
Abstract
In the realm of medical procedures for urinary obstructions, a distinct division of roles is evident: the vast majority of percutaneous nephrostomies (PCNs) are the domain of Interventional Radiology (IR), while the placement of double J stents (JJ stents) falls squarely under Urology. This division, however, is not without its complexities. When confronted with a patient suffering from a urinary obstruction, the decision-making process can become intricate. The underlying cause often fuels the debate: should IR intervene with a PCN, or should Urology place a JJ stent? Such decisions have profound implications for the individual patient.
In this comprehensive review, we aim to compare the utilization of PCN to that of JJS in a variety of clinical settings and evaluate their indications, relative efficacies, and potential complications to ascertain whether one procedure outperforms the other.
Introduction
Percutaneous nephrostomy (PCN) and Double-J stent (JJS) placements are both minimally invasive, image-guided urinary drainage procedures that are indicated for a range of uropathies, most commonly relief of obstructive uropathy, urinary diversion, and access for endourologic procedures. 1
PCN (Figure 1) is performed under both sonographic and fluoroscopy guidance. This procedure requires the patient to be in the prone position, and moderate sedation is needed. PCN placement is associated with a risk of hemorrhage, septicemia, urinary tract infection, and catheter dislodgement. 2 On the other hand, JJS placement (Figure 2) is performed concomitantly with cystoscopy for the visualization of the ureteral orifice. JJS placement can be done under local anesthesia, and the patient is usually in the supine position during the procedure. Early complications of JJS placement include irritative bladder symptoms, hematuria, and stent discomfort; meanwhile, stent migration, encrustation, and fragmentation are among the common complications in the late period. 3 Choice of technique may be influenced by the nature of each case, that is, complexity, local technical expertise, availability of medical equipment, and patient factors. There are no absolute contraindications to either procedure. However, PCN may be more favorable in patients with pathologic conditions of the bladder; meanwhile, JJS is preferred in morbidly obese patients and patients with nondilated renal collecting systems.1,4 Both procedures have advantages and disadvantages in regard to complications, costs, and post-operative management. Therefore, it is important to select the appropriate technique, as each has its own unique impact on the patients’ outcomes.
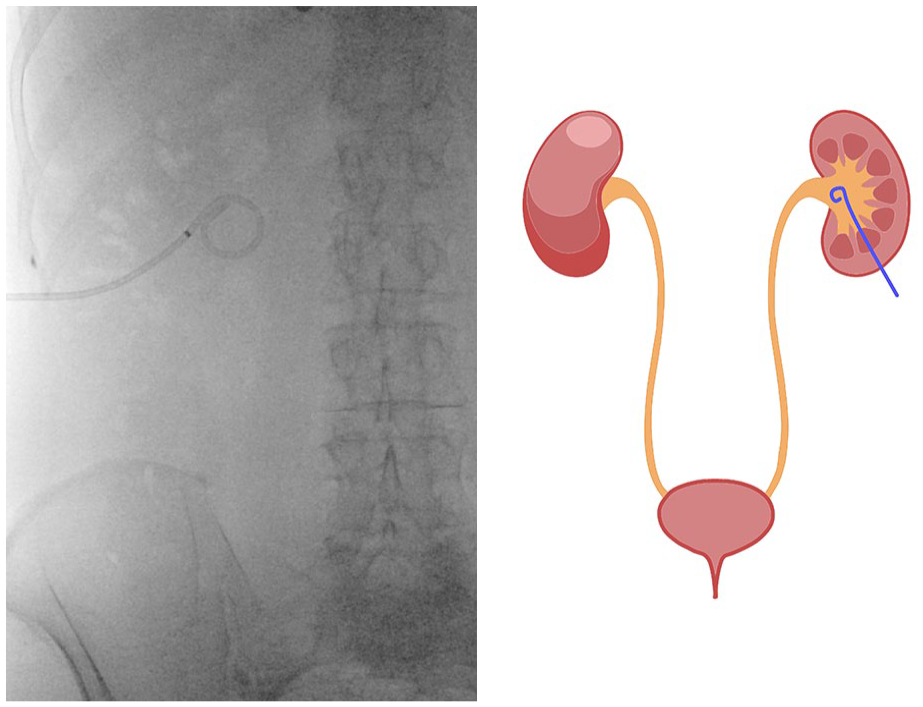
Diagram and fluoroscopy images of percutaneous nephrostomy (PCN) tube.
