
Abstract
Background:
To study the impact of early in comparison to late catheter removal following acute urine retention (AUR) secondary to benign prostatic hyperplasia (BPH) using silodosin therapy on the outcome of trial without catheter (TWOC).
Methods:
Two hundred sixty patients with AUR 2ry to BPH were catheterized then were randomly divided to receive silodosin 8 mg either for three or 7 days followed by catheter removal and successful voiding unaided was assessed.
Results:
Out of the 260 men (mean age 64.8 ± 6.5 years) treated, 74 men who were receiving 3 days of silodosin and 88 patients who were receiving 7 days of silodosin didn’t require re-catheterization on the day of TWOC (57% and 68% respectively, p = 0.096). Complications like urinary leakage, acute urinary tract infection, hematuria, or catheter blockage recorded in 21 men (16.2%) who received 3 days of silodosin, and in 63 men (48.5%) who received 7 days of silodosin (p ⩽ 0.001).
Conclusion:
Patients catheterized after AUR 2ry to BPH can spontaneously void following catheter removal if treated by silodosin, independent of the catheterization duration, while side effects have increased with prolonged catheterization.
Introduction
The incidence of acute urine retention (AUR) due to benign prostatic hyperplasia (BPH) ranges from 0.4% to 25 %. 1 Urethral catheterization is the first procedure in these patients followed by appropriate intervention. The usage of trial without catheter (TWOC) has been increased recently as immediate surgery is linked with high morbidity and mortality and due to significant complications of prolonged catheterization. 2
Mechanism of action of Alpha-1 (α1)-blockers depends mainly on reducing smooth muscle fibers tone within the prostate, therefore it leads to a rapid improvement of urinary symptoms with better urinary flow. There is a wide variety of α1-blockers either selective as Doxazosin, Alfuzosin and Terazosin or highly selective as tamsulosin and silodosin. The efficacy and outcome of all these drugs are comparable while the main difference between them lies in patient’s tolerability and side effects. 3
The value of use of α1-blockers in AUR patients is to reduce bladder outlet resistance with improving chances of successful TWOC. 4 Prolonged catheterization is associated with significant increase of many morbidities like catheter blockage, urine leakage, hematuria, urinary tract infection, urosepsis and even urethral stricture. So, we should spare no effort in trying to minimize the duration of catheterization which eventually reduces the forementioned complications and public health services costs. 5
The use of alpha blockers and catheterization >3 days increases the chances of successful TWOC. However, till now there is no consensus about the ideal catheterization duration through which medical treatment is used before TWOC. 1 Our study aim was to investigate the efficiency of early in comparison to late urinary catheter removal in patients with AUR due to BPH after silodosin treatment on the outcome of TWOC.
Methods
A prospective randomized study carried out in our tertiary care hospital including male patients presented with first attack of AUR secondary to BPH and no previous use of alpha blockers. Exclusion criteria were patients with initial catheterization volume >1500 ml or <500 ml, bladder stones, patients with renal impairment, neurogenic bladder, malignancy, medically induced urinary retention (α agonists and antihistaminic drugs), patients with history of drug hypersensitivity or allergy to silodosin and patients with previous prostate surgery and stricture urethra. Our institution ethical committee approval (numbered R 166/2023) and informed written consents from all patients were signed before starting the study.
Using STATA version II program, setting type-1 error (α) at 0.5 and power at 80%. Results from study by Desgrandchamps et al. concluded that the success rate in the early group was 55.2% 6 while for the late group Li et al. reported 79% success rate. 7 Calculations according to these values, showed that the required sample size is 87 cases in each group.
A total of 425 male patients with AUR due to BPH were assessed to be involved in the study. One hundred sixty-five patients were excluded for many reasons. For not meeting inclusion criteria, 95 patients were excluded while 70 declined to participate as shown in Figure 1. The remaining 260 patients were randomly categorized (1:1) into two groups by closed envelope method, catheterized, and received urinary antiseptic; group I: 130 patients had silodosin 8 mg once daily for 3 days then catheter removal and group II: 130 patients had silodosin 8 mg once daily for 7 days then catheter removal.
