
Abstract
Objectives:
To assess disobstructive proficiency of BPH3 trifecta in RASP according to different techniques.
Methods:
Baseline prostate volume (PV), uroflowmetry parameters and Validated questionnaires: IIEF, Incontinence severity index score (ISI), International prostatic symptoms score (IPSS), MSHQ, Quality of recovery (QOR), were recorded preoperatively and 12 months postoperatively. RASP was conducted using both the urethra-sparing (Madigan) technique and a non-urethral-sparing transvesical (Freyer) approach. Two groups were evaluated for achievement rates in terms of BPH-3 and BPH-6. BPH-3 was defined by a combination of: a reduction of ⩾30% in IPSS compared to baseline, ISI score ⩽ 4, and absence of complications beyond Clavien grade 1.
Results:
About 158 patients underwent RASP, with 93 undergoing the Madigan procedure and 65 the Freyer approach. Patients in the Madigan group were younger, with lower PV, baseline IPSS score, overactive symptoms (ISI score), but higher MSHQ and IIEF score, when compared to the Freyer population (all p < 0.02). At 12-month follow-up, patients who underwent the Madigan procedure reported shorter bladder irrigation time and time to catheter removal (both p < 0.001). As expected, Madigan patients also demonstrated superior postoperative IIEF and MSHQ scores (all p < 0.001). Postoperative complication incidence was higher in the Madigan cohort, mainly due to UTI (p < 0.001). Although there were no differences in postoperative IPSS and Q-max between groups, the Madigan cohort presented with higher post void residue (p < 0.001). BPH6 achievement was higher in the Madigan cohort (48% vs 28%) (p < 0.001), while no difference was observed in BPH3 achievement rate.
Conclusion:
The BPH3 composite trifecta appears to be more suitable than BPH6 in assessing the proficiency in disobstructive symptoms relief after RASP.
Keywords
Introduction
Benign prostatic obstruction (BPO), is the most common cause of lower urinary tract symptoms (LUTS), affecting adult men. 1 Surgical treatment is a valid option when pharmacological therapy fails, with this regards, prostate volume (PV) represents an important parameter to establish the most appropriate treatment option among several techniques available, which can vary from endoscopic approaches to laparoscopic or robot assisted approaches. 1 Uroflowmetry and validated questionnaires are usually adopted to estimate pre-operative symptoms’ severity and post-operative functional outcomes. For large prostates (PV ⩾ 80 g), the EAU guidelines recommend enucleative techniques with lasers or bipolar energy, such as HoLEP, ThulEP, BipEP. 2 With the advent of robotic surgery, Simple Prostatectomy with a minimally-invasive approach gained popularity.3–5 Few randomized studies proved the non-inferiority of Robotic-assisted simple prostatectomy (RASP) to other enucleative techniques. 6
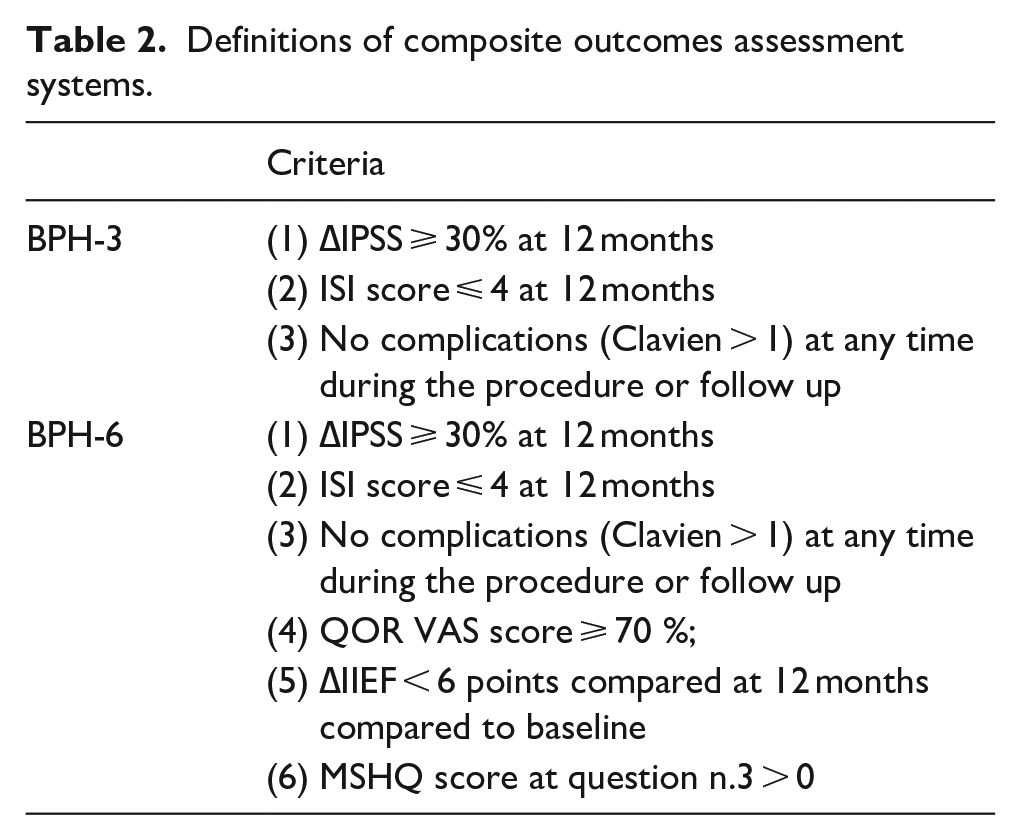
