
Abstract
Background and objectives:
There is no recommendation on the timing of ureterolithotripsy after the treatment of obstructive acute pyelonephritis (APN). The effect of early and delayed ureterolithotripsy on postoperative urinary tract infection (UTI) and other complications was investigated.
Methods:
Patients who underwent ureterolithotripsy after obstructive APN treatment between February 2017 and August 2021 were divided into two groups, those operated during hospitalization and those operated within 3 months after discharge. Two groups were compared in terms of stone-free status, postoperative complications, postoperative UTI, and urosepsis rates.
Results:
Of the 91 patients included in the study, 68 were in the early ureterolithotripsy group, while 23 patients were in the delayed ureterolithotripsy group. The postoperative UTI rate was significantly higher in patients who underwent early ureterolithotripsy (29.4% vs 8.7%, p = 0.045). Patients with postoperative UTI had a higher moderate/severe perinephric fat stranding (PFS) on non-contrast CT at hospital admission (52.2% vs 29.4%, p = 0.048). Among the laboratory parameters, white blood cells were significantly higher in the group with postoperative UTI (21604.5 vs 14728.9, p = 0.042). In the multivariate analysis, early ureterolithotripsy and moderate/severe PFS were independent predictors for postoperative UTI. In the created model, the probability of postoperative UTI after ureterolitripsy after obstructive APN treatment was 3.5% in patients without risk factors, while this rate was 51.9% in patients with both risk factors.
Conclusion:
There is no consensus on the timing of stone removal after treatment of obstructive APN. Early ureterolithoripsy and moderate/severe perinephric fat stranding on non-contrast CT are risk factors for postoperative UTI.
Keywords
Introduction
Ureteral stone-associated obstructive acute pyelonephritis (APN) can cause severe symptoms which can lead to systemic inflammatory response syndrome (SIRS), septic shock, and even mortality. Recent studies showed that the mortality rate is around 2% in obstructive APN. 1 Considering the clinical condition of the patient, the size of the stone, the degree of hydronephrosis and other radiological findings, and laboratory parameters, drainage and antibiotherapy should be applied quickly. 2 After the patient’s infection parameters and symptoms regress, stone removal should be performed. Laser ureterolithotripsy, together with ESWL, are the recommended treatment methods for ureteral stones. Although ureterolithotripsy offers high stone-free rates, there are also significant postoperative complications. Postoperative urinary tract infection (UTI) is the most common complication following ureterolithotripsy. 3 Postoperative complications after obstructive APN treatment may be more severe than in primary patients.
There is no definite recommendation regarding the timing of ureterolithotripsy after treatment of obstructive APN. The guidelines particularly emphasize obtaining a preoperative sterile urine culture. 2 However, there is no specific recommendation on other risk factors to pay attention to. In our study, we investigated the effect of early or delayed ureterolithotripsy after obstructive APN treatment, on stone-free rates, postoperative complications, and postoperative UTI. We also evaluated other factors that could lead to postoperative UTI.
Material and methods
Patients who were admitted to our clinic with obstructive acute pyelonephritis between February 2017 and August 2021 were retrospectively reviewed. Patients who underwent endoscopic Ho:YAG laser lithotripsy for ureteral stones and who were operated within 3 months of hospitalization, and patients with a sterile urine culture prior to 1 week of lithotripsy were included in the study. They were divided into two groups, those who underwent early or delayed ureterolithotripsy. Patients who were operated during the hospitalization (within 2 weeks) following obstructive acute pyelonephritis treatment were included in the early ureterolithotripsy group, and patients who were operated after discharge (after 4 weeks), within 3 months were included in the delayed ureterolithotripsy group. Demographic data of patients such as age, gender, body mass index (BMI), comorbidities, characteristics such as stone burden, number of stones, degree of hydronephrosis, type of drainage, perinephric fat stranding (PFS), and tissue rim sign on non-contrast CT, preoperative infectious parameters and postoperative success, urinary system infection, SIRS complications were screened.
