
Abstract
Objectives:
This study aims to assess the efficacy of Clam enterocystoplasty (CECP) surgery for the treatment of non-neurogenic refractory urgency urinary incontinence (UUI).
Methods:
We conducted a retrospective evaluation of 17 female patients who underwent CECP for non-neurogenic refractory UUI between May 2010 and November 2022.
Results:
The median of ICIQ-SF was 19 (15–21) before treatment, which decreased to a median of 0 (0–5) after treatment (p = 0.01). The average preoperative pad use among the participants was 4 (3–6), while it became 0 postoperatively (p < 0.01). The median preoperative cystometric bladder capacity was 251 ml (100–350 ml), increasing to 456 ml (400–650 ml) postoperatively (p < 0.01). According to the Clavien-Dindo classification system, the majority of patients experienced either no complications (66%) or minor complications (CD I/CD II) (33%) within the initial 90 days following surgery.
Conclusions:
“Clam” iliocystoplasty emerges as a secure and successful treatment option in the patient group whose symptoms persist after first, second, and third-line treatments with the diagnosis of urge incontinence.
Introduction
Urge urinary incontinence (UUI) is defined as the involuntary leakage of urine, associated with a sudden compelling desire to void. 1 In women older than 30 years, the incidence is 30% and the incidence increases with age. 2 Notably, UUI is linked to heightened levels of depression and a diminished quality of life. 3 The initial approach to managing UUI involves behavioral interventions, encompassing techniques such as bladder training, pelvic floor muscle exercises, fluid regulation, and bladder control strategies, along with the possible integration of pharmacologic measures. 1 Second-line therapies are oral anti-muscarinic or oral β3-adrenoceptor agonists. 1 Notably, transdermal (TDS) oxybutynin (administered via patches or gel) can be a viable alternative. 4 Combination therapy with an anti-muscarinic and β3-adrenoceptor agonist can be used for patients resistant to monotherapy with anti-muscarinic or β3-adrenoceptor agonists. 5 Despite anticholinergics being a cornerstone of overactive bladder (OAB) treatment, their effectiveness varies, and poor compliance due to adverse effects, such as dry mouth, constipation, cardiac arrhythmias, and cognitive impairment, often compromises patient satisfaction. 6 Intradetrusor botulinum toxinA (100U), peripheral tibial nerve stimulation (PTNS) or sacral neuromodulation (SNS) can be applied as third-line therapy in carefully selected patients who refractory to first- and second-line OAB treatments. 1 There are studies comparing third-line treatment options, but their long-term efficacy and superiority over each other are not definitively accepted.7,8 In rare cases, augmentation cystoplasty or urinary diversion for severe, refractory, complicated OAB patients may be considered for forth-line therapy. 9
Clam augmentation enterocystoplasty was first described by Bramble in 1982 as a viable option for the treatment of severe urge incontinence. 2 There are no randomized prospective studies in the literature on Clam enterocystoplasty (CECP) but it can be safely applied in patients with neurogenic and non-neurogenic urge urinary incontinence according to studies with a limited number of case groups.10,11
In this study, our aim is to evaluate the efficacy of CECP surgery in the treatment of non-neurogenic refractory UUI.
Methods
Patient selection and evaluation
The data of 17 female patients who underwent CECP for non-neurogenic refractory UUI between May 2010 and November 2022 were evaluated retrospectively. All patients had written informed consent before operation. Age, comorbidities, body mass index (BMI), previous treatments for urge incontinence, operation time, duration of hospital stay, day of abdominal drain removal, day of urethral catheter removal, post-operative recovery day of bowel functions and follow up duration were recorded (Table 1). The Turkish version of The International Consultation on Incontinence Questionnaire-Urinary Incontinence Short Form (ICIQ-SF) was filled out in the preoperative and postoperative periods to evaluate their complaints and the number of pads used by patients daily were measured. 12 A 3-day voiding diary was evaluated for all patients pre-operatively. Diagnostic cystourethroscopy and urodynamic evaluation were conducted before CECP for all patients. Postoperative evaluations were conducted at 1, 3, 6 months, and every 6 months thereafter. Pre-operative cystometric bladder capacity was evaluated urodynamically. Postoperative urodynamic study was performed only on patients who needed it. Success was defined as complete continence without urine leakage and no pad usage.
Demographic features of patients.
