
Abstract
Introduction:
Bladder cancer is a common and serious disease globally, often requiring radical cystectomy as the preferred treatment. However, this procedure carries substantial risks and complications. To evaluate its success, pentafecta, a five-component measure, was introduced. This study investigates the attainment of pentafecta following radical cystectomy and examines factors that influence its achievement.
Methodology:
This retrospective, single-group study was conducted at AIIMS Jodhpur. The study population included 42 patients who underwent radical cystectomy for bladder cancer. Various data, including demographic characteristics, clinical features, surgical techniques, and postoperative outcomes, were collected from medical records. The primary outcome measure was the rate of achieving pentafecta, which comprises five parameters.
Results:
Out of 42 patients, 26 (61.9%) achieved pentafecta. Age, gender, comorbidities and surgical approach did not significantly affect the attainment of pentafecta. Negative surgical margins were achieved in 95.2% of cases, and adequate lymph node dissection (>16 lymph nodes) was performed in 85.7% of cases. The absence of Clavien-Dindo grade 3–5 complications and recurrence was observed in 80.9% and 90.47% of cases, respectively. Uretero-enteric stricture was absent in 95.2% of cases.
Conclusion:
The study emphasizes the significance of negative surgical margins, thorough lymph node dissection, absence of complications, recurrence, and uretero-enteric strictures in evaluating the success of radical cystectomy as pentafacta outcomes. Patients with higher drain output and wound infections are less likely to achieve pentafacta outcome and indicates poorer outcome. By considering these factors, clinicians can assess patient outcomes and identify areas for improvement.
Introduction
Bladder cancer is one of the most common malignancies worldwide, with an estimated 550,000 new cases 1 and 200,000 deaths annually. 2 It is the sixth most common cancer in men and the 17th in women. 3 Risk factors include smoking, exposure to certain chemicals, chronic bladder inflammation, and a family history of bladder cancer. 4 Bladder cancer treatment includes surgery like TURBT for non-muscle invasive bladder cancer (NMIBC) while radical cystectomy for muscle invasive bladder cancer (MIBC) and chemotherapy or radiation therapy may be used alone or in combination. 5 Radical cystectomy is the primary treatment for MIBC and high-risk NMIBC. 6 It involves removing the bladder, lymph nodes, and the prostate gland in men and bladder, lymph nodes and uterus in females to eliminate cancer cells and prevent spread. Radical cystectomy is a potentially curative treatment for bladder cancer, but it carries a high risk of complications and can impact quality of life. 7 While it can improve overall survival, it is a major surgery associated with risks such as bleeding, infection, and long-term side effects like erectile dysfunction.8,9 The success of radical cystectomy in bladder cancer is typically assessed based on 3-year recurrence-free survival (RFS) and 5-year overall survival (OS) rates. 10 However, standardized outcome criteria that consider both cancer management quality and surgical complications are needed. 11
The pentafecta outcome measure for radical prostatectomy includes five components: negative surgical margins, preservation of renal function and absence of significant surgical complications, recovery of urinary continence, and recovery of erectile function. The pentafecta outcome measure is a valuable tool for evaluating surgical outcomes, including quality of life, and identifying areas for improvement. 12 The concept of pentafecta was introduced originally by Aziz et al., 13 and further developed by Cacciamani et al. 14 in the context of RC. In present study pentafecta comprises five essential components, namely negative surgical margins, adequate lymph node dissection, no perioperative complications of Clavien-Dindo grade 3–5, absence of urinary diversion-related sequelae, and no recurrence of bladder cancer within 12 months after the surgery. This retrospective analysis examines outcomes of radical cystectomy using the pentafecta measure. It investigates factors influencing pentafecta achievement and aims to improve patient counseling and outcomes.
Methodology
Study design and setting
This is a retrospective, single-group study conducted at AIIMS Jodhpur to evaluate the rate of achieving the pentafecta in patients who underwent radical cystectomy in our newly established tertiary health care institute. The minimum follow up duration was 1 year.