Acute pyelonephritis was defined as fever ⩾38°C and flank pain/costovertebral angle tenderness accompanied by pyuria or positive urine culture. 4 The presence of elevated WBC at complete blood count or elevated CRP strengthened the diagnosis. Postoperative UTI was defined as postoperative fever and a positive urine culture. Urosepsis was defined as the presence of ⩾2 systemic inflammatory response (SIRS) criteria (hyperthermia or hypothermia, leukocytosis or leukopenia, tachycardia, and tachypnea) and a positive urine culture. Urine and blood cultures were obtained from each patient, and empirical parenteral antibiotherapy, third generation cephalosporins as the first choice or other β-lactam antibiotics as the second choice, was administered. DJ stent or nephrostomy tube was inserted in patients with hydronephrosis, according to the decision of the clinician. Some patients with mild hydronephrosis and quick response to antibiotherapy were not drained. Urine cultures were also obtained from each patient following the decompression. Antibiotics were changed considering culture-antibiogram sensitivity testing. Antibiotherapy was continued for 7–21 days according to the patients’ clinical response. Laboratory parameters WBC, CRP, and creatinine were monitored during hospitalization. It was required that the urine culture be sterile in the preoperative 1-week period and 3 days period without fever. Dj stent was placed for each patient at the end of the ureterolithotripsy and removed within 2 weeks after the procedure. Nephrostomy tubes were removed after operation. Residual fragments, stones ⩾4 mm, were assessed using a plain abdominal radiograph (KUB) on the first postoperative day. Antibiotherapy was continued for 3 days following ureterolithoripsy.
Findings such as stone length, number, location of stones, degree of hydronephrosis, tissue rim sign, and perinephric fat stranding were defined by a clinician blind to the clinical information of the patients according to non-contrast CT. The tissue rim sign was defined as present or absent according to the annular soft-tissue attenuation around the stone. 5 The perinephric fat stranding was evaluated as none, mild = few thin lines, moderate = between mild and severe, severe = many thick lines according to the linear soft-tissue attenuation around the kidney. 6
The factors affecting postoperative UTI were analyzed and a model was created to predict postoperative UTI.
Ethical board approval was obtained for this study (2021/0473).