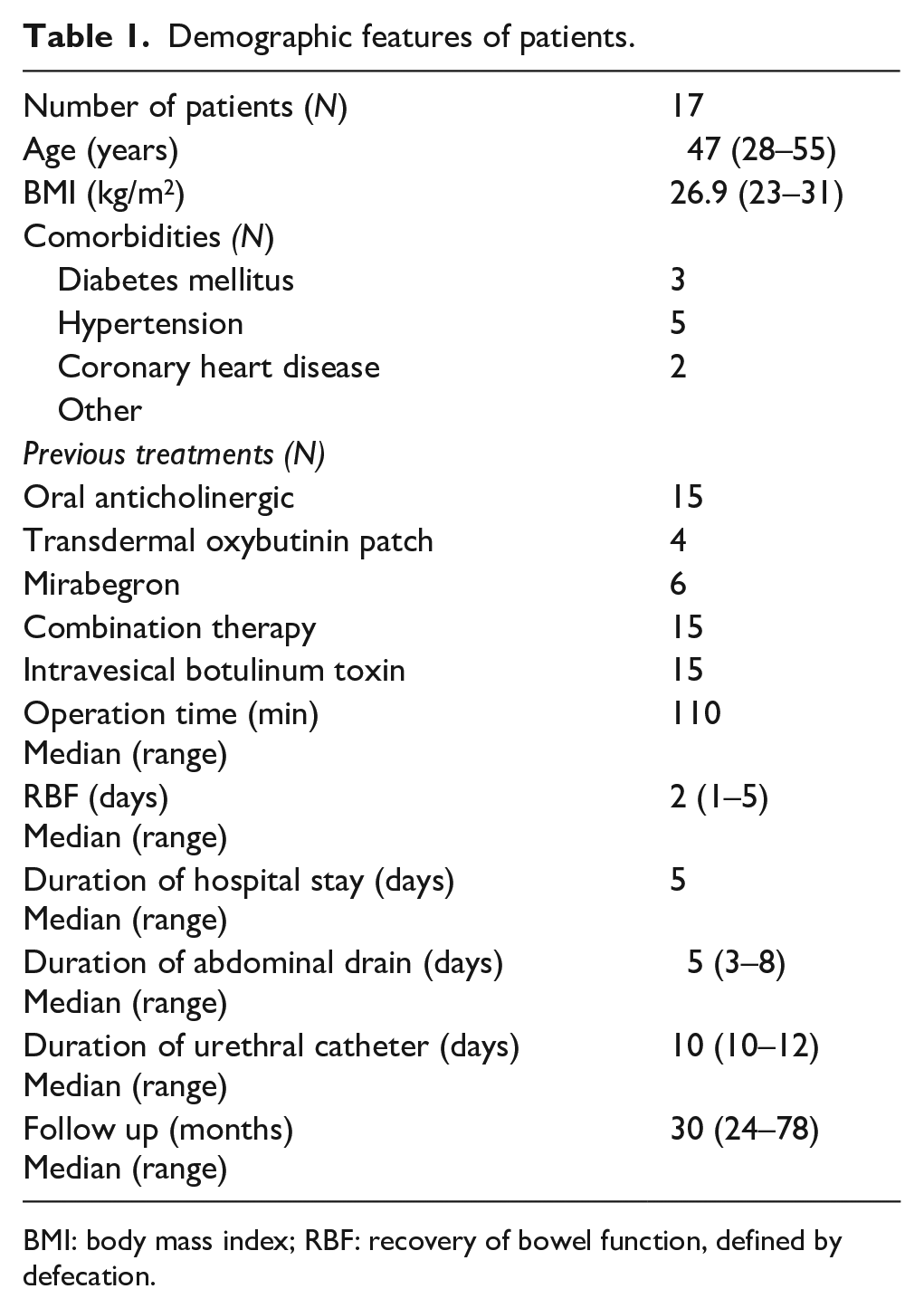
BMI: body mass index; RBF: recovery of bowel function, defined by defecation.
Exclusion and inclusion criterias
Patients who had undergone CECP for non-neurogenic refractory UUI were included in our study. Patients with neurogenic etiology were excluded from the study. Patients who have inadequate follow up are also excluded from our study.