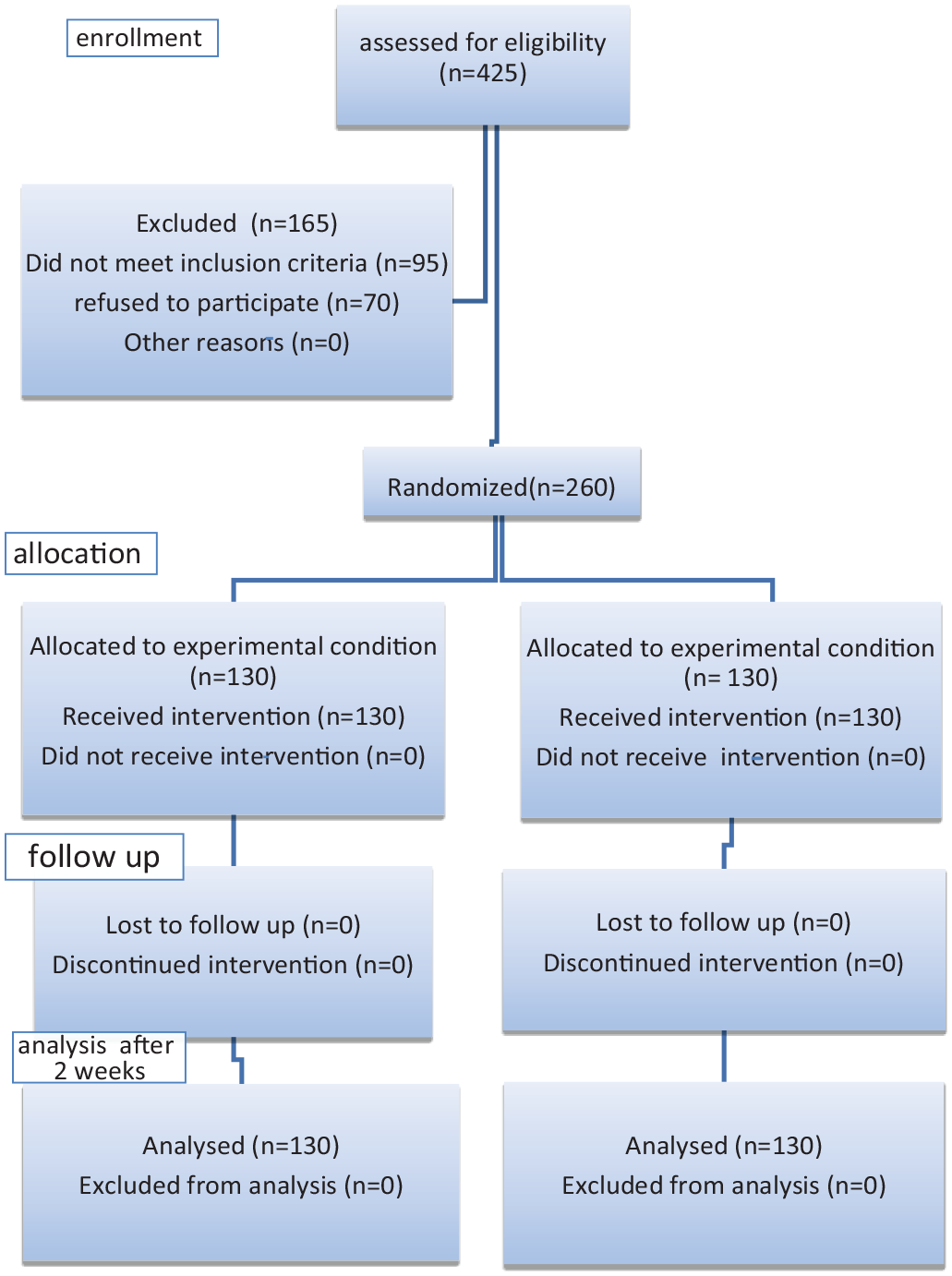
CONSORT flowchart.