To date, the BPH-6 is the only composite outcomes scoring system available to evaluate efficacy, safety and patients’ satisfaction after surgery. 7 Notably the BPH6 includes: (1) Reduction of ⩾30% in IPSS at 12 months compared to baseline; (2) Incontinence severity index (ISI) score of ⩽4 points at all follow-up; (3) Quality of recovery (QoR) VAS score ⩾ 70; (4) Reduction of <6 points for International Index of Erectile Function (IIEF) score compared to baseline during follow-up; (5) Response to Male Sexual Health Questionnaire (MSHQ) score at question n.3 > 0 (indicating ejaculatory function preservation); (6) No treatment-related adverse event greater than grade I on the Clavien-Dindo classification system at any time during the procedure or follow up. In turns, the surgical procedure performed, can achieve the BPH6 only if is successful in preserving sexual functions.
Autorino et al. 4 proposed a Trifecta to assess peri-operative outcomes, which included: International Prostate Symptom Score (IPSS) < 8, urolowmetry assessed Q-max > 15 ml/s, and no perioperative complications. However, the above composite trifecta scoring system, doesn’t take in account the individual improvement in obstructive symptoms’ relief provided by the surgical procedure, but instead, it shows only if certain thresholds are reached, regardless of how severe was the baseline score. To overcome the above mentioned biases, we introduced a novel composite Trifecta outcome (BPH3) and compared its achievement rate to that of BPH6, in patients who underwent RASP for BPO.
Materials and methods
The Internal Review Board (IRB) approved database of patients that underwent surgery for BPO (Registration number 1722/22), was retrospectively queried for patients who presented with a PV ⩾ 80 g at the time of treatment. All the patients suitable for surgery, presenting with LUTS/BPO and large prostates (⩾80 g), refractory to medical therapy or associated with urinary retention, recurrent urinary tract infections, secondary renal function impairment, were offered RASP according to different techniques (urethra-sparing vs non-urethra-sparing). Exclusion criteria were defined as: patients with a history of prostatic or bladder cancer, neurological disease, urethral stricture, and a prostate volume <80 cc. Surgical techniques are described in Table 1. Surgeries were performed by the same experienced surgeon, with a Da Vinci Xi Surgical System (intuitive Surgical, Sunnyvale, CA, USA), via a trans-peritoneal approach, according to the previously published techniques. 8 Patients presenting with a prostatic median lobe indenting the bladder neck, or with coexistent bladder diverticula and/or stone underwent RASP according to the non-urethra-sparing trans-vesical (Freyer) approach. Young and sexually active patients without a prostatic median lobe, underwent RASP according to the urethra-sparing trans-capsular (Madigan) technique.