Surgical technique
Prior to surgery, no bowel preparation was administered. A clear diet was implemented for 1 day. Prophylactic antibiotics (2 g ceftriaxone and 500 mg metronidazole) were given 1 h before anesthesia induction. The bladder was opened like a clam in the coronal plane along its maximal circumference, which is along the line of attachment of the fascial wing that attaches the bladder to the iliac vessels, from a point 1 to 2 cm in front of one ureteric orifice and about 2 cm from the bladder neck to a similar point on the other side. 13 A section used from 15 cm proximal of terminal ileum equal in length to the measured maximal circumference of the opened bladder is then isolated on its vascular pedicle, opened along its antimesenteric border to form a patch, triangulated at each end and sewn in place with one layer of continuous absorbable suture material (3/0 or 4/0 vicryl) (Figure 1). A suprapubic catheter was left in the bladder at the end of the procedure, clamped after 10 days to allow spontaneous voiding and removed when adequate emptying without undue frequency is established.
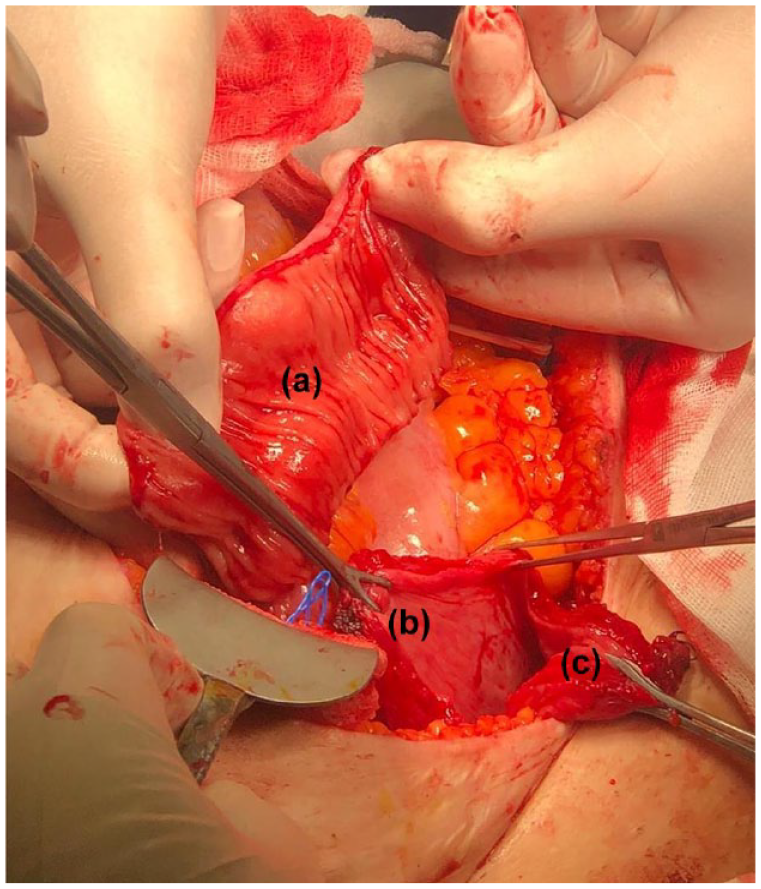
(a) Detubularized ileum segment, (b) posterior wall of bladder, and (c)anterior wall of bladder.
Statistical analyses
IBM SPSS Statistics Version 24 package program was used for statistical analysis. The conformity of the quantitative data to the normal distribution was evaluated with the Shapiro-Wilk test. Paired samples were given with the mean and standard deviation values by applying the T-test to evaluate the data that fit the normal distribution, while the Wilcoxon signed ranks test was used to evaluate the data that did not fit the normal distribution, along with the median, minimum and maximum values. p-Values were based on two-sided probability at a 5% significance.
Results
Seventeen female non-neurogenic refractory urinary incontinence UUI patients underwent CECP. In all cases, the ileum was used as a augmentation segment. Patients had a median age of 47 years (range: 28–55), with a mean body mass index was 26.9 (23–31). Three patients were diagnosed with type 2 diabetes mellitus. The median length of the operation was 110 min (95–150), and the median length of hospital stay after the operation was 5 days (4–7). Patients were followed up for a median duration of 36 months (range: 24–78). Demographic features of patients are summarized in Table 1.
The success rate of CECP was 80%. Median pre-operative cystometric bladder capacity was 251 ml (100–350 ml), while post-operative bladder capacity was 456 ml (400–650 ml). There was statistically significant difference between pre-operative and post-operative bladder capacity (p < 0.01). Additionally, there were statistically significant differences between pre-operative and post-operative ICIQ-SF scores and pad use. The median of ICIQ-SF was 19 (15–21) before treatment, and the median was 0 (0–5) after treatment (p = 0.01). The average pad use of the patients participating in our study was 4 (3–6) preoperatively, while it was 0 postoperatively (p < 0.01) (Table 2).