Statistical analysis
Statistics were performed using SPSS v22.0 (SPSS Inc, Chicago, IL, USA). The normal distribution between groups was assessed using Kolmogorov-Smirnov test. Independent samples t-test was used for comparing the means. Mann Whitney-U test was used comparing two non-parametric variables. The Chi-square test or Fisher’s exact test was used for categorical variables. Logistic regression was performed for multivariate analysis and p-value <0.05 was considered statistically significant. The probability (P) of postoperative UTI was calculated using log-odds (linear prediction (LP)), as shown in the following equations: b0 is the constant (B) of logistic regression analysis. “e” is a mathematical constant value, which is approximately equal to 2.718. B1, B2 (Beta) are the predicted change in Log Odds of each variable.


Results
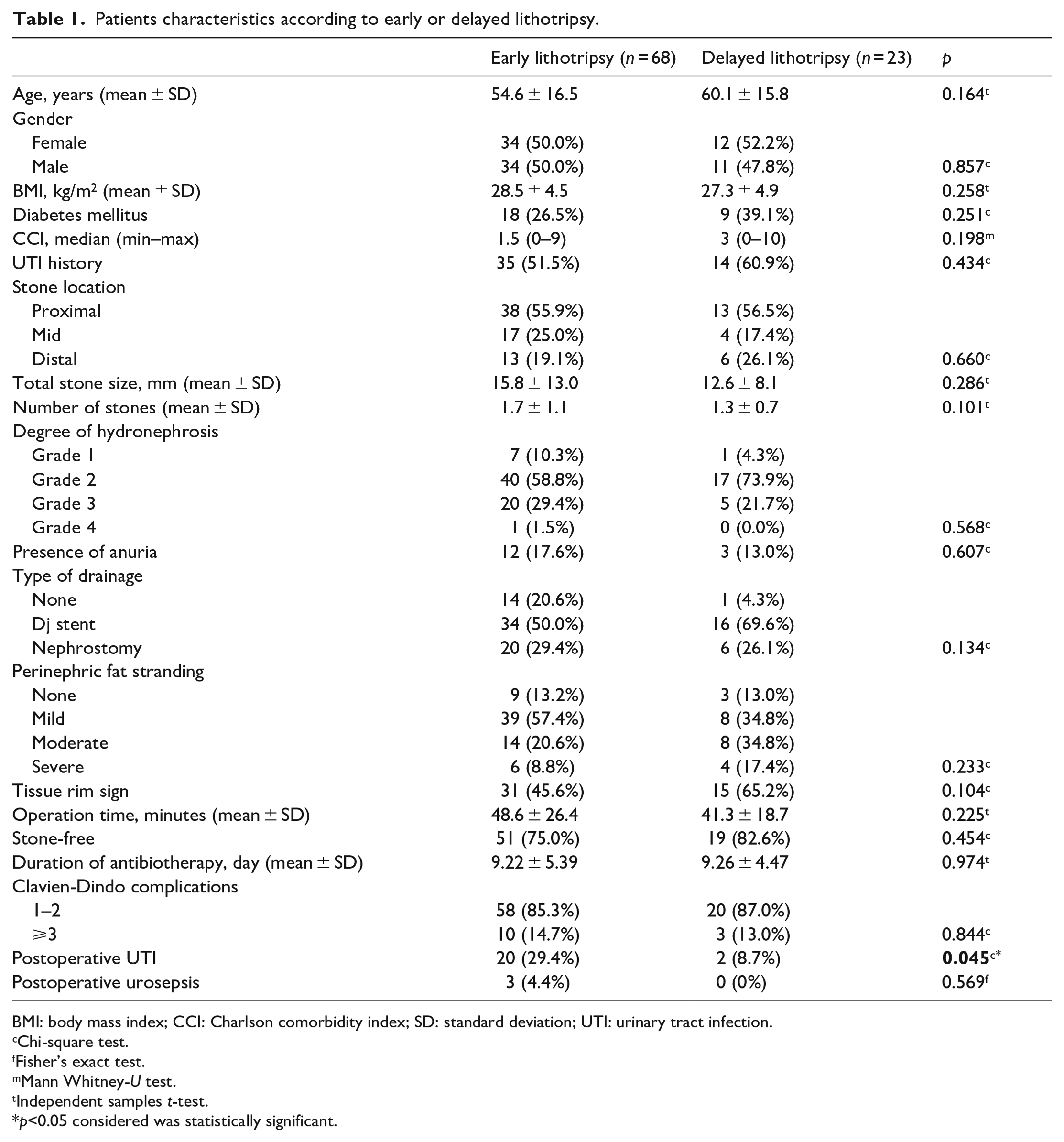
A total of 91 patients with obstructive acute pyelonephritis were included in our study. Sixty-eight (74.7%) patients underwent early ureterolithotripsy, and 23 (25.3%) patients underwent delayed lithotripsy. Delayed lithotripsy was performed in 17 (73.9%) patients due to pandemic and 6 (26.1%) due to patient preference. In the delayed ureterolithotripsy group, the interval between hospital admission and lithotripsy was 45.5 days overall, in the early ureterolithotripsy group it was 10.6 days overall. Patient characteristics were similar between groups. Total stone size, number of stones, degree of hydronephrosis, type of drainage, perinephric fat stranding, and tissue rim sign were similar between patients who underwent early and delayed ureterolithotripsy. Stone free rates (75.0% vs 82.6%, p = 0.454), complications requiring surgical, endoscopic, or radiological interventions were similar between groups (14.7% vs 13.0%, p = 0.844). Patients with early lithotripsy had a higher rate of postoperative UTI than patients with delayed lithotripsy (29.4% vs 8.7%, p = 0.045). Three (4.4%) patients with early lithotripsy developed sepsis without the need for an intensive care unit (ICU), and none of the patients with delayed ureterolithotripsy had postoperative sepsis (Table 1).
Patients characteristics according to early or delayed lithotripsy.
BMI: body mass index; CCI: Charlson comorbidity index; SD: standard deviation; UTI: urinary tract infection.
Chi-square test.
Fisher’s exact test.
Mann Whitney-U test.
Independent samples t-test.
p<0.05 considered was statistically significant.