Study population
The study population comprises 42 patients who underwent radical cystectomy at a newly established tertiary health care institute from 2016 to 2022. The inclusion criteria specify that the patients must have undergone radical cystectomy for histopathologically confirmed urinary bladder cancer during the study period and at least have completed follow up of 1 year after surgery. Additionally, complete medical records should be available for review. On the other hand, the exclusion criteria state that patients with incomplete medical records, a history of previous pelvic radiation therapy, or those who underwent partial cystectomy will be excluded from the study.
To gather the necessary data, a retrospective approach was employed, relying on the medical records of the included patients. Various types of data was collected, including demographic characteristics such as age and gender, clinical characteristics like BMI (Body Mass Index), comorbidities, and smoking status. Pathological characteristics such as tumor stage, grade, and lymph node involvement was also recorded. Surgical characteristics, including the type of radical cystectomy performed and the type of urinary diversion employed, was documented. Postoperative outcomes, such as postoperative complications like ileus, obstruction, wound infection, readmission rate, and length of follow-up, were also noted.
The primary outcome measure of the study is the rate of achieving the pentafecta in radical cystectomy patients. The pentafecta comprises five parameters: (1) negative surgical margins, (2) adequate lymph node dissection (defined as ⩾16 lymph nodes), (3) no perioperative complications of Clavien-Dindo grade 3–5, (4) absence of urinary diversion-related sequelae, and (5) no recurrence of bladder cancer within 12 months after the surgery.
Statistical analysis
The data was analyzed using appropriate statistical methods. Descriptive statistics were used to summarize the demographic, clinical, and pathological characteristics of the study population. The rate of achieving the pentafecta was calculated, and the association between patient characteristics and achieving the pentafecta was evaluated using logistic regression analysis. All statistical analyses were performed using a two-sided significance level of 0.05 (Table 1).
Socio-demographical and clinical variables .
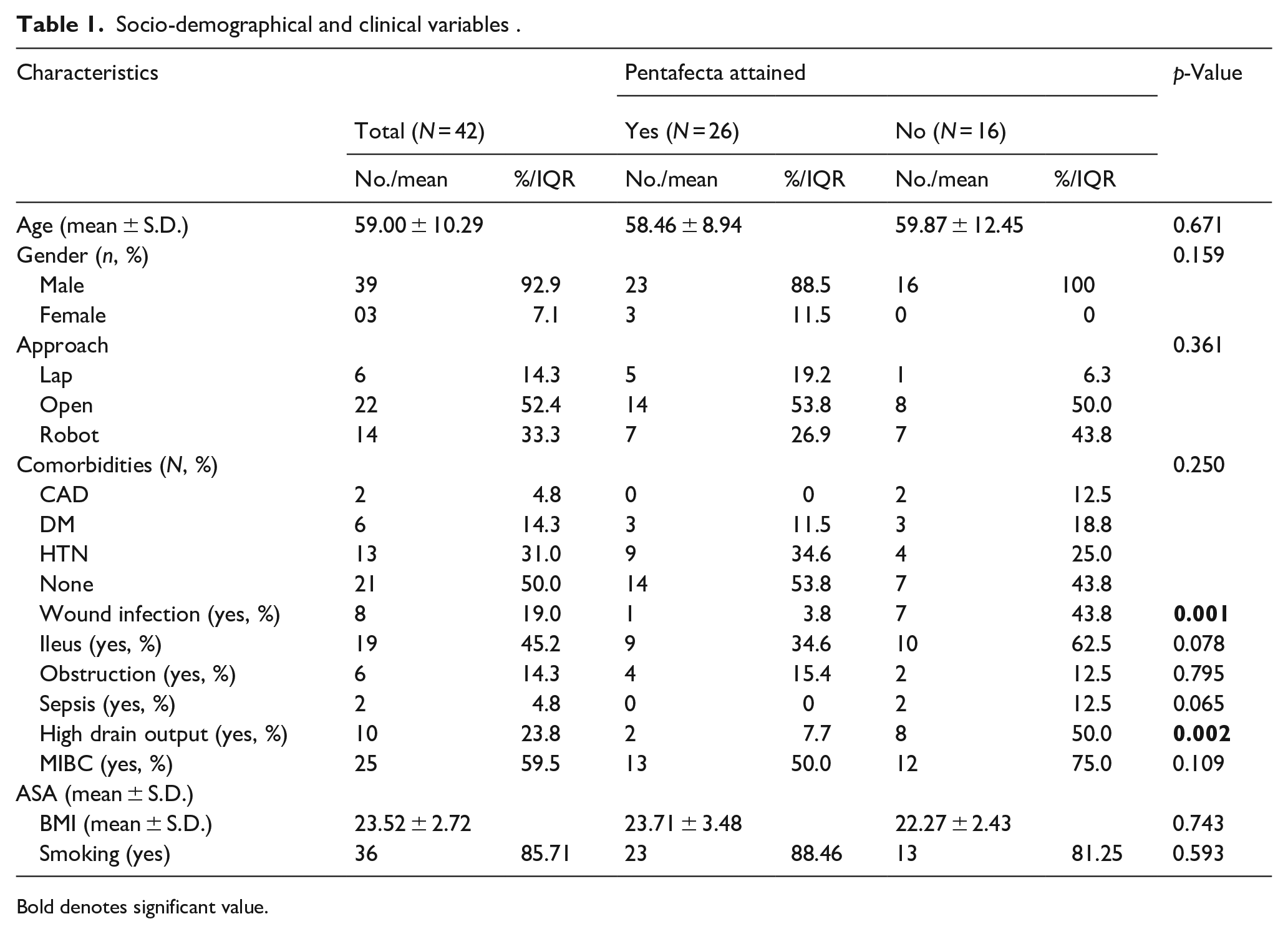
Bold denotes significant value.
Results
The total number of patients was 42, with 61.9% meeting the Pentafecta criteria. Age, gender, approach used for surgery (laparoscopic, open, or robotic), smoking status, BMI and comorbidities did not significantly differ between patients who met the criteria and those who did not. Patients who achieved the Pentafecta criteria had significantly lower rates of wound infection and low rate of High drain