Evaluation of pre-operative and post-operative functional results.
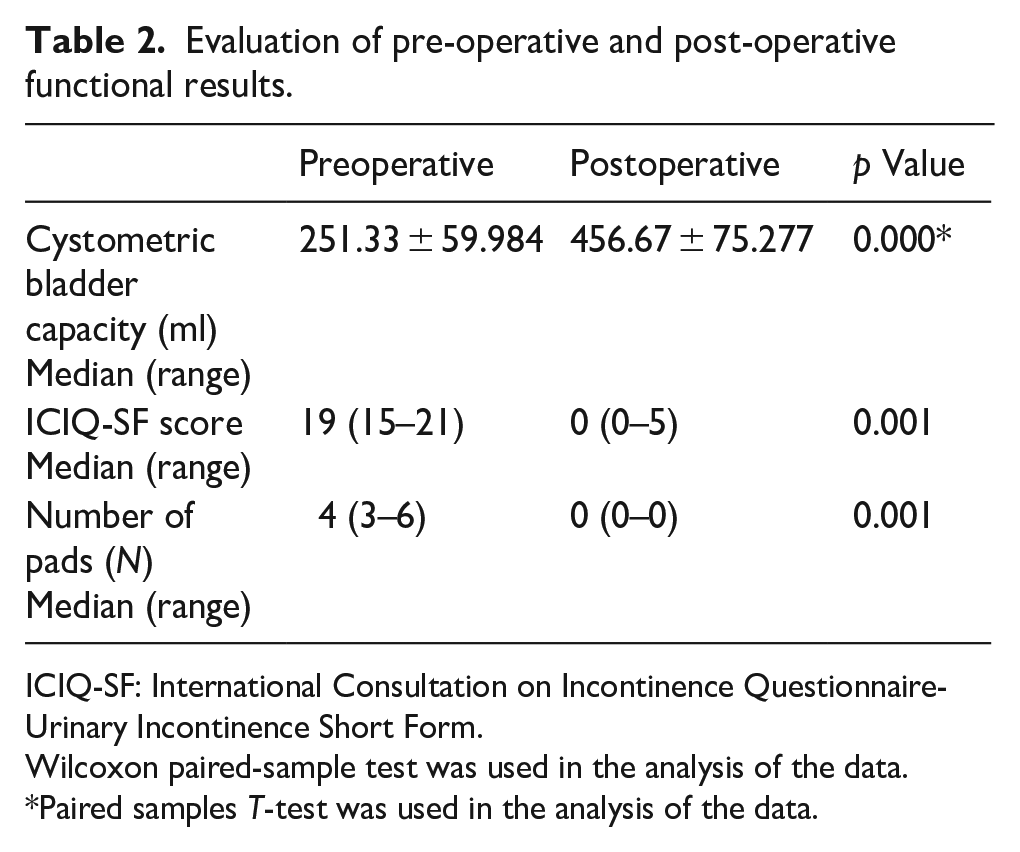
ICIQ-SF: International Consultation on Incontinence Questionnaire-Urinary Incontinence Short Form.
Wilcoxon paired-sample test was used in the analysis of the data.
Paired samples T-test was used in the analysis of the data.
No major complications were observed according to the Clavien-Dindo (CD) classification system within the initial 90 days post-surgery. The majority of patients experienced no complications (66%) or minor complications (CD I/CD II) (33%) during this period. In the follow-ups after catheter removal, incontinence was not observed in the patients. Post void residual measurements were performed, it was evaluated as <150 ml in all patients. Throughout the regular outpatient clinic follow-ups at postoperative 1, 3, 6 months, and every subsequent 6 months, no signs of urge incontinence, urgency symptoms, or symptomatic urinary tract infections were noted. During long-term follow-ups, there were 2 patients needed oral bicarbonate due to acidosis, no other metabolic complications were observed. Two patients required CISC (clean intermittent self-catheterization), and an additional patient diagnosed with bladder stones who also required CISC. No cases of perforation or cancer in the augmented bladder were detected. At the latest follow-up, three patients reported mild symptoms based on the ICIQ-SF. No patients experienced urinary tract infections requiring hospitalization.
