
Abstract
Background:
The existence of β3 receptors in the bladder and ureter was documented in many studies on animals and humans, it was documented that relaxation of the lower ureteral segment is achieved by the stimulation of these receptors. Our aim was to assess the efficacy and safety of mirabegron as a medical expulsive therapy (MET) for distal ureteral stones in comparison with silodosin and placebo.
Methods:
One hundred eighty patients with distal ureteral stone of 5–10 mm size were included in our study. They were divided into three groups, and each one consisted of 60 patients. Group I was given silodosin 8 mg, group II mirabegron 50 mg and group III placebo once daily. The treatment was prescribed for all the cases till stone expulsion or a maximum duration of 4 weeks. Primary outcome was the stone expulsion rate (SER). While secondary outcomes were stone expulsion time, side effects of the used drugs, hospital visits number for pain, and amount of analgesic taken.
Results:
We found that the SER was significantly higher in silodosin than mirabegron and placebo groups (61%, 38.6%, and 36.7%, respectively) (p = 0.013). Also, the stone expulsion interval was significantly shorter in silodosin than mirabegron and control groups (p < 0.001). While hospital visits number for pain, and amount of analgesic taken were comparable. There was no difference between the studied medications in terms of the adverse effects except for retrograde ejaculation (silodosin = 63.3%, mirabegron = 0%, and placebo = 0%; p < 0.001).
Conclusion:
Mirabegron has no medical expulsive effect. While silodosin improves SER and stone expulsion time. However, retrograde ejaculation was its main side effect and occurred in 63.3% of the male patients. Therefore, more research is needed to discover a more tolerable MET.
Introduction
Urolithiasis is a common problem with a prevalence of 2%–3% in all populations. 1 About 20% of urinary tract stones are in the ureter. 2 and because almost all these patients are symptomatic, they require immediate assessment and pain killers. 3 According to the literature, more than 50% of the ureteral stones smaller than 10 mm pass spontaneously; this percent is higher in those smaller than 5 mm. 4 Spontaneous expulsion ratios (SER) rely mainly on stone size, site, anatomic structure, and ureteral spasm or edema. 5
Medication is used to reduce ureteral edema and spasm in order to enhance stone transit. Both medical expulsive therapy (MET) and nonsteroidal anti-inflammatory medications (NSAIDs) act to reduce ureteral edema and spasm. 6 MET usage has skyrocketed in recent years. Many drugs like calcium channel blockers, alpha-blockers, phosphodiesterase inhibitors, and antispasmodics have proven to be efficient in the management of urolithiasis. 7 MET works by relaxing the ureteral smooth muscle in order to enhance ureteric stone passage reducing the need for surgical procedures and save money. Also, it improves the results and the success rate of shockwave lithotripsy (SWL) and the symptoms of ureteral stents.2,3
However, alpha-blockers have many side effects as orthostatic hypotension, dizziness, nausea, and dry ejaculation due to their mechanism of action. From this point of view, research is ongoing to use a more tolerable drug with fewer complications. 8 The existence of β3 receptors in the bladder and ureter was documented in many studies on animals and humans, it was documented that relaxation of the lower ureteral segment is achieved by the stimulation of these receptors.9 –12 The aim of this study was to evaluate efficacy and safety of mirabegron as a medical expulsive therapy for distal ureteric stones in comparison with silodosin and placebo.
Methods
This was a prospective randomized study carried out between November 2022 and June 2023. It was approved by the ethics committee of our hospital (numbered M S 645/2022). All selected patients gave a written informed consent. Patients aged 18–60 years old complaining of a single radiopaque ureteral stone in the distal part (below the sacroiliac joint) and of 5–10 mm size were included. While patients with solitary kidney, bilateral ureteric stones, renal impairment, urinary tract infection (UTI), severe renal colic, pregnancy, severe hydronephrosis, uncontrolled hypertension, any urologic anomalies or previous history of ureteral surgery were excluded.