output (Table 1). Urine leak was excluded by doing drain fluid creatinine in patients of high drain output (>200 ml/day). Urine leak was included in failure of pentafecta achievement while high drain output was not as it was considered as Clavien-Dindo type 1 complication. Wound infections were managed using dressing and antibiotics and classified as Clavien -Dindo type 2. Post cystectomy lymphorrhea was the main cause of high drain output in these patients.
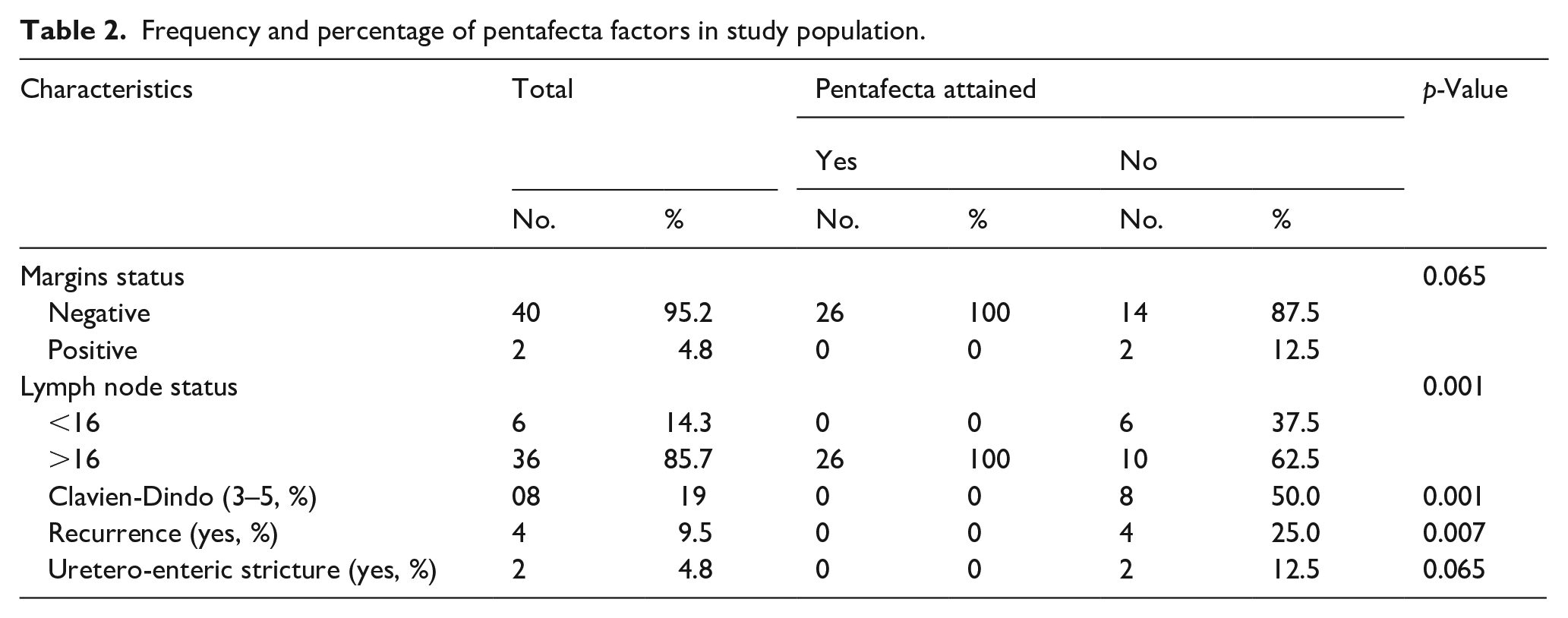
The p-value associated with margin status and Uretero-enteric stricture characteristic is 0.065 as shown in Table 2, indicating a moderate level of statistical significance. For lymph node status, Clavien-Dindo 3–5 classification, and recurrence, the difference in distribution is statistically significant, with a p-value of 0.001 (Table 3).
Frequency and percentage of pentafecta factors in study population.
Summary of pentafecta criteria achievement (N = 42).
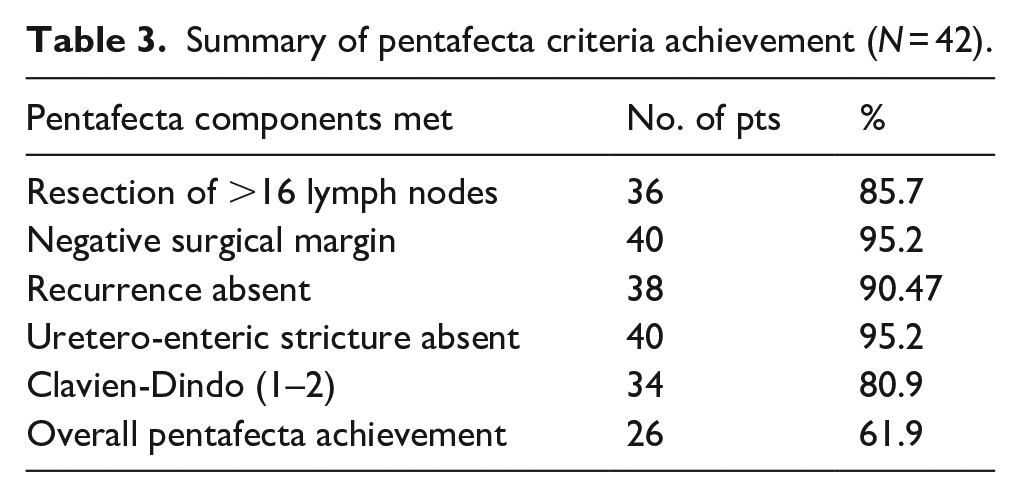
As shown in Table 3, the requirement for resection of more than 16 lymph nodes was fulfilled by 36 (85.7%) patients, 40 (95.2%) patients had negative surgical margins, 38 (90.47%) patients did not experience a recurrence, 40 patients (95.2%) were free from uretero-enteric stricture, 34 patients (80.9%) had Clavien-Dindo grades 1–2. Overall, 26 patients (61.9%) successfully achieved all five components of the pentafecta.