Minimal invasive simple prostatectomy surgical techniques performed.
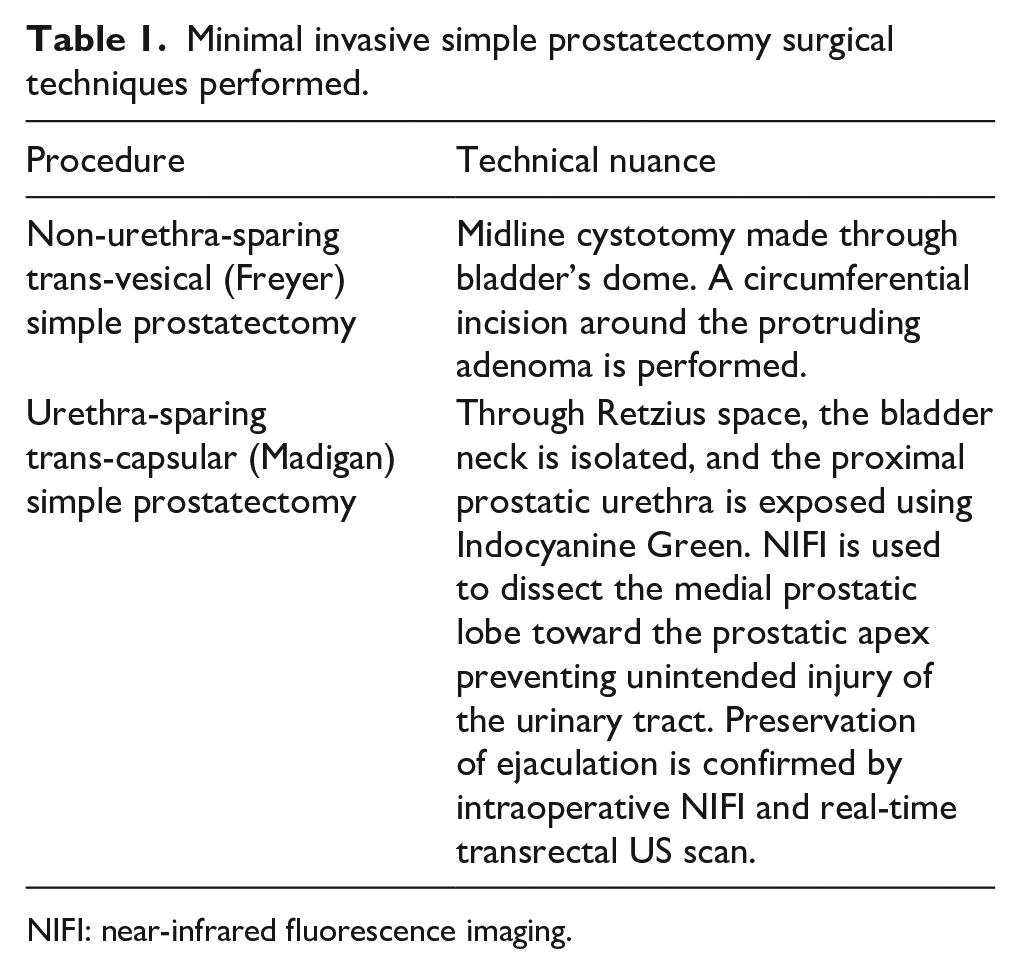
NIFI: near-infrared fluorescence imaging.