In all patients, full medical history was obtained with detailed analysis of lower urinary tract symptoms (LUTS) prior to retention. Past medical and surgical history was recorded. Thorough physical examination was done; it included Digital Rectal Examination (DRE) and focused neurological examination.
Patients were evaluated after catheterization with complete urine analysis, urine culture and sensitivity tests if required, kidney function tests, prostatic-specific antigen (PSA), transrectal ultrasonography was performed to determine prostate size and pelviabdominal ultrasonography to exclude any other bladder pathologies. Incidence of Complications after urinary catheterization as urinary tract infection (UTI), hematuria, catheter obstruction and urinary leakage were monitored and recorded in both study groups.
Our primary endpoint was successful voiding (TWOC) after urinary catheter removal, this was defined as free voiding of 200 ml of urine or more in a single void, within <6 h of removal of the catheter and with postvoiding residual urine <200 ml. Patients who voided successfully were discharged home and continued alpha blocker treatment with scheduled follow up at outpatient clinic after 2 weeks. While those who failed to void were re-catheterized and scheduled for intervention. The secondary endpoints were free voiding after 2 weeks, estimation of post voiding residual urine volume (RV) using pelviabdominal ultrasonography and measurement of peak flow rate (Qmax) on uroflowmetry study.
The statistical methods were carried out using SPSS version 21 for windows (Chicago, IL). Numerical data with normal distribution was expressed as mean ± SD and differences between groups were measured by the independent Student’s t-test and categorical variables were compared by the χ2 test or fisher exact test and were expressed as number (%). p < 0.05 was considered to be statistically significant.
Results
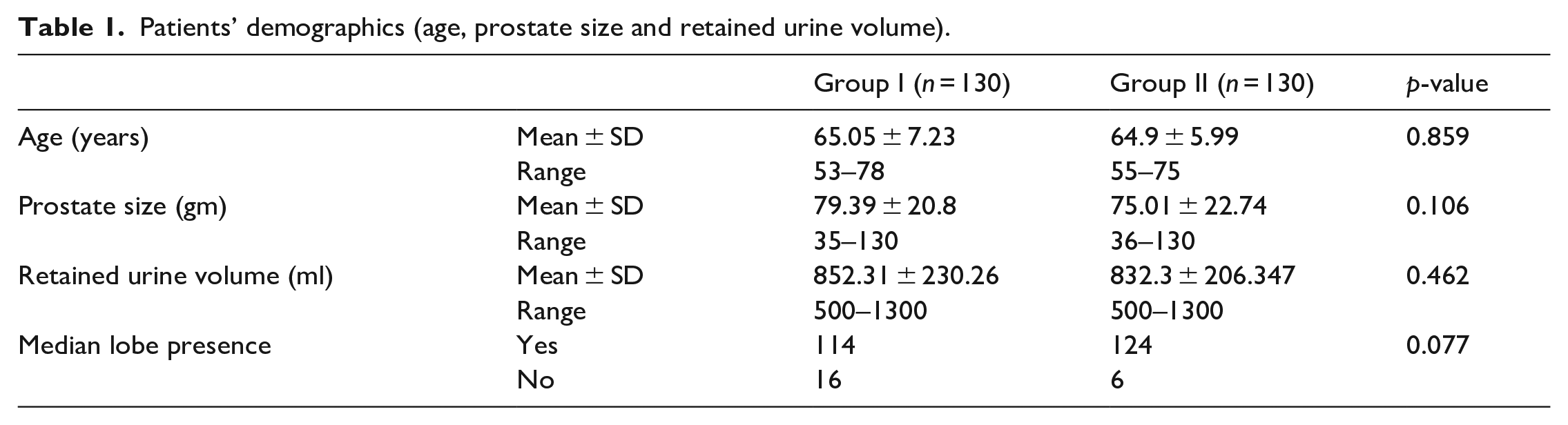
Comparison of age, prostate size, RV, and presence of median lobe between the two groups, showed no statistically significant difference (p = 0.859, 0.106, 0.462, and 0.077 respectively). See Table 1.