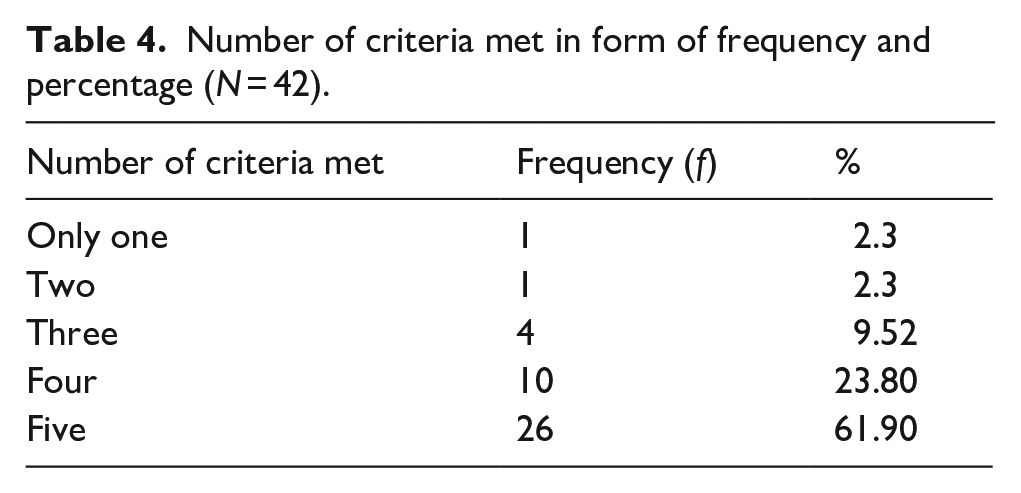
The pentafecta consists of five components, and the number of patients who met each criterion, as well as the corresponding percentages, are summarized in Table 4. Our data reveals that 2.3% patients met only one and two criterion, 9.52% patients met three criteria, 23.80% or 10 samples, met four criteria, 61.90% or 26 individuals, successfully met all five criteria.
Number of criteria met in form of frequency and percentage (N = 42).
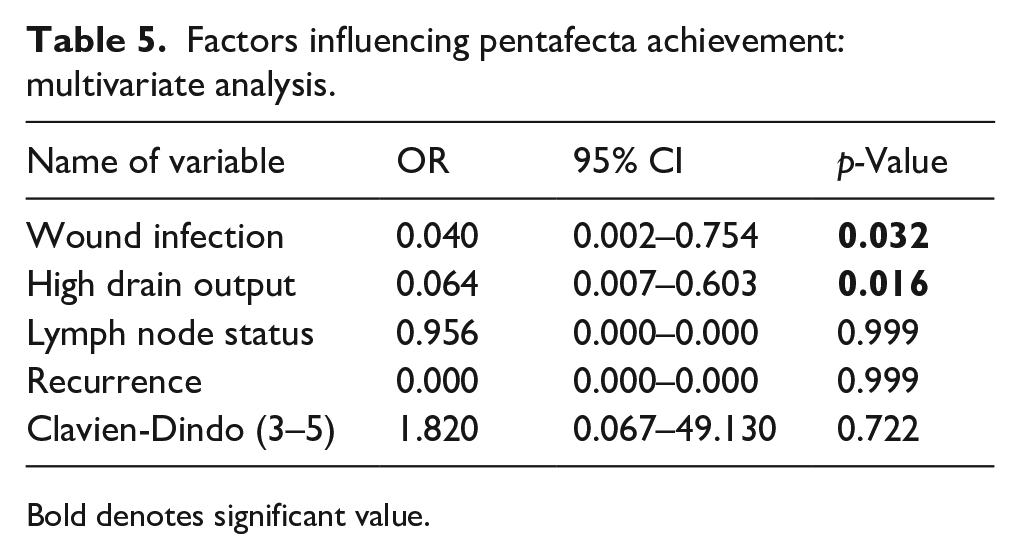
Those factors which were significantly associated with pentafecta achievement in univariate analysis, were analyzed by using multivariate analysis. The result of multivariate analysis is shown in Table 5. It shows that presence of wound infections and high drain output were found to be negatively associated with the successful attainment of the pentafecta. However, there was no evidence of recurrence impacting pentafecta achievement, nor was there a significant association observed with the Clavien-Dindo (3–5) classification and lymph node status on multivariate analysis.
Factors influencing pentafecta achievement: multivariate analysis.
Bold denotes significant value.