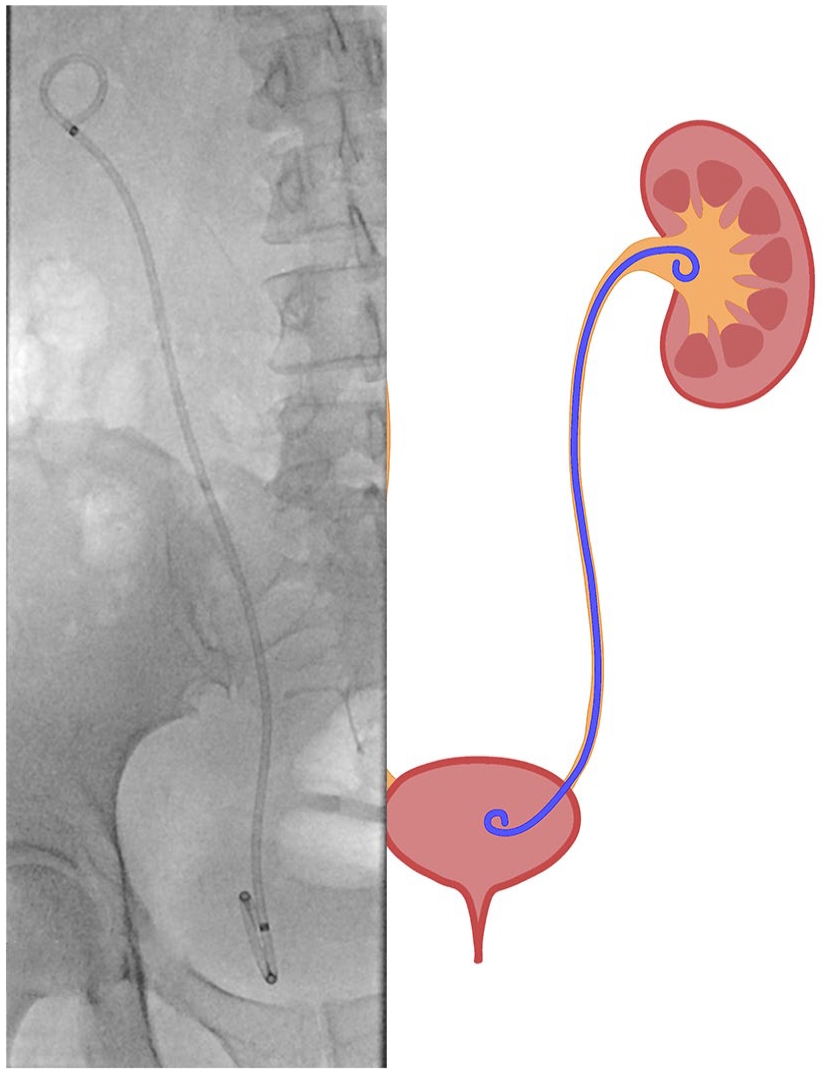
Diagram and fluoroscopy images of Nephroureteral/JJ stent tube.
In this comprehensive review, we aim to compare the utilization of PCN to that of JJS in a variety of clinical settings and evaluate their indications, relative efficacies, and potential complications to ascertain whether one procedure outperforms the other and suggest the most appropriate intervention.