Prospectively collected clinical data included BMI, age, American Society of Anesthesiology classification status, International Prostate Symptom Score (IPSS), quality of life (QoL), Incontinence severity index (ISI) score, Male Sexual Health Questionnaire (MSHQ), International Index of Erectile Function (IIEF) score, Overactive bladder questionnaire (OABQ), and prostatic volume (PV). PV was measured by transrectal ultrasound, using the ellipsoid formula: height × width × length of the prostate × 0.523. Intra-operative blood loss was recorded from the suction canisters at the end of the procedure. Perioperative complications were graded according to the Clavien classification system. The IIEF, ISI, IPSS, QoL score, MSHQ, were administered to every patient during yearly follow-up, as well as uroflowmetry assessed Q-max and Quality of recovery (QOR) VAS scale. Composite BPH-6 and BPH-3 definitions are described in Table 2.
Definitions of composite outcomes assessment systems.
The study population was split into two subgroups based on the surgical approach and patients’ baseline features were compared: χ2 and Student t-tests were used for categorical and continuous variables, p < 0.05 was considered statistically significant. Statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS®, IBM, version 24).
Results
A total of 158 patients were included in the analysis: 93 patients underwent RASP according to Madigan technique and 65 patients underwent RASP according to Freyer technique. Baseline features and demographics are shown in Table 3. Median age was 68 years; however, patients were older in the Freyer group (p = 0.02). Patients scheduled for Madigan technique had a median baseline IIEF score of 20 points versus 17 and a median MSHQ of 21 versus 