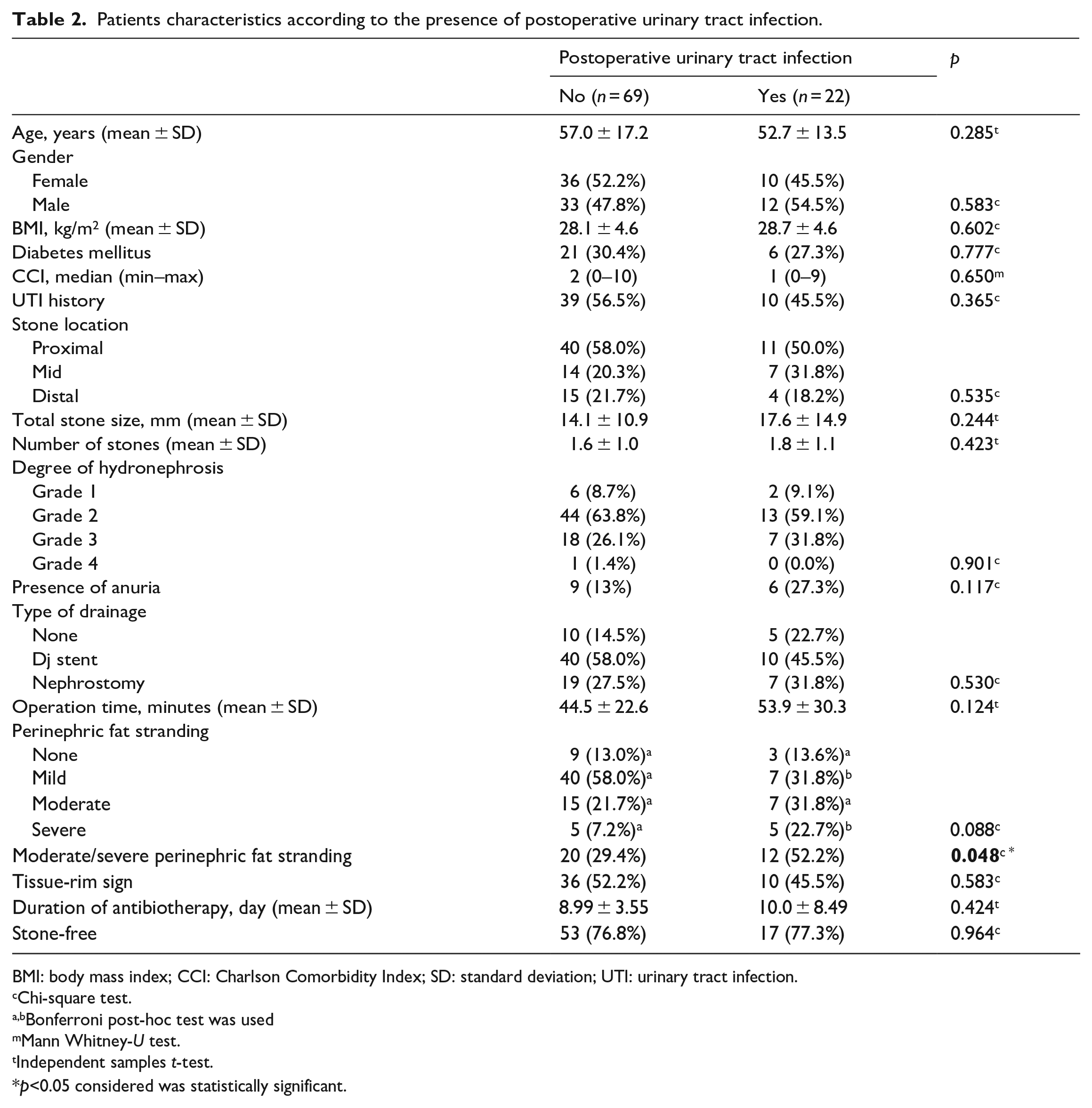
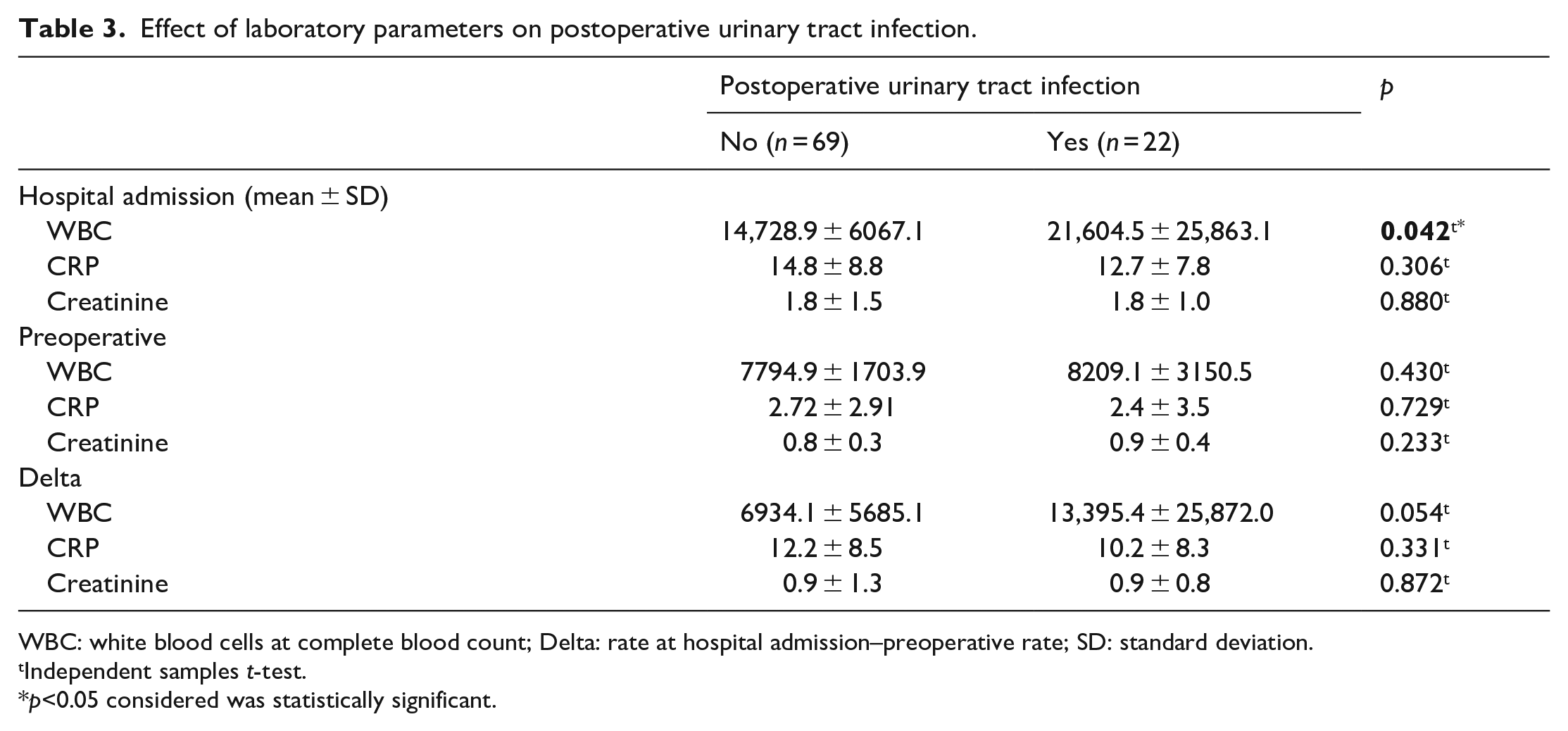
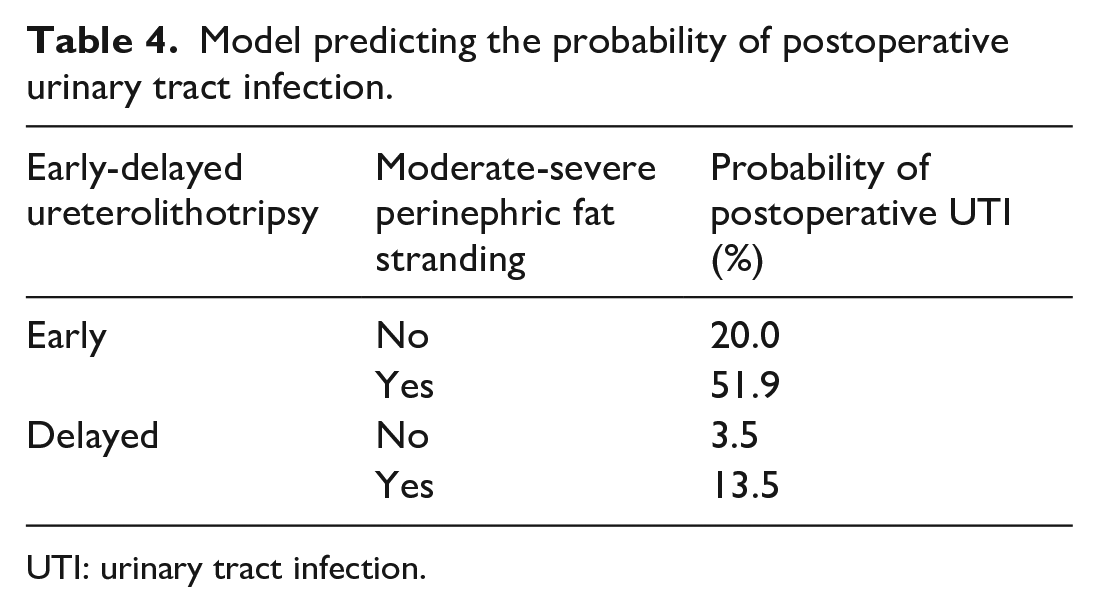
Patients with and without postoperative UTI had similar stone size, number of stones, and degree of hydronephrosis. Moderate or severe perinephric fat stranding rate was higher in those with postoperative UTI (52.2% vs 29.4%, p = 0.048). Both groups had similar rates of tissue rim sign (45.5% vs 52.2%, p = 0.583) (Table 2). Patients with postoperative UTI had higher WBC at hospital admission (21604.5 vs 14728.9, p = 0.042) (Table 3). In the multivariate analysis, moderate or severe perinephric fat stranding (OR: 4.3, p = 0.008) and early ureterolithotripsy (OR: 6.9, p = 0.02) were independent predictors of postoperative UTI. According to multivariate analysis a model to predict the probability of postoperative UTI was created. Patients with both risk factors had a probability of postoperative UTI of 51.9%, and patients without risk factors had a probability of 3.5% (Table 4).
Patients characteristics according to the presence of postoperative urinary tract infection.
BMI: body mass index; CCI: Charlson Comorbidity Index; SD: standard deviation; UTI: urinary tract infection.
Chi-square test.
Bonferroni post-hoc test was used
Mann Whitney-U test.
Independent samples t-test.
p<0.05 considered was statistically significant.
Effect of laboratory parameters on postoperative urinary tract infection.
WBC: white blood cells at complete blood count; Delta: rate at hospital admission–preoperative rate; SD: standard deviation.
Independent samples t-test.
p<0.05 considered was statistically significant.
Model predicting the probability of postoperative urinary tract infection.
UTI: urinary tract infection.