Impacted ureteral stones
Impacted ureteral stones refer to stones that have remained in the same position for more than two months. When associated with hydronephrosis, impacted stones are the most difficult stones to remove with flexible ureterorenoscopy (f-URS) due to ureteral impaction, polyps, and strictures, which may increase the risk of ureteral injury.
Adjunctive PCN may have the advantage of straightening a flexed ureter by elevating the kidney after hydronephrosis is decompressed. It allows for efficient irrigation and a clear view of the surgical field, potentially improving stone-free rates. The PCN may help relieve intrarenal pressure when stones are pushed back into the renal pelvis or penetrated. 5 According to a clinical report of 2650 patients who underwent ureteroscopic treatment for impacted stones, ureteral injury, ureteral stenosis, postoperative fever, postoperative hydronephrosis, and hospitalization were not significantly different with or without preoperative PCN. 6
Malignancy
Malignant ureteral obstruction (MUO) is one of the most common complications of advanced malignancies. Among the two discussed techniques, JJS placement is less invasive, less painful, and has a lower risk of bleeding compared to the PCN placement. 7 PCN tube also tends to diminish the patient’s quality of life (QoL) due to the requirement of external drainage with a nephrostomy catheter and the need of frequent exchange. For instance, Zhang et al. stated that PCN patients experienced significantly more difficulties in self-care compared to JJS patients. 8 A similar result on the quality of life was demonstrated in Gauhar et al. 9 Shvero et al. also reported 84% of patients who have experience with both types of urinary drainage preferred JJS. 10 Moreover, the phenomenon of metastatic seeding along the nephrostomy catheter tract has been increasingly reported in the literature as the cause of death in patients undergoing PCN placement as the treatment of obstructive uropathy secondary to advanced cancer.11–13 In our opinion, JJS stent is a more favorable option and should be offered as the initial treatment of MUO. However, when a stent cannot be placed, particularly in cases with evidence of bladder invasion or anatomically altered bladder trigone or ureteral orifices, we recognize that percutaneous nephrostomy tube placement is a better alternative approach to divert urinary flow and relieve the symptoms resulting from the obstruction.
Emphysematous pyelonephritis
Emphysematous pyelonephritis (EPN) is a rare but potentially life-threatening infection characterized by gas-forming bacteria within the renal parenchyma or perinephric tissue. The overall mortality rate ranges from 6.7% to over 50% depending on the stage15,16 and is most related to septic complications. In their review, Huang and Tseng used the following criteria for EPN 17 :
Class I: Gas in collecting system only (Emphysematous Pyelitis)
Class II: Parenchymal gas only
Class IIIA: Extension of gas into peri-nephric space
Class IIIB: Extension of gas into pararenal space
Class IV: EPN in solitary kidney or bilateral disease.
JJ stenting is preferred in class I EPN cases,18–20 where the renal function is relatively preserved, and the urine can drain through the ureter. Das et al. found that patients who underwent JJ stenting for treatment of EPN had similar outcomes to those who underwent PCN. 18 Elbaset et al. noted, however, that management of EPN with JJ stenting compared to PCN was correlated with a significantly shorter hospital admission length and a higher leukocytic count decrease by discharge. 19 Additionally, El-Nahas et al. found that management with JJ stenting as opposed to PCN resulted in greater preservation of kidney function in the affected kidney. 20
On the other hand, existing literature for managing higher grade EPN (II and above), where renal function is usually compromised and urine cannot drain through the ureter, is less clear. In a 12-year review, Storey et al. reported that PCN was associated with better outcomes in EPN class 2 and above.16,21 PCN is also preferred in cases where there is an extensive collection of pus, which cannot be drained through JJ stenting. A subgroup analysis of patients found a statistically significant difference (p = 0.035) in favor of PCN in more severe EPN. 21
Xanthogranulomatous pyelonephritis (XGP)
XGP is a rare chronic bacterial renal infection. This condition is typically characterized by obstructive nephrolithiasis coupled with granulomatous inflammation, resulting in an enlarged, nonfunctional, hydronephrotic kidney with diffuse parenchymal destruction. 22 In the study by Xie et al. Longer draining of large obstructions for effective antibiotic therapy was recommended to facilitate surgery. 23 Furthermore, Kuo et al. advocated preoperative drainage to achieve a cleaner surgical field, improve safety, and reduce postoperative complications. 24
DIC/coagulopathy
JJS placement is a more favorable option for these patients since it carries a lower risk of bleeding compared to PCN placement. In cases where PCN must be performed, coagulopathy must be corrected prior to the procedure to prevent adverse consequences resulting from excessive blood loss.