Discussion
The need for an adequate perioperative risk calculator for radical cystectomy (RC) in terms of both survival and morbidity is increasing. One suggestion is to refer patients to selected centers that can perform RC to improve the quality and outcomes of surgery. The concept of pentafecta may be useful for clinicians as well as patients. However, regionalization of bladder cancer surgeries may not be the best solution due to overload of cancer centers. The quality assessment using pentafecta may be an additional tool to improve the quality of care and operative morbidity. Other approaches have poor accuracy, and the concept of tri- and pentafecta models was proposed based on expert panel ranking of variables, with five commonly selected criteria forming the pentafecta. This idea was developed and modified by other researchers, analyzing it in various settings such as open or robotic approach, but mainly single-center data are available except for some papers. This study is a part of the evaluation process for assessing the quality of surgical procedures and the impact of the learning curve in onco-urology.
In terms of individual pentafecta components, our study showed a negative margin in 95.2% of patients. This finding is comparable to other studies, which have reported negative soft margin rates ranging from 97% to 100%.15 –19 Our study also demonstrated that ⩾16 lymph nodes were removed in 85.7% of patients, which is consistent with the minimum number of lymph nodes recommended and extended PLND template should be used to ensure comprehensive removal of the lymph nodes. It is important to note that the range of PLND is more critical than the total number of nodes resected. 20
In addition, our study showed that 80.9% of patients were major complication-free, which is similar to the 90% reported by Kang et al. 21 and 88.6% reported by Novara et al. 22 in their studies. Similarly, we found that 95.2% of patients were free from urinary diversion-related sequelae within 1 year, which is in line with previous studies reporting a rate of 96%. 23 Finally, our study revealed a clinical recurrence-free rate of 90.47% within 1 year, which is consistent with the rates reported in other studies.24,25
Based on our study, the main factors contributing to the reduced Pentafecta rate at our center were the number of removed lymph nodes and the rate of complications. Specifically, we found that a greater number of lymph nodes removed and a lower rate of complications were associated with a higher likelihood of achieving the Pentafecta. These findings are consistent with previous research that has shown that the number of lymph nodes removed is an important prognostic factor in bladder cancer, and that minimizing complications is crucial to achieving favorable surgical outcomes. 26
A study by Wu et al. found that achieving the Pentafecta was associated with a shorter length of hospital stay and a lower rate of intraoperative and postoperative complication. 27 Another study by Baron et al. reported that achieving the Pentafecta was more likely in patients undergoing intracorporeal urinary diversion than extracorporeal diversion, likely due to the reduced surgical trauma associated with the former approach. 28 In our study, patients who experience wound infections or have high drain output following radical cystectomy are less likely to achieve the desired outcome of RC-pentafecta more likely due to firstly, wound infections can delay wound healing and increase the risk of complications such as dehiscence (opening of the wound) or abscess formation and secondly, high drain output (such as excessive blood loss or lymphatic leakage) can be indicative of intraoperative complications or tissue damage.
Baron et al. proposed that the incorporation of other factors, such as LOH, readmission rates, or NAC usage, could increase the prognostic value of the pentafecta, possibly transforming it into a hepta- or octafecta tool. 28 However, it is yet to be determined which model – the tri-, pentafecta, or an enlarged model – is best suited for the clinical scenario of radical cystectomy. This knowledge is essential in guiding clinical decision-making and improving patient outcomes. Further research is needed to evaluate the benefits and limitations of incorporating additional factors into the existing models, and to identify the most accurate and clinically relevant prognostic model for patients undergoing radical cystectomy.
Our results demonstrate that the RC-pentafecta, as proposed by Cacciamani et al. 14 can be replicated in a Indian cohort of patients who underwent RC for bladder cancer in a newly developed tertiary health care center . Furthermore, our findings indicate that the validation of the RC-pentafecta improves with the surgeon’s experience.
Limitation
There were several limitations to our study that should be considered. Firstly, due to its retrospective nature, some data were missing. Secondly, to meet the RC-pentafecta definition, patients with less than 12 months of follow-up were excluded, resulting in a low number of included patients. This limited our ability to confirm the superiority of the pentafecta on survival and the significance of certain data in the multivariate analysis.
Conclusion
Achievement of Pentafacta outcome after radical cystectomy at new tertiary care center is comparable with high volume center. Wound infections and high drain output are associated with failure of achievement of pentafacta. Improvement in strategies to decrease these complications can improve the outcome.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.