Patients’ demographics (age, prostate size and retained urine volume).
Group I had a success rate of 57% upon TWOC and 68% in group II, difference wasn’t statistically significant (p = 0.096). The mean RV (in patients who voided successfully) after 2 weeks in group I was 73.9 ± 46.03 ml and the mean volume in group II was 58.11 ± 54.6 ml and the difference wasn’t statistically significant (p = 0.52). The mean Qmax (in patients who voided successfully) after 2 weeks in group I was 12.66 ± 2.49 ml/s and the mean in group II was 12.39 ± 3.41 ml/s and the difference wasn’t statistically significant (p = 0.578). See Table 2.
Comparison of RV and Qmax between the studied groups.

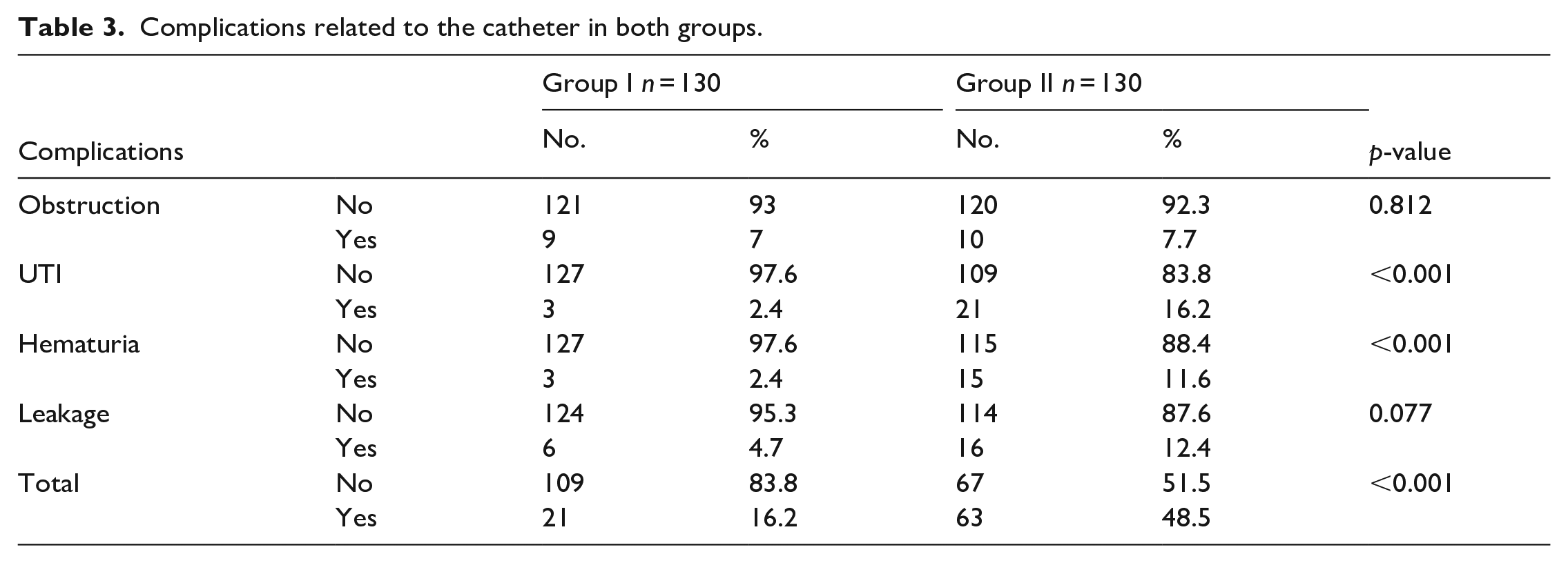
Patients in group I had complications related to the catheter (16.2%) that were significantly lower in comparison with group II (48.5%) (p ⩽ 0.001). See Table 3.