Pregnancy
During pregnancy, both JJ-stent and PCN are equally effective and safe for relieving renal colic when conservative treatment has been unsuccessful, but complications and invasiveness of both must be considered. According to Mason et al., 25 when compared to PCN, JJ-stenting has been associated with a significantly decreased rate of subsequent urinary tract infection or pyelonephritis, and repeat exchange procedures within 6 months of their initial procedure, but there were no notable variations in the risk of preterm labor or delivery, regular vaginal delivery, typical cesarean section, early labor leading to delivery, premature rupture of membranes, false labor before and after 37 weeks, or intrauterine infection. In pregnancy, PCN is relatively uncommon and usually reserved for severe cases where there is significant obstruction or infection that cannot be managed conservatively. In a study by Khoo et al., 26 the percutaneous nature of PCNs had been linked to elevated incidences of septic complications (bacteriuria and pyelonephritis), bleeding as well as discomfort and social impact arising from the presence of an external device.
In addition, radiation exposure to the fetus is an important consideration. Therefore, exposure should be minimized by careful collimation over the area of interest during fluoroscopy and lead shielding of the maternal abdomen. In situations where the placement of a ureteral stent is needed, this procedure can be performed through ureteroscopy, and the precise positioning of the stent can be verified using ultrasonography, thereby eliminating radiation risk.
Large stones/hydronephrosis
PCN is commonly used for large kidney stones that are difficult to manage with less invasive techniques. It allows for subsequent interventions such as percutaneous nephrolithotomy (PNL), which is the recommended treatment for large kidney stones of 20 mm or more. 27 Ureteroscope (URS) is effective for multiple stones, but limited by stone size, burden, and the presence of impacted stones, particularly suitable for patients with a stone burden smaller than 20 mm. 27
There are limited instances in the medical literature that discuss the application of PCN for intricate renal stones (those occupying a majority of the major calyces in at least 80% of the renal collecting system). Few reports have highlighted the challenges associated with using PCN for complex renal stones, indicating a technical success rate of 82% to 85%, in contrast to 96% to 100% for cases involving an enlarged renal system. 28
Regarding ureteric stone location, a study published in the International Journal of Urology found that JJ stent placement failure, mucosal injury, and ureteral perforation were more frequent in patients with upper ureteric stones larger than 1.5 cm. The study suggested that the PCN tube for PNL was more successful for proximal ureteral stones larger than 1.5 cm, while URS and JJ-stenting were effective for distal and mid-ureteral stones < 1.5 cm. 29
In a study by Mokhmalji et al., 30 PCN was found to be more effective than JJ-stenting in diverting hydronephrosis caused by stones, especially in patients with a fever, as well as in males and juveniles. PCN had a 100% success rate, while JJ-stenting had an 80% success rate, with the failed cases requiring conversion to PCN due to factors such as high ureteral stones, extent of obstruction, or ureteral kinking.