Linear Prediction (LP) = −3.321 + 1.461 × moderate or severe PFS (0 or 1) + 1.937 × early lithotripsy (0 or 1). The probability of postoperative UTI was calculated with the formula of = e^LP/(1 + e^LP).
Stone analysis of 31 patients was available. Fifteen (48.4%) of them were calcium oxalate (including mixture with calcium phosphate), 6 (19.4%) uric acid, 5 (16.1%) cystine, 5 (16.1%) infection stones.
Discussion
In this study, we evaluated the clinical impact of early or delayed ureterolithotripsy following obstructive APN, and also the factors leading to postoperative UTI. Patients who underwent early ureterolithotripsy had a higher rate of postoperative UTI. Early ureterolithotripsy and moderate/severe PFS at hospital admission were independent risk factors for postoperative UTI.
Ureterolithotripsy after obstructive APN has different characteristics compared to the primary ureterolithotripsy. It should be kept in mind that the obstructed system is more closely associated with complications such as postoperative UTI and sepsis. However, the number of studies about the timing of the operation and its postoperative complications is very limited. Youssef et al. compared the complication rates between ureterolithotripsy following sepsis due to obstructive APN and primary ureterolithotripsy. Patients presenting with sepsis developed significantly higher complications (20% vs 7%, p = 0.007) and postoperative fever (7.2% vs 0%) after ureterolithotripsy. 7 Therefore, it should be known that the factors affecting UTI after ureterolithotripsy, such as UTI history, residual fragments, and comorbidities may differ in this patient group, and different principles should be defined in the treatment of stone removal after APN treatment.8,9