Sample size
In study by Hsu et al., we studied a continuous response variable from independent control and experimental subjects with one control(s) per experimental subject. 13 The response within each subject group was distributed normally with standard deviation of 5.5. If the true difference in the experimental and control means is 0.6, we will need to study each of the 54 experimental subjects and 54 control subjects to be able to reject the null hypothesis that the population means of the experimental and control groups are equal with probability(power) 0.08. The Type I error probability associated with this test of the null hypothesis is 0.05. The estimated lost to-follow-up rate was accepted at 10%; 60 patients per group were randomized.
One hundred eighty patients who fulfilled the inclusion criteria were randomly divided using computer generated method into three equal groups of 60 patients. Group I received silodosin 8 mg, group II mirabegron 50 mg, and group III placebo once daily (Figure 1). The treatment was continued until stone passage or maximally for 4 weeks. The workup for each patient was detailed history, physical examination, laboratory investigations (serum creatinine, urine analysis, urine culture, and complete blood count) and radiologic investigations (KUB = kidney, ureter and bladder X-ray, abdominal ultrasound, and NCCT = non-enhanced spiral CT). Stone size was measured as the longest dimension calculated on CT.
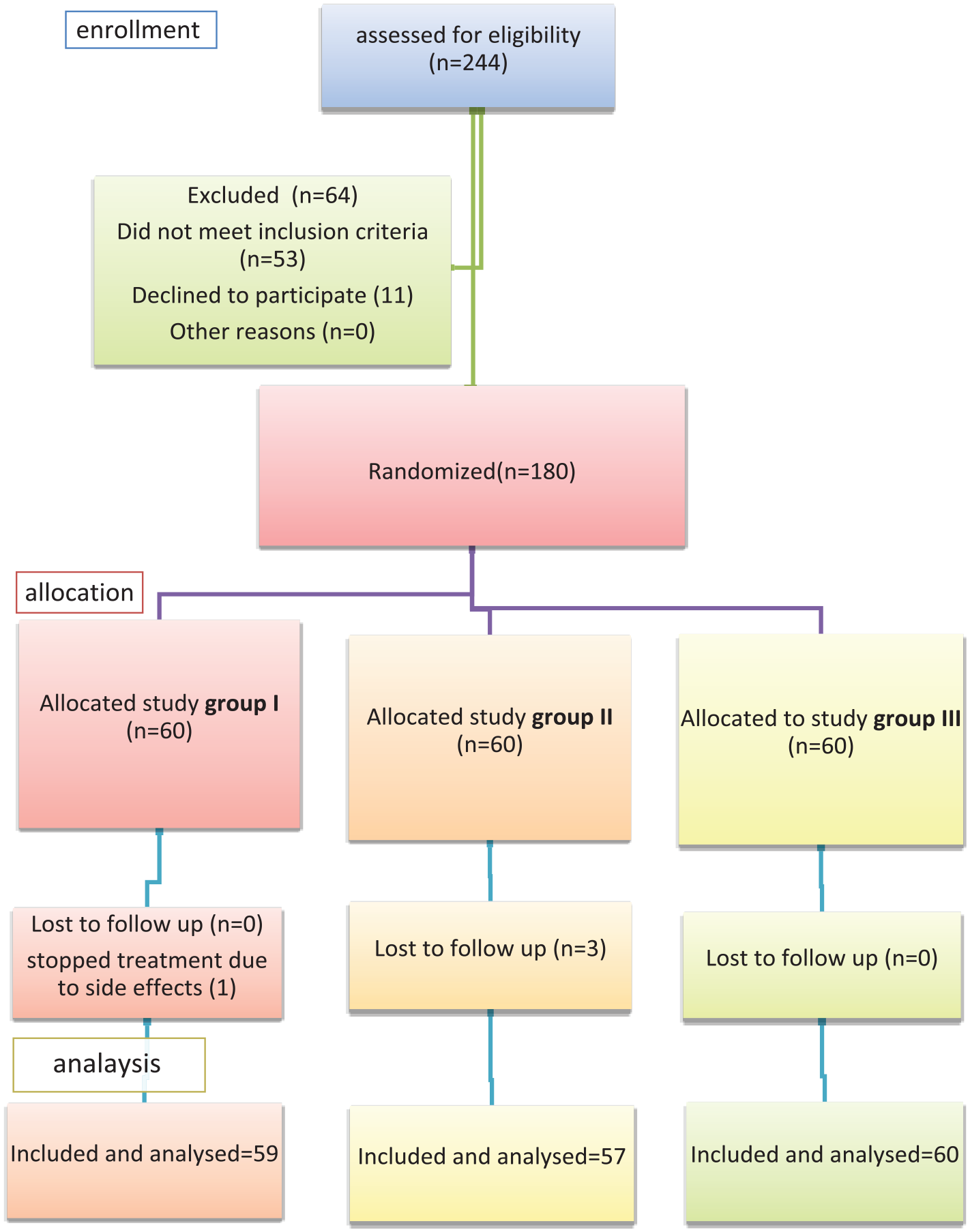
Consort flow chart.