Staghorn stones without hydronephrosis
Staghorn stones, also known as struvite stones, are large kidney stones that branch out and fill the renal pelvis and multiple calyces of the kidney. They are often associated with recurrent urinary tract infections caused by bacteria like Proteus, Klebsiella, and Pseudomonas. If left untreated, these stones can grow rapidly and cause significant obstruction and damage to the kidney. They have a high risk of complications, including recurrent infections, renal impairment, and potential loss of kidney function. 31
The management of staghorn stones usually involves a combination of medical therapy and surgical intervention. Percutaneous nephrolithotomy (PNL) is recommended as the primary treatment for struvite staghorn stones. PCN can effectively provide drainage and facilitate subsequent interventions like PNL for stone removal. PCN enables direct visualization and removal of stones from the kidney, but it may be challenging to perform without hydronephrosis. Alternative technique such as ureterscopy-assisted retrograde nephrostomy (UARN), ultrasound- and flouroscopy-guided PCN, and double-puncture technique with air or carbon dioxide distension have shown effictiveness in accessing collection system with staghorn calculus and no hydronephrosis.
PCN placement for future lithotripsy
The most common approach in PCN is to directly access the desired calyx. However, if the stone is large, limited space in the calyx can pose challenges for accommodating the Amplatz sheath and nephroscope, potentially affecting the effectiveness of stone removal.
Performing PCN for an upper calyceal stone through lower calyx access, specifically in the supine position, has been found to be a safe technique with higher success rates in reaching the stone and achieving a stone-free status. 32 However, the upper pole calyceal access remains relatively riskier when compared to the lower pole access for PCN. A study by Tefekli et al. revealed that upper pole access group experienced significantly longer operative times, a higher incidence of overall complications, lower rates of achieving a stone-free status, and extended mean hospital stays. 33 A newer alternative technique allows accessing the lower calyx in a supine position, offering improved accessibility and maneuverability due to anatomical differences compared to the prone position, further enhancing the safety of lower pole access. 34
High BMI
Bayne et al. found that the mean BMI for patients with nephrostomy tube dislodgement was significantly higher compared to the mean BMI of those without tube dislodgement (p < 0.0001), and the likelihood of tube dislodgment increased by 6% for each unit of increase in BMI. 35 Wynberg et al. showed that there was a positive correlation between BMI and nephrostomy tube creation time. The study also reported high procedure failure rate was associated with a BMI greater than 40 kg/m2, and the PCN placement procedure became more difficult as the BMI increased. Since the increased subcutaneous fat in morbidly obese patients may deflect the wire, patients with a BMI above 40 kg/m2 may require an alternative option as the risk of developing procedure-associated complications may outweigh the benefits. 36 On the other hand, no articles have been reported regarding the specific BMI thresholds for double J-stent placement.
Quality of life, Cost & patient preference
Although the choice to treat patients with stenting or PCN is based upon medical expertise, patients must be involved in treatment decisions that affect their quality of life and be informed of expected post-procedural outcomes.
PCN has a shorter procedural time than JJ stenting and requires conscious sedation and local anesthesia. This is appealing to many patients who are unable to tolerate general anesthesia. Post-procedural pain and need for analgesics in the immediate recovery period have been shown to be comparable between patients undergoing JJS and PCN, and both sets of patients show clinical improvement at similar rates.37,38
In a meta-analysis of 10 studies reporting outcomes in patients with malignant ureteral obstruction (140 patients with stents and 135 with PCN), stents were preferred because of easier maintenance but PCN was a safe alternative if the malignant obstruction prevented stent placement. 9
Both stenting and PCN can cause urinary symptoms such as dysuria and hematuria in the immediate recovery period. However, these symptoms are much more common after JJ stents than PCN and persist for significantly longer. Weltings et al. found that almost 80% of JJ patients report dysuria, whereas only 17% of PCN patients face this problem. 39 Prolonged urinary symptoms after JJ stenting are the most common complaint from the procedure, significantly impacting the quality of life for many patients.30,40 In a study of 18 patients who underwent PCN, de Sousa Morais et al. reported that 28% of patients reported bag leak/slippage, 22% had problems with bag management and 22% reported unpleasant smell. 41
Evidence in support of one technique over the other is mixed in the setting of malignant obstruction. PCN patients report higher dissatisfaction with impaired mobility and personal hygiene due to the necessary collecting bag. De Sousa Morais et al. report that approximately a quarter of patients with PCN face problems such as collecting bag management difficulties and smell, though these symptoms typically resolve to a clinically insignificant level within a few weeks of the procedure. 41 Of consideration, women are more likely than men to report worse mobility and personal hygiene after PCN.