Stone burden, degree of hydronephrosis, and non-contrast CT findings were similar in patients with early and delayed ureterolithotripsy. Patients who underwent early ureterolithotripsy, during hospitalization after obstructive APN treatment, had a higher postoperative UTI rate compared to patients with delayed ureterolithotripsy (29.4% vs 8.7%, p = 0.045). Yoo et al. showed that patients with postoperative SIRS had a shorter APN to ureterolithotripsy interval (7.0 vs 15.0 days, p = 0.027). It was stated that antibiotic therapy for less than 14 days caused postoperative SIRS. 10 In our study, early and delayed groups had similar duration of antibiotherapy (9.22 vs 9.26 days, p = 0.974) In this study we investigated primarily, the effect of performing early or delayed ureterolithotripsy after a standard antibiotherapy. Contrary to Yoo et al. we excluded renal stones and the number of stones, stone sizes were homogeneously distributed. Itami et al. 11 stated that Dj stent for 21 days or more increased the postoperative UTI rate following endoscopic renal stone removal after obstructive APN treatment significantly. Yamashita et al. 12 defined female gender and multiple stones as independent factors for postoperative UTI following stone removal after APN treatment, however, 18.7% of patients had renal stone removal and stone characteristics were not homogeneously distributed. Whether lithotripsy is intrarenal or ureteral, creates significant differences in terms of intrarenal pressure. Xia et al. showed that lithotripsy in the distal ureter caused significantly lower intrarenal pressure than proximal ureter (74.6 vs 110.3 cmH2O). To avoid heterogeneous groups with different characteristics, such as renal and ureteral lithotripsy, we included only patients with ureteral stone removal.