10, respectively (all p < 0.001). Baseline median IPSS score was lower in the Madigan group: 21 versus 24 points in the Freyer group (p = 0.04). Median Prostate volume was higher in the Freyer cohort as compared to Madigan cohort: 140 g versus 100 g (p < 0.001). Peri-operative and 12 months functional outcomes are reported in Table 4.
Baseline and demographics.
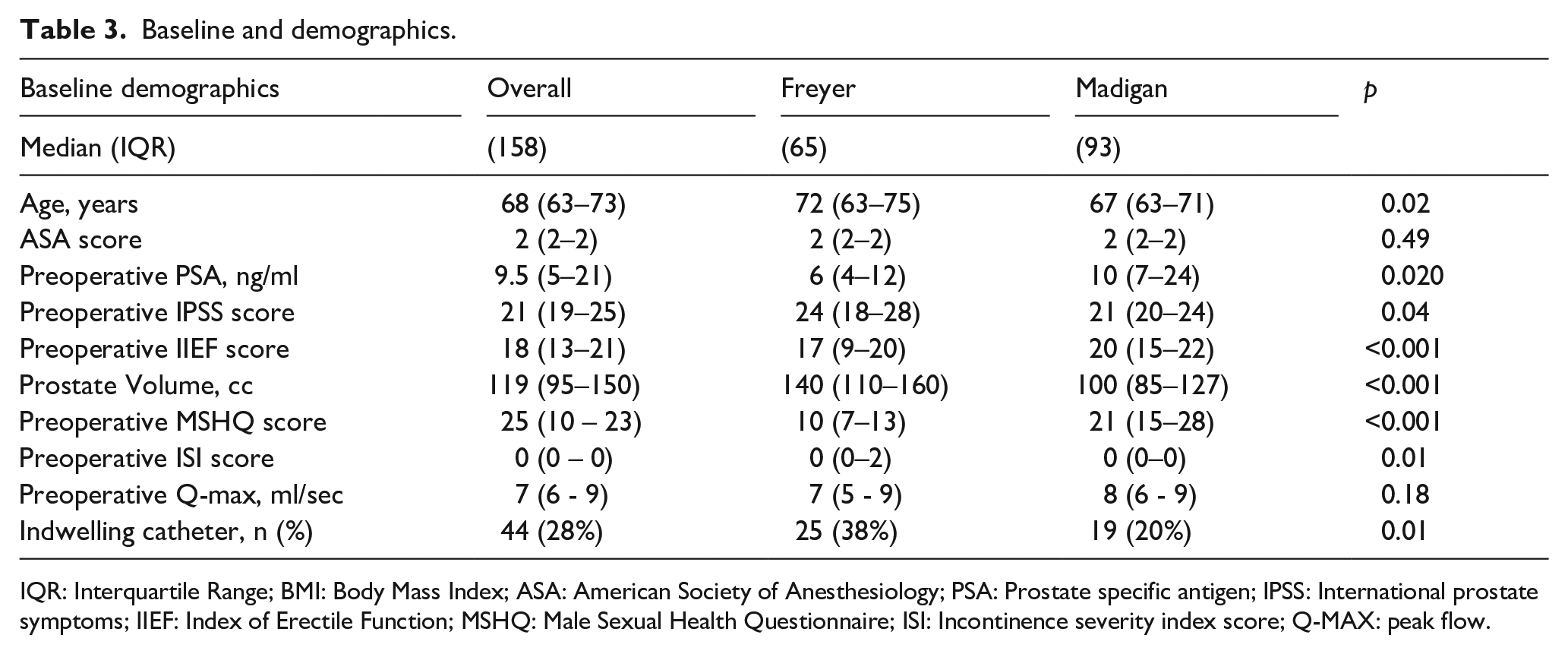
IQR: Interquartile Range; BMI: Body Mass Index; ASA: American Society of Anesthesiology; PSA: Prostate specific antigen; IPSS: International prostate symptoms; IIEF: Index of Erectile Function; MSHQ: Male Sexual Health Questionnaire; ISI: Incontinence severity index score; Q-MAX: peak flow.
Perioperative and 12-month functional outcomes comparison.
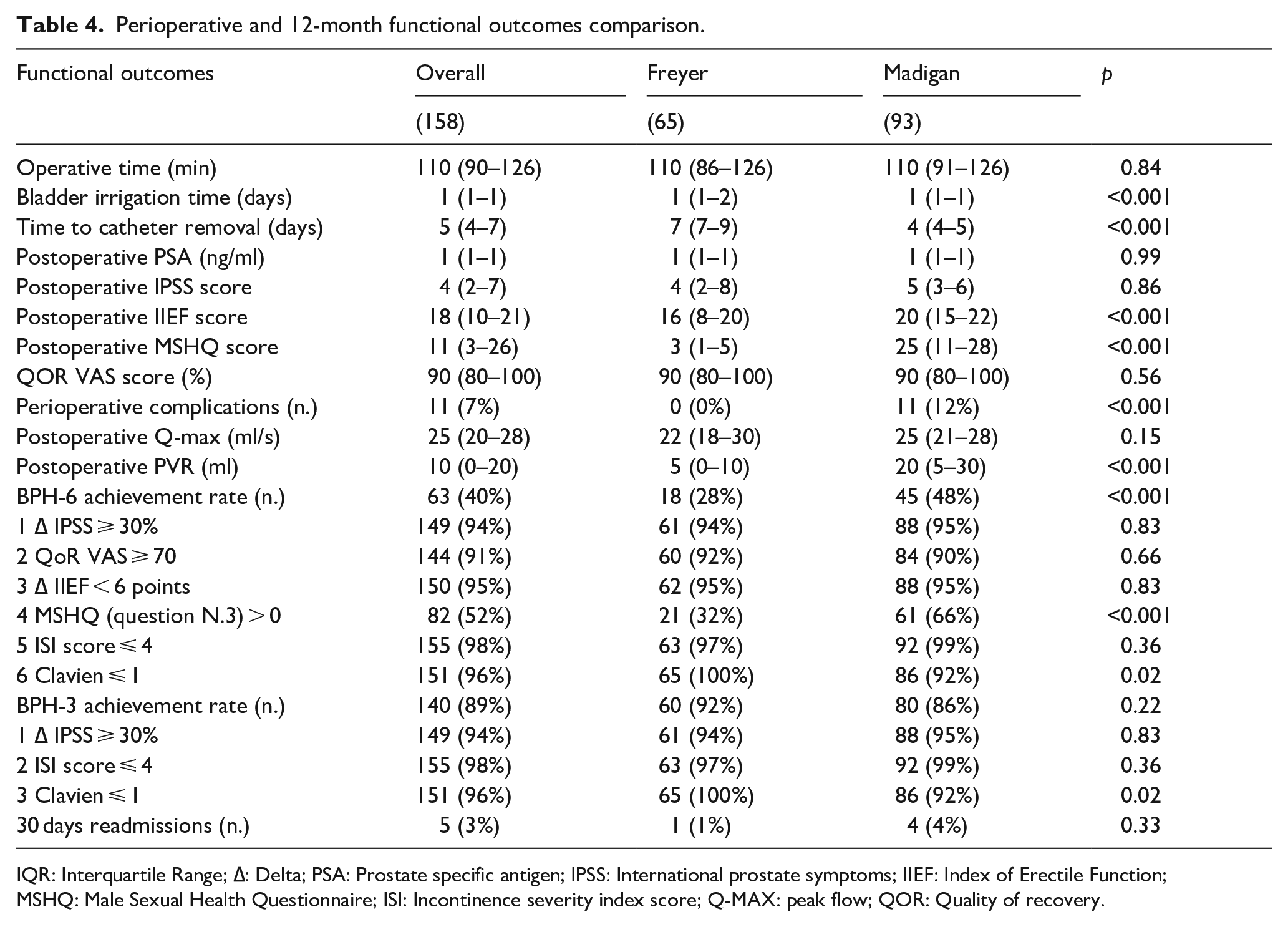
IQR: Interquartile Range; ∆: Delta; PSA: Prostate specific antigen; IPSS: International prostate symptoms; IIEF: Index of Erectile Function; MSHQ: Male Sexual Health Questionnaire; ISI: Incontinence severity index score; Q-MAX: peak flow; QOR: Quality of recovery.
Operative time was comparable between groups. Freyer patients had longer median catheterization time: 7 versus 4 days (p < 0.001). At 12 months follow-up, no significative differences were observed in terms of median Qmax and ∆IPSS between the two groups. Postoperative complication incidence was higher in the Madigan cohort, mainly due to UTI (p < 0.001). Moreover, no significative differences were found in ISI score at 12 months, which was ⩽ 4 in the majority of patients. As expected, patients in the Madigan cohort reported a better sexual function at 12 months: median MSHQ score was 21 in the Madigan cohort versus 10 points in Freyer cohort, and median IIEF score was 20 in the Madigan cohort versus 17 