In addition, there are higher rates of depression in JJ stent patients. This is due to the prolonged urinary symptoms reported by many patients. Overall, quality of life tends to be higher after PCN than JJS because symptoms improve faster and more reliably.41–43 Given the varying impacts on quality of life, including prolonged uninary symptoms with JJ stent and mobility or hygiene challenges with PCN, the choice between these interventions should be guided by both clinical factors and patient preferences.
Regarding the cost, on a per-procedure basis, 2023 Medicare facility and physician fees for JJ stenting (Code 52332) is $329 at an ambulatory surgery center and $671 at a hospital outpatient department, whereas PCN (Code 50432) is $209 at an ambulatory surgery center and $410 at a hospital outpatient department However, both pathways can be more costly when complications ensue due to repeated procedures, leading to decreased patient satisfaction.
When to exchange
Currently, there are no evidence-based guidelines for PCN exchange frequency, and current recommendations are based on expert opinion. During the treatment of obstructive nephropathy with PCN, crust formation in the PCN can result in chronic obstruction. 44 Therefore, it is recommended to change the PCN on a regular basis (every 3–4 months) to prevent chronic obstruction. 45
Current guidelines from the Infectious Diseases Society of America (IDSA) have not included percutaneous nephrostomy catheter-related infections due to a lack of robust evidence. 46 An empirical antibiotic regimen should be initiated, preferably following the collection of blood and urine cultures by the PCN and should not be withheld if the specimen collection is delayed. If the initial urine culture is positive, catheter exchange is recommended to be performed within 1–4 days. 47 At least one dose of concordant antibiotics must have been administered to the patient prior to exchange. Antimicrobial coverage must be continued for a total course of 10–14 days. 47 If urine cultures from PCN reveal bacterial growth despite no clinical evidence of infection, antibiotic treatment, and catheter exchange are not recommended, as PCN colonization would be inevitable.47,48