Patients were instructed to take diclofenac 100 mg tablet as an on-demand analgesic. One tablet was counted as one dose. Patients were advised to strain their urine to search for any passed stones. All patients were informed to record their blood pressure measurements twice daily. The follow-up schedule was once every week included history-taking, blood pressure measurement, abdominal ultrasound and KUB (and NCCT if there was any doubt). The study was designed as a double-blind one. Primary outcome was the stone expulsion rate (SER). While, secondary outcomes were stone expulsion time, side effects due to the used drugs, hospital visits number for pain, and amount of analgesic taken.
Statistical analysis
Data was analyzed using Statistical Program for Social Science (SPSS) version 24. Quantitative data was presented as mean ± SD. Qualitative data was presented as frequency and percentage. One-way ANOVA test was used to compare between more than two means (for normally distributed data), while Kruskal Wallis test (KW) was used to compare between more than two means (for abnormally distributed data). Chi-square test was used to compare between non-parametric data. p-Value < 0.05 was considered significant.
Results
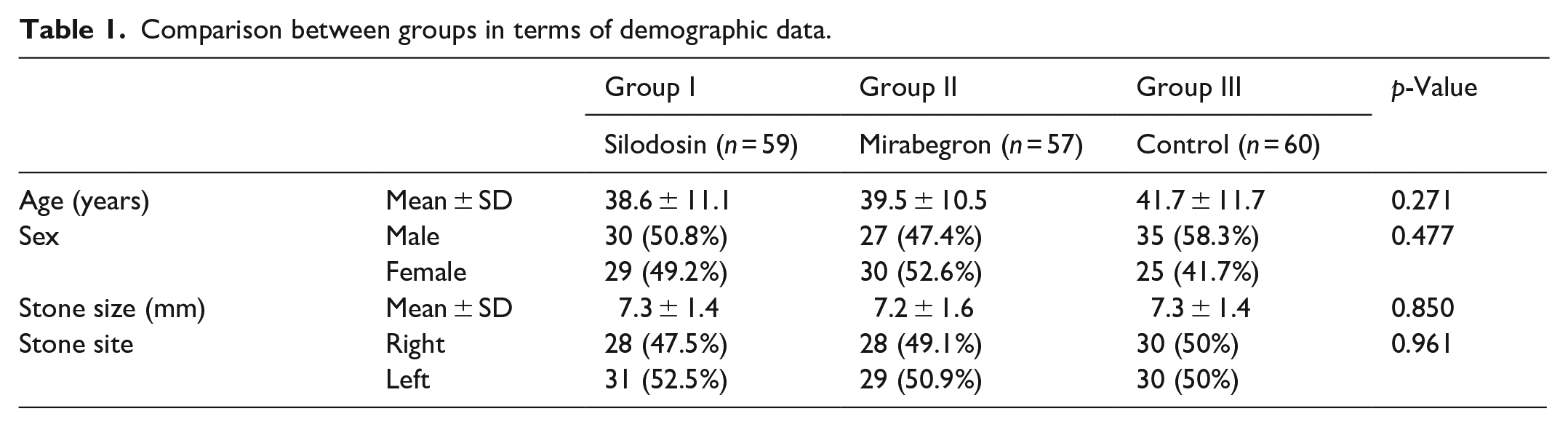
The demographic data was comparable in the three groups for age, sex, stone location, severity of hydronephrosis, and stone size (Table 1).
