapering dose) and dapsone (100 mg/daily) until complete remission of the disease. As soon as prednisone was tapered, the psoriasis began to worsen (PASI 14). In 2007, we prescribed efalizumab 1 mg/kg/week and the patient achieved a complete resolution of the psoriatic plaques (PASI 0), maintained successfully for 2 years. During this therapy, no side effects were reported at the subsequent check-ups. In 2009, efalizumab was removed from the market and we switched to etanercept (ETN) 25 mg/twice a week. From 2009 until 2013, psoriasis was perfectly under control (PASI 0) and the patient was seen for follow-up visits once a month; all his blood tests were in the normal range and no side effects were reported. In September 2013, during a check-up, our patient indicated a lump on the right side of his jaw, which had grown during the previous 2 months. No increased cervical lymph nodes were found on palpation and an ultrasound exam was performed, revealing a cystic mass of 22.5 × 15.5 mm in size in the right side of the jaw. Subsequently, a computed tomography confirmed this cystic mass (Figure 1) but demonstrated another cystic lump. This new mass, smaller than the first one, was situated at the left side of the patient’s jaw. After these findings a fine needle aspiration cytology (FNAC) exam was performed on both parotids, revealing a bilateral Warthin tumor (WT). At this point, ETN treatment was interrupted, and the patient was put on a list for surgical removal of both tumors. The first mass found on the right side of the jaw was removed. Histologic examination of hematoxylin and eosin stained slides demonstrated a well circumscribed, thinly encapsulated cystic lesion filled with papillary projections of epithelial cells intimately associated with aggregates of lymphocytes. The papillae were composed of two layers of oncocytic cells; a luminal layer of tall columnar cells and an inner layer of cuboidal cells. These histologic characteristics confirmed the diagnosis of WT (Figure 2).

Computed tomography exam performed with contrast enhancement (Xenetix 350, Guerbet, Villlepinte, France) revealing cystic mass of 22.5 × 15.5 mm on the right side of the jaw.
(
Discussion
WT is a benign tumor characterized by an uncontrolled proliferation of the epithelial component of the salivary gland and the lymphoid stroma. It is the second most frequent benign cancer of salivary glands, and occurs in 2–6% of all parotid tumors. 3 It is commonly found in the lower pole of the parotid gland, and only 5–14% arise bilaterally. 4 This cancer is usually benign, and only 1% of WT undergoes a malignant transformation, which is rarely represented by non-Hodgkin lymphomas. 4 To date, only two cases of bilateral salivary gland tumor during anti-TNFα treatment have been reported. Both the patients had been suffering from psoriasis for a long time and had previously been treated with several systemic therapies. 5 For this reason the relationship between WT and anti- TNFα therapies is still unclear. In fact, biological drugs have been demonstrated to be associated with several adverse events which include infections (as the re-activation of tuberculosis), auto-immune disorders, hematological and neurological diseases, hepatotoxicity, and an enhanced risk of developing malignancies. 6 Concerning this last-mentioned adverse effect, scientific studies have not yet clarified the occurrence of cancers in patients treated with anti-TNFα agents.
On the one hand, a possible correlation between anti-TNFα drugs and lymphomas have been reported by several studies 7 and has been described in all the anti-TNFα drug technical details; on the other hand, Scott et al. reported that the overall risk of solid cancer is controversial: in fact, even though the only systematic review of randomized trials involving infliximab and adalimumab (but not etanercept) reported a dose-related increased risk of cancer, national registries have not yet found an increase in solid cancers after treatment with TNFα inhibitors. 8
With regard to our case, it is difficult to state whether WT had been induced by biological therapy or not, as WT seems to be extremely rare when occurring in both parotid glands (5–14%). 4 Furthermore, in this case, after the diagnosis of BP, our patient was treated with several immunosuppressive therapies including corticosteroids which could have influenced the occurrence of a bilateral WT. The patient was also a smoker and in medical studies the role of tobacco smoke has been described as an influencing factor by altering the reaction of the immune system thereby increasing the coexistence of WT. 9 Even though the relationship between anti-TNFα agents and WT is still unclear, we followed the consolidated international practice to stop administering biologic drugs in all patients with a solid tumor, even benign, in order to minimize a possible malignant transformation as can occur in WT.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.