Complications related to the catheter in both groups.
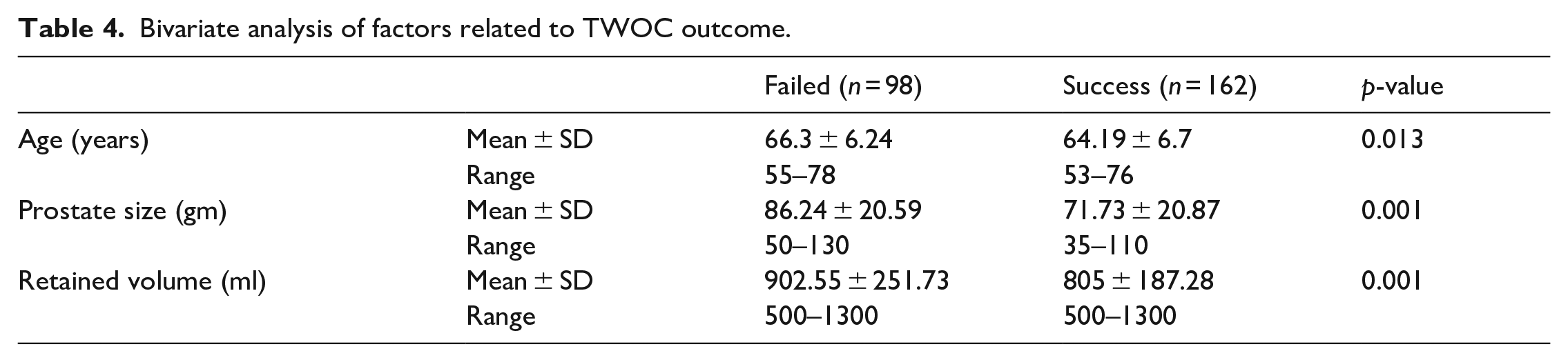
Bivariate analysis was done to identify variables that may have an effect on TWOC success. The difference between the mean of prostate size in failed and succeeded cases was significant (p = 0.001). Also, retained urine volume difference between patients who failed to void and those with successful TWOC was statistically significant. While age was a non-significant factor. See Table 4.
Bivariate analysis of factors related to TWOC outcome.
Discussion
The most common benign tumor in men is BPH, and it has age related incidence. The prevalence of histologic BPH in autopsy studies increases from about 20% in men 41–50 years, to 50% in men 51–60 years, and to more than 90% in men older than 80 years. 8 Studies from Asia, Europe and US also showed that old age is a risk factor for onset and progression of clinical BPH. 9 Furthermore, prostate volume increases with age as concluded from the Krimpen and Baltimore Longitudinal Study of Aging demonstrating a prostate growth rate of about 2.0%–2.5% every year in older men.10,11
It was suggested by Shim and colleagues that the use of α1-blockers before a TWOC inhibits the recurrence of AUR and increases the chance of spontaneous voiding. 12 However, the optimal duration of treatment has not been fully defined, and there is controversy regarding the optimal duration of time a catheter should stay in situ during the initial treatment phase. 1
As regards the patients in our study their mean age was 64.8 ± 6.5 years and there was significant difference in TWOC outcome with age as the mean age among succeeded cases was 64.19 ± 6.7 years while among failed cases was 66.3 ± 6.24 years (p = 0.013). Also, Fitzpatrick et al. found that older cases showed a significant more TWOC failure rate than younger cases in agreement with our study. 5
Emberton et al. found that smaller prostate size was linked with an increased TWOC success rate 13 which was in agreement with our study where the mean prostate size among succeeded cases was 71.73 ± 20.87 gm while mean size in failed cases was 86.24 ± 20.59 gm which was significantly different (p = 0.001) which was also in agreement with Fitzpatrick et al. 5
Our results showed that retained amount of urine at catheterization time among succeeded was 805 ± 187.28 ml and among failed cases was 902.55 ± 251.73 ml, the difference was statistically significant (p = 0.001). Several studies have shown that if RV at the catheterization time is ⩾ 1 l, it might be a risk factor for failed TWOC, which demonstrates a relation between RV and success of TWOC14,15 On the other hand, many authors have found that the RV has no predictive value for the outcome of TWOC.16,17
As regards duration of catheterization in relation to TWOC success rate, our study demonstrated that the group of patients who were catheterized for 7 days had a slightly greater success rate than the group who were catheterized for 3 days, the percentage was 68% and 57% respectively but this result was statistically insignificant (p = 0.096).