Comparison between groups in terms of demographic data.
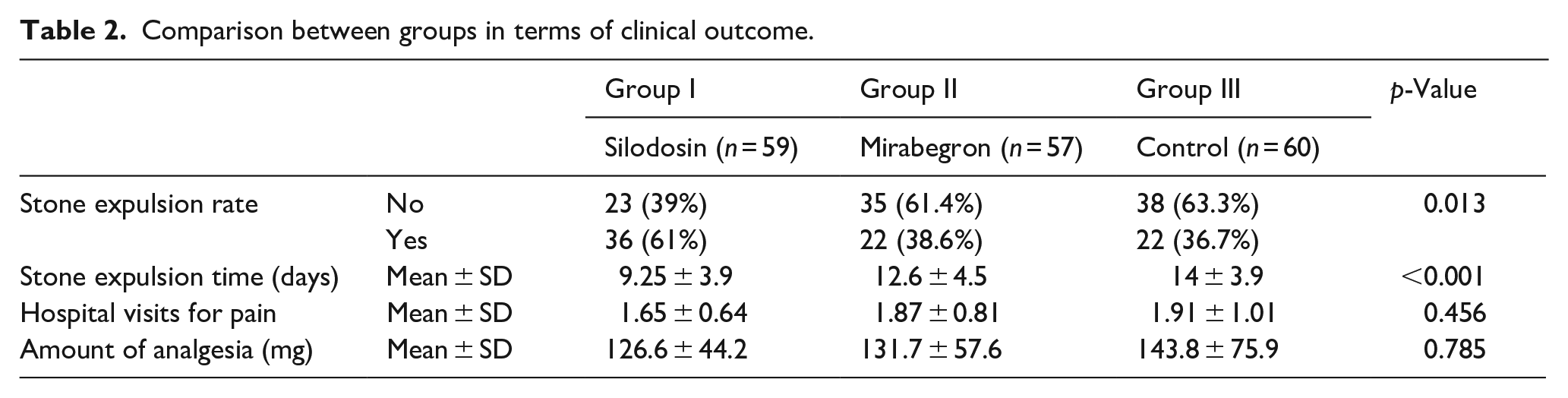
SER was significantly higher in silodosin than mirabegron and control groups (p = 0.013) and the stone expulsion interval was significantly shorter in silodosin than mirabegron and control groups (p < 0.001). While there was no significant difference between groups in terms of hospital visits for pain and amount of analgesia (Table 2).
Comparison between groups in terms of clinical outcome.
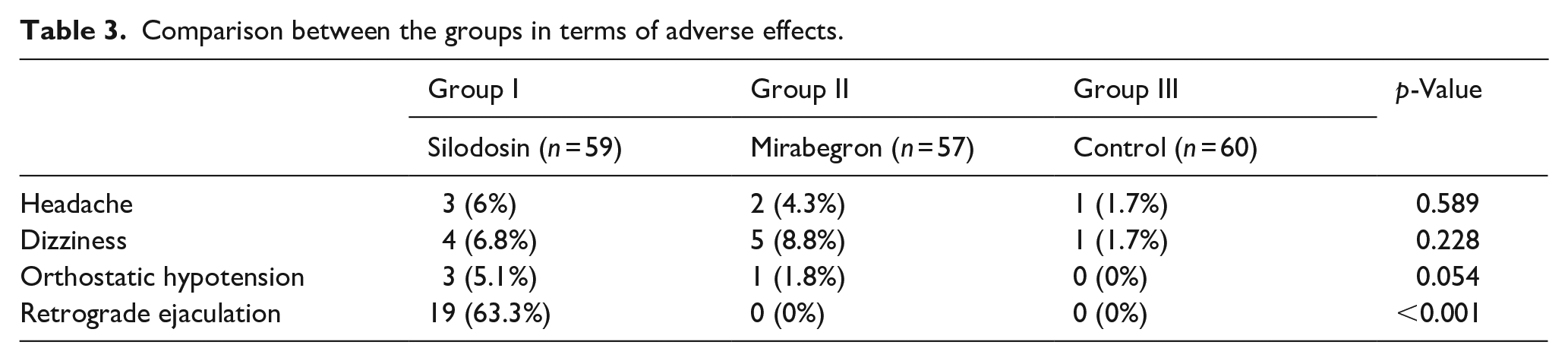
There was no significant difference between the three groups regarding headache, dizziness, and orthostatic hypotension. While retrograde ejaculation was significantly higher in silodosin than mirabegron and control groups (p < 0.001). No patients suffered from hypertension (Table 3).