points in the Freyer cohort (all p < 0.001). No differences in postoperative IPSS and Q-max were found between groups, nonetheless, the Madigan cohort presented higher median post void residue 20 ml versus 5 ml (p < 0.001). BPH6 achievement rate was higher in the Madigan cohort (48% vs 28%) (p < 0.001), while no difference was found in BPH3 achievement rate.
Discussion
Since its first appearance in 2008, 9 robot-assisted simple prostatectomy has emerged as a viable treatment option for enlarged prostates. The widespread adoption of robotic technologies, including systems other than DaVinci, 10 has led to a significant increase in the use of this technique. This approach has demonstrated significant advantages, such as a shorter hospital stay and reduced estimated blood loss when compared to other enucleative techniques like HoLEP, ThuLEP and particularly to open ATV. 11
Despite good outcomes in the achievement of better flow, with a mean gain of Qmax at uroflowmetry of 2.47 ml/s, RASP, like other enucleative techniques, shares the side effect of retrograde ejaculation, which can represent a significant problem for many patients, especially for those sexually active. The only technique today which can avoid this issue is the adenomectomy,12,13 with a 65% probability of preserving antegrade ejaculation. 8
We previously reported that no differences were observed between different RASP techniques in terms of symptom relief, postoperative complications, or hospital stay. However, significant differences were observed in IIEF and MSHQ scores, favoring the Madigan Approach. 14 This data consistent with the current study, as no significant differences were observed between groups in both ∆ IPSS achievement (94% vs 95%) and postoperative Qmax (Table 4).