Li and colleagues in Hong Kong found a remarkable rise (26.6%) in TWOC at first follow up (day 3) but only a small (2.1%) further contribution from the second follow up (day 6) so, they concluded that those who failed TWOC on day 3 would get limited benefit with more trials and this was in agreement with our study. 7 In another study by Kwangsu et al. on 135 patients who underwent a TWOC, the trial succeeded in 100 patients (74%), but 35 patients (26%) had an indwelling catheter due to voiding failure they divided the patients into those with catheterization ⩾ 5 days and those with catheterization <5 days. There was no statistically significant difference in the success rate in the two groups (81%vs 77%, p > 0.05) again in agreement with our study. 18 In contrary, Desgrandchamps et al. showed that the TWOC success rate was also higher following catheter removal after 1–3 days than for a longer duration of catheterization, In their study, the TWOC success rate was higher for short catheter duration (63.2%, 52.7%, and 52.5% after 1, 2 and 3 days, respectively) than long catheter duration (41.5% and 46.9% for 4–7 and >7 days, respectively). However, their study wasn’t randomized. 6
As regards side effects of catheterization, our study concluded that the total complications rate was 32.3% and the rate was significantly higher in the group catheterized for 7 days (48.5%) than in the group catheterized for 3 days (16.2%) and this difference was statistically significant (p ⩽ 0.001). In a study by Emberton et al. showed that catheterization for > 3 days compared with ⩽ 3 days was associated with a significantly higher incidence of side effects (33.1%, 17.5%; p < 0.001) such as asymptomatic bacteriuria, gross hematuria, lower UTI, urosepsis, and urine leakage and catheter blockage. 13 Fitzpatrick et al. found that Catheterization for >3 days was associated with a significantly higher rate of adverse events compared with those catheterized for 3 days or less (33.8% vs 19.7%, p < 0.001). 5 Also, Desgrandchamps et al. found that the risk of catheter-related complications was related to the duration of catheterization, those men catheterized for > 3 days having a significantly higher rate of adverse (32.3%) events than those catheterized for ⩽ 3 days (15.9%) (p < 0.001). 6 Regarding bacteriuria, Stensballe et al. concluded that patients with catheters suffered from bacteriuria with different rates. Incidence of change from sterile urine to bacteriuria happened at the rate of 3%−10% per day. 19
Our study main limitation is mainly not considering some factors like IPSS and PSA in relation to the outcome of TWOC. However, these results can aid in establishing a protocol for management of patients with AUR 2ry to BPH but more studies on a larger sample of patients are needed to validate these findings.
We concluded that no difference in the success rate of early in comparison to late catheter removal after silodosin usage in BPH patients with AUR. However, other factors may influence the success of TWOC whether early or late catheter removal as the size of the prostate and the retained urine volume before catheterization. Also, late catheter removal was found to be associated with increased risk of complications.
Footnotes
Acknowledgements
None.
Abbreviations
AUR acute urine retention, BPH benign prostatic hyperplasia, TWOC trial without catheter, LUTS lower urinary tract symptoms, DRE digital rectal examination, PSA prostatic-specific antigen, UTI urinary tract infection, RV residual urine volume and Qmax peak flow rate.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.