Comparison between the groups in terms of adverse effects.
Discussion
The ureter has many alpha-adrenoceptors, the majority of which are found in the lower ureter. 14 These receptors are activated, resulting in ureteral spasm and contraction. 15 Alpha1-adrenoceptor subtypes mediate ureteral contraction by phenylephrine. 16 Silodosin, a highly selective alpha1a – adrenoceptor antagonist, is a regular component of MET for ureteral stones. 17
Relaxation is mediated by ß-2 and 3 adrenoceptors situated in the ureteral smooth muscle, and urothelium. 9 Any obstruction causing smooth muscle contraction decreases the density of ß-3 adrenoceptors, and this leads to more contraction and spasm. 6 Mirabegron was assessed by many investigators as a MET for ureteral stones with diverse results.6,18,19
In the present study, we found that the SER was significantly higher in silodosin than mirabegron and placebo groups (61%, 38.6%, and 36.7%, respectively; p = 0.013). Also, stone expulsion time was significantly shorter in silodosin than mirabegron and placebo groups. Similarly, Bayar et al., found that SER was higher in silodosin than mirabegron and placebo groups, however this difference wasn’t statistically significant. Also, they concluded that in patients with ureteric stones less than 6 mm, the stone expulsion time was significantly shorter in the silodosin than the control group and mirabegron didn’t affect the stone expulsion time. 6 In contrast, Solakhan et al., found that SER was 73.52% in the mirabegron group, and 47.05% in the control group (p = 0.026). While there was no statistically significant difference regards the stone expulsion time. 19
Beta-3 receptors number decreases with smooth muscle contraction by any form of obstruction. 6 We believe that this is the explanation for the absence of significant effect of mirabegron in comparison with silodosin and placebo regards SER and stone expulsion interval.
In terms of hospital visits for pain and amount of analgesia required, there was no significant difference between the studied groups. On the other hand, Tang et al. found that the occurrence of renal colic episodes was significantly lower in mirabegron than the tamsulosin group (1.3 ± 0.5 and 1.6 ± 0.7 respectively, p = 0.022) and less analgesia was needed. 18 Also, Bayar et al. concluded that the requirement of analgesia was less in the mirabegron than the control group (p = 0.017). 6 While some studies reported that silodosin use decreased the analgesic requirement more than the control.20,21
Side effects caused patients to stop treatment have occurred in only one patient in silodosin group and he was excluded from analysis. This small number can be explained by the fact that we have informed male patients that silodosin is expected to cause dry ejaculation. In our study, retrograde ejaculation was significantly higher in silodosin than mirabegron and control groups (p < 0.001). While there was no significant difference in occurrences of other side effects. In agreement with this, Solakhan et al. documented that nasopharyngitis happened in 1 (2.5%) patient, and hypertension another one (2.5%) in the mirabegron group. 19 Also, Tang et al. reported constipation in only one patient on mirabegron. 18 While, about 4%–15% of patients developed side effects from alpha blockers as MET.22,23
The current study had some limitations, including a small patient group and a brief follow-up time. Larger, multicenter prospective trials are needed to confirm our findings.
Conclusion
Mirabegron has no potential role as a MET for ureteric stones. Accordingly, further studies are required to discover a new medication that can improve stone expulsion and decrease pain with another mode of action and more tolerable adverse effects than silodosin .
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.