The uroflowmetry is historically the exam used both to determine the degree of obstruction and postoperative, the relief of symptoms. The association with validated questionnaires is strongly recommended by EAU guidelines.2,4 In this scenario, the BPH-6 serves as a comprehensive scoring system which investigates various aspects of LUTS, beyond those evaluated in the IPSS, namely, symptom relief, continence (ISI score), recovery after anesthesia (QoR VAS), postoperative complications (Clavien), ejaculatory function preservation, and sexual satisfaction (IIEF and MSHQ).
It is not surprising that in this study we obtained a higher BPH-6 achievement rate in Madigan cohort (48% vs 28%). Unlikely, when treating large prostates, few techniques are efficient in preserving the antegrade ejaculation, so, in our opinion, rely on BPH-6 score for the evaluation of postoperative results, may divert the attention from the primary problem which is the BPO.
Several efforts have been made to propose a practical tool to objectively measure a comprehensive metric to assess outcomes and QoL following prostate surgery. Different components for defining the trifecta have been proposed, that is, Q-max > 15 ml/s, IPSS < 8 pts. and absence of complications.4,11,15,16 In this study, the trifecta was proposed as a combination of ∆ IPSS ⩾ 30%, ISI score ⩽ 4 pts. And a Clavien ⩽ 1.
A study performed by Pavan et al. 15 analyzed trifecta outcomes according to a combination of IPSS score < 8, Qmax > 15 ml/s and no perioperative complications when comparing laparoscopic simple prostatectomy versus robot-assisted simple prostatectomy. They reported that age and BMI (p = 0.03) were factors associated with a likelihood of achieving the trifecta, showing that the procedure did not affect the outcome.
In another study by Zarraonandia-Andraca, 17 trifecta outcomes were analyzed in simple prostatectomy with parameters including, (1) no perioperative complications, (2) Postoperative IPSS < 8 pts., and (3) Postoperative Qmax > 15 ml/s. Results showed that 68% of patients achieved complete trifecta outcomes, however, it is important to note that this study only followed patients for 3 months. Additionally, one of our studies, which defined these same trifecta outcomes and compared them to HoLEP, showed a 56% success rate for RASP compared to 33% of HoLEP. 11
The robotic approach allows surgeons to follow the principles open prostatectomy while translating them into an endocorporeal, minimally-invasive procedure. This technique allows for a more precise enucleation, offering mayor visualization and detail of the prostate and prostatic urethra anatomy. These advantages allow a superior manual control and reduction of complications. 18 Despite the advancement made by other laser enucleation techniques in benign prostate surgery, there are still some drawbacks that need to be addressed. These include a steep learning curve, irritative voiding symptoms, urethral stenosis and the rate of incontinence.19–21
In our proposed definition of the Trifecta, the incorporation of the ISI score as an objective measure of continence in RASP holds significant importance. Incontinence is a common adverse outcome following prostatectomy, significantly affecting patient’s QoL. 22 In a study performed by Talamini et al., 3 RASP was superior to ThuLEP when assessing postoperative stress urinary incontinence (SUI) with rates of 18.8% versus 0% (p = 0.008). Furthermore, incontinence rates after HoLEP have been reported between 7% and 14%, as compared to RASP.23,24 These observations position RASP advantageously when compared to other enucleation techniques. 25 It is important to note, however, that their results contrast with those obtained by Sorokin et al., 17 where no incontinence was observed in cases comparing RASP versus HoLEP. Furthermore, obesity has been identified as a risk factor for irritative symptoms and incontinence-related symptoms following benign prostate surgery. This should be considered as an important influencing factor during outcome evaluation and group comparisons. 26 Our results are comparable to those obtained by Okullo et al., 18 who conducted a comparative analysis of functional outcomes, however, their study only assessed 27 patients with robotic modified Freyer’s prostatectomy. Postoperative IPSS was remarkably low in their cohort compared to ours (1.25 vs 4). The Q-max (29.6 ml/s vs 25 ml/s), and PSA (1.2 ng/ml vs 1 ng/ml) were comparable between the two studies, while our cohort showed a lower PVR (55.9 ml vs 10 ml). Regarding postoperative Clavien score, our results are comparable to other studies that show a low incidence of minor complications (Clavien 1).4,5 This strengthens the robustness of our findings with the broader context of relevant research.