There are no studies that could explain the lower postoperative UTI rates in the delayed group, but persistence of bacteriuria for weeks after the elimination of obstruction may clarify this. Johnson et al. 13 showed in their experimental study on mice, that acute pyelonephritis develops in a short period of 1–6 h after obstruction and histological findings of pyelonephritis persist 3 and 6 weeks after the elimination of obstruction. Early ureterolithotripsy will increase intrarenal pressure and exacerbate existing bacteriuria through pyelovenous leakage.
On non-contrast CT at hospital admission, it was observed that patients with postoperative UTI had a higher rate of moderate/severe PFS (52.2% vs 29.4%, p = 0.048). Other stone-related and clinical parameters of the patients with and without postoperative UTI were homogeneously distributed. PFS is a common CT finding in APN patients, with a prevalence of 29.1%–72%.14,15 Yu et al. 15 showed that PFS was associated with bacteremia in UTI (40.8% vs 21.2%, p = 0.004). Tanizaki et al. 16 also stated that PFS was seen at a higher rate in those with bacteremia, and median peak body temperature was higher (38.8°C vs 38.5°C, p < 0.001). Although PFS does not have high sensitivity in diagnosing APN, it can be used to predict more severe course of APN as previously shown and postoperative UTI after ureterolithotripsy.
Patients with postoperative UTI had significantly higher WBC at hospital admission (21,604.5 vs 14,728.9, p = 0.042). The improvement rate in laboratory parameters was similar between groups. Yoo et al. 10 found that preoperative CRP of 6 mg/L and higher was found to be an independent predictor for postoperative SIRS following ureterolithotripsy after APN. Although we could not detect the effect of CRP or other preoperative parameters, it should be kept in mind that APN patients with high WBC values at hospital admission may encounter UTI in the postoperative period.
This is the first study creating a comprehensive model to predict postoperative UTI following the treatment of obstructive APN. Early ureterolithotripsy and moderate/severe PFS were independent risk factors included in our model to predict postoperative UTI in patients who underwent ureterolithotripsy after obstructive APN. While the risk of postoperative UTI was 3.5% in the absence of risk factors, the risk was 51.9% when both risk factors were present. There are several limitations of our study, first of these was that the study was retrospective and had a limited number of patients. Second, although each patient received 7–21 days of antibiotherapy for APN, a standardized antibiotic regimen was not applied. Urine cultures of the patients were heterogeneous and resistant bacterial strains were not compared between the two groups, and stone analysis could not be performed on all patients.
Conclusion
Early ureterolithotripsy and moderate/severe perinephric fat stranding on CT at hospital admission were independent risk factors for postoperative urinary tract infection following acute obstructive pyelonephritis treatment.
Supplemental Material
sj-docx-1-urj-10.1177_03915603231210604 – Supplemental material for Early versus delayed ureterolithotripsy following obstructive acute pyelonephritis treatment
Supplemental material, sj-docx-1-urj-10.1177_03915603231210604 for Early versus delayed ureterolithotripsy following obstructive acute pyelonephritis treatment by Huseyin Ozgur Kazan, Muhammet Cicek, Hulya Caskurlu, Ramazan Gokhan Atis and Asif Yildirim in Urologia Journal
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.