Discussion
According to our long-term results, CECP is effective and safe procedure in non-neurogenic refractory UUI. The success rate for continence achieved through CECP was 82.3% in our study. Brandt et al. demonstrated that success rate of CECP in non-neurogenic refractory UUI was 64%. 11 In addition, Cetinel et al. reported 94% of non-neurogenic patients were fully continent after CECP. 14 The range of reported continent rates in the literature for non-neurogenic patients spans from 78% to 93%.15,16 These variations may stem from differences in the underlying etiology of non-neurogenic urge incontinence Notably, many existing studies lack validated questionnaires like the ICIQ-SF. In our study, the median ICIQ-SF score dropped significantly from 19 (15–21) before treatment to 0 (0–5) after treatment (p = 0.01). Additionally, literature often fails to comprehensively address pad usage. Our study revealed that the average pad usage decreased from 4 (3–6) preoperatively to 0 postoperatively (p < 0.01).
Meanwhile, the need for clean intermittent self-catheterization occurred in 2 (13%) of our patients due to clinically significant post-voiding residue. Brandt et al. found that 44% of their non-neurogenic group needed CISC after CECP. 11 Also, Cetinel et al. reported that 44% of their non-neurogenic group used CISC after CECP. 14 Other studies indicated that CISC is needed 6%–39% of patients who underwent augmentation cystoplasty for idiopathic detrusor over activity.16,17 When patients do not comply with CISC, bladder stones and a potentially fatal complication spontaneous bladder perforation may develop. It is important to inform patients in detail about the use of post-operative CISC and to confirm patient compliance.
The median bladder capacity was evaluated as 251.33 ± 59.984 ml on cystometric capacity. The median bladder capacity post CECP was 456.67 ± 75.277 ml. According to results, there was statistically significant difference between pre-operative and post-operative bladder capacity (p < 0.01). Brandt et al. reported that the mean bladder capacity increase was 269.5 ml. 11 Cheng et al. reported that overall increase in bladder capacity was 219 ml, but in this study only 57.5% of the Chinese patients had ileum as segment of choice, the rest had sigmoid or stomach. 18 Although increase in bladder capacity is seen in CECP, the primary aim is not to increase bladder capacity, but to treat urge incontinence and create augmented bladder without high PVR.
Bladder stone formation rates in augmented bladders range from 3% to 40%. 19 Ineffective emptying can lead to urinary stasis and an increased risk of stone formation. 20 Our study identified bladder stones in 1 (6.6%) patient who also required CISC due to high post-void residual volumes, aligning with the findings of Brandt et al. 11
Ileocystoplasty can lead to metabolic changes. Hyperchloraemic acidosis resulting from urinary ammonia reabsorption may necessitate oral bicarbonate treatment. We observed this condition in three of our patients (20%), in line with a study reporting a 16% incidence. 16 Additionally, Vitamin B12 deficiency is a potential outcome due to the use of the terminal ileum. 21 However, our approach of protecting the terminal ileum during surgery and using the 15 cm proximal section from the ileocecal valve for the augmented bladder likely contributed to our lack of observed cases.
Spontaneous bladder perforation has an incidence of 0.8%–13%,22,23 with higher risk among pediatric patient groups, possibly due to lower CISC compliance. While Brandt et al. reported a 2.5% incidence in adult patients, 11 our study did not encounter spontaneous bladder perforation, likely due to patient education on techniques like Valsalva and Crede maneuvers while voiding post-surgery.
The reported incidence of malignancy in augmented bladders is around 1% with a mean latency of 19–22 years.24,25 Despite the absence of malignancy development in our follow-up period, this may be influenced by the duration of the follow-up.
Limitations and strengths
Nevertheless, our study has some limitations. Firstly, this study is retrospective and has limited number of patients also we did not have a control group. This is limiting situation in terms of statistical significance. Secondly, because of its retrospective aspect, we didn’t compare CECP with other procedures and treatments used in urge incontinence. prospectively. CECP in patients with non-neurogenic etiology constitutes the strengths of the study due to the number of patients and long follow-up period.
In conclusion, “clam” enterocystoplasty proves to be a secure and effective option for patients whose symptoms persist through multiple treatment lines for urge incontinence. Comprehensive patient education on potential short-term and long-term complications is crucial. Larger prospective randomized trials are necessary to underscore the long-term results of CECP.
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.