Simplifying the previous reported BPH-67 to a three-element BPH-3 achievement significantly boosts the overall achievement rate from 40% to 89%. When assessing Freyer and Madigan techniques individually, achievement rates between BPH-6 and BPH-3 in Freyer and Madigan technique increase from 28% to 92% for Freyer and 48%–80% for Madigan, respectively. Although a stricter evaluation of postoperative results with the BPH-6 could give a more precise understanding of the postoperative performance and self-perception of the patient, in this analysis, the only notable difference, as expected, was a better ejaculation perception as evaluated by the MSHQ, question 3. it is worth mentioning, that sexual function was no different between both groups when evaluated with ∆ IIEF. Excluding non-functional items from the BPH-6, such as QoR VAS, a simplified BPH-3 assessment reveals that, regardless of the surgical technique employed, both procedures achieve significant completion in a trimodal evaluation. Consistent results have been observed when comparing these trifecta outcomes with pentafecta, which includes antegrade ejaculation (MSHQ > 0) and erectile function (ΔIEEF < 6). The core trifecta outcomes showed a rate of 60% as opposed to 20% for pentafecta.27,28
To our knowledge this is the first study proposing BPH-3 as a tool to evaluate trifecta outcomes following robotic simple prostatectomy with either Freyer or Madigan technique. External validation must be carried out prospectively to assess the efficacy of this tool. Although LUTS have been proved to be a condition with many edges in their origins, 2 when applied to benign prostatic obstruction (BPO), parameters such as ∆ IPSS ⩾ 30%, ISI score ⩽ 4, and Clavien < 1 emerge as robust indicators for evaluating postoperative outcomes in terms of relief of prostatic obstruction.
While our study lacks the randomization typically seen in clinical trials, it compensates with the strengths of a substantial and well-documented cohort, a thorough 12-month postoperative follow-up, procedures conducted by seasoned robotic surgeons, and the diligent prospectively recorded data.
The overall increase in minimally invasive strategies to relieve bladder outlet obstruction due to prostate enlargement continues to expand. Evaluation of outcomes is challenging in the context of a complex myriad of functional variables. However, regarding relief of obstruction, the proposal of the BPH-3 may be an attractive tool for non-sexual functional assessment, even after a long-term follow-up. BPH-3 completion rates, are no different between Robot-Assisted Madigan Prostatectomy and Robot-Assisted Freyer Prostatectomy
Footnotes
Author contributions
Conceptualization: A.M.B; A.B; S.D.; L.M. Data Curation: A.M.B.; A.B.; S.D.; L.M.; R.M.; G.T.; R.S.F; D.A. Formal Analysis: A.M.B.; A.B.; S.D.; L.M.; R.M.; R.S.F. Investigation: A.M.B.; A.B.; S.D.; L.M.; R.M.; G.T.; M.F.; R.S.F.; L.M.; F.P. Methodology: A.M.B; A.B; L.M; U.A.; M.C.F.; R.S.F.; F.P.; D.A. Project Administration: A.M.B; M.F.; F.P.; D.A.; F.P.; C.L.; G.S. Resources: A.M.B; G.T.; R.M.; U.A.; M.F.
Software: A.M.B; A.B.; R.S.F.; F.P. Supervision: A.M.B; A.B.; F.P.; C.L.; G.S. Validation: A.M.B; R.P.; A.B; M.F.; F.P.; C.L.; G.S. Visualization: A.M.B; R.P.; A.B; M.F.; F.P.; C.L.; G.S. Writing – Original Draft Preparation: A.M.B; R.P; A.B; S.D. Writing – Review and Editing: A.M.B; R.P; A.B; S.D.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Approval of the research protocol
The international Review Board approved this protocol with number: 1722/22.
Informed consent
N/A.