In cases of catheter dislodgement or kinking, catheter exchange should be performed as soon as possible to maintain tract patency. 49 If the tube is not replaced within 48–72 h, subsequent catheterization of the tract could be a challenge. 50
Conclusion
In essence, while both nephrostomy and nephroureteral stenting have their specific clinical indications, the choice often hinges on the unique clinical scenario and patient factors (Table 1).
Summary of best indication for nephrostomy versus nephroureteral catheter.
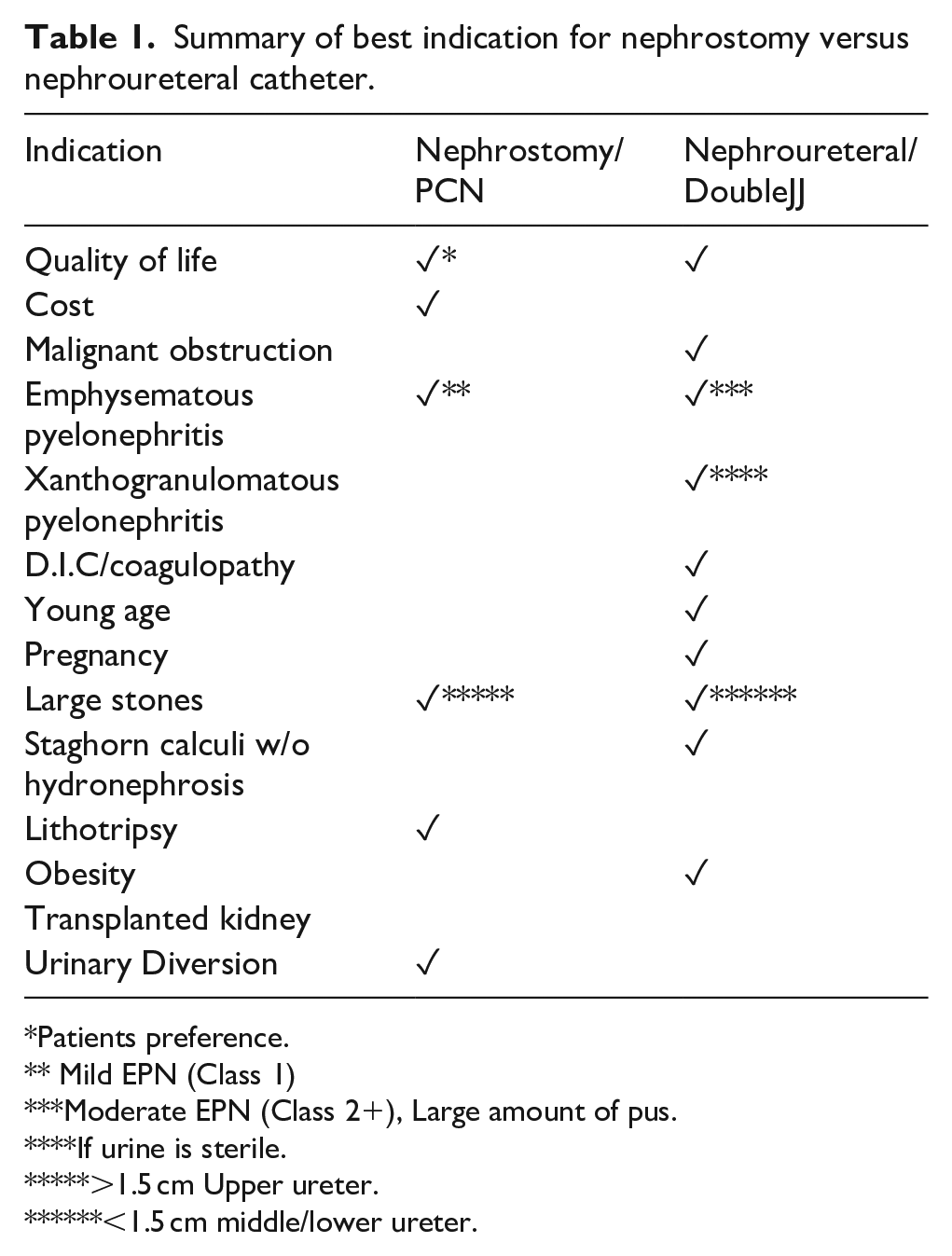
Patients preference.
Mild EPN (Class 1)
Moderate EPN (Class 2+), Large amount of pus.
If urine is sterile.
>1.5 cm Upper ureter.
<1.5 cm middle/lower ureter.
1. PCN catheter is recommended for Stones > 1.5 cm in the proximal ureter, Staghorn calculi with hydronephrosis, xanthogranulomatous pyelonephritis, urinary diversion, and large stone for future lithotripsy.
2. Double JJ stent is better for the malignant obstructions, disseminated intravascular coagulation (DIC)/coagulopathy, pregnancy, staghorn calculi without hydronephrosis, obesity (specially BMI of >40) and stones smaller than 1.5 cm in the mid and lower ureter.
3. Both methods have their indications for treating emphysematous pyelonephritis: Double JJ stent is preferred for mild EPN (Class 1), while the PCN stent is chosen for moderate EPN (Class 2+) as well as large amount of pus that cannot be drained with double JJ.
Footnotes
Acknowledgements
None.
CRediT Authorship statement
MGR: Conceptualization, Writing - Review & Editing, Supervision, Project administration
KT: Investigation, Writing - Original Draft, Review & Editing, Visualization
DW, MA, MHS and OG: Investigation, Writing - Original Draft, Review & Editing
AB, SR, DL: Methodology, Writing - Original Draft, Review & Editing
All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Not applicable.
Data availability statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.