
Abstract
Introduction:
Interstitial cystitis/bladder pain syndrome (IC/BPS) is a chronic painful bladder condition characterized by pelvic pain and urinary symptoms without another identifiable cause. Cystoscopy as primary initial investigation for IC/BPS has not been accepted yet and needs more studies to definitely conclude.
Aims and objectives:
We aimed to assess cystoscopy findings in patients of interstitial cystitis/bladder pain syndrome and to prove role of cystoscopy as primary initial investigation for interstitial cystitis/bladder pain syndrome.
Materials and methods:
Our prospective observational study included 35 female patients aged 18–69 years presenting to the Urology OPD at SMS Hospital with suprapubic or pelvic pain for 6 months, bladder pain that worsens with bladder filling and reduced with voiding, dysuria, urinary frequency and urgency, nocturia, dyspareunia. Those with history of bladder capacity more than 350 ml, duration of symptoms less than 6 months, day time frequency less than eight times per day, diagnosis of bacterial cystitis or prostatitis, bladder or ureteral calculi, active genital herpes, any existing urological malignancy, radiation cystitis were excluded from the study. They were then subject to cystoscopy and the findings of the cystoscopy were analyzed.
Results:
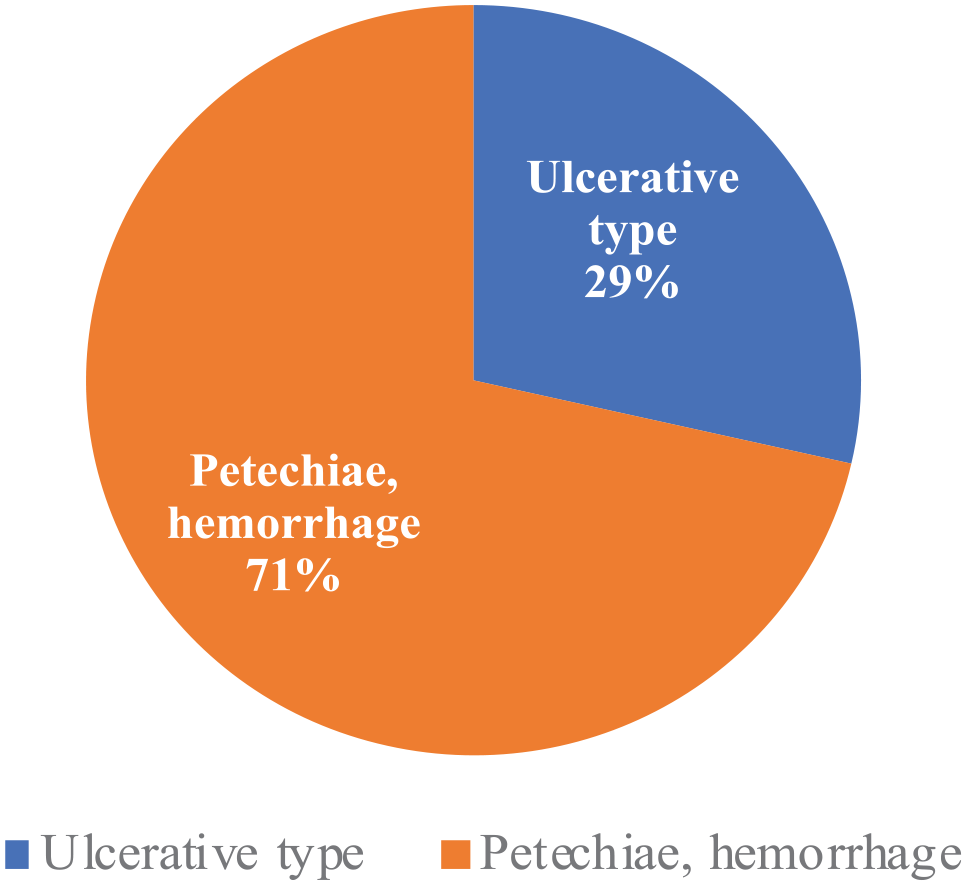
Out of the 35 patients, 11 (31.43%) had a normal cystoscopy. Of the 24 patients (68.57%) who had a positive cystoscopy, cystoscopy in seven patients (20.0%) revealed an ulcer. All these seven patients underwent fulguration. In the remaining 17 patients the abnormal findings were petechiae, large submucosal bleed. The sensitivity of cystoscopy in detecting the ulcerative type of Interstitial cystitis was found to be 20.0%.
Conclusion:
Our study found that Cystoscopy, if employed in initial investigation can help early detection of ulcerative variety of IC/BPS and can act as therapeutic modality by using fulguration plus hydrodistension. Larger comparative studies are needed for diagnostic/Therapeutic value of cystoscopy.
Introduction
Interstitial is characterized by chronic inflammation of the urinary bladder due to non-infectious etiology. In many cases, because it remains a diagnosis of exclusion, the condition is often diagnosed late in the patient’s journey. Patients often describe suprapubic pain, with urinary urgency. This sensation is worsened by filling the bladder and is often relieved by frequent passage of urine. This may be during the daytime and/or during the night (nocturia). There may also be other symptoms such as dysuria and dyspareunia. 1
Based on a large population, questionnaire-based, prevalence study in the US, 2.7% of women meet the specified criteria, with 1.9% of men meeting the criteria.2,3 In terms of age groups, women between 50 and 59 and men between 56 and 74 years of age. However, a lower prevalence is seen when physician-completed questionnaires and histological samples were employed to establish a diagnosis. A study in the Netherlands quoting as low as between 8 and 16 out of 100,000 individuals. 4 Investigations have noted a female predisposition, with one study in the US quoting a 5–1 ratio. 5 As this is a diagnosis of exclusion, a detailed medical history and physical examination are necessary to rule out other conditions that may present with similar symptoms. 1
The role of cystoscopy in the diagnosis and classification of IC/BPS has long been a matter of debate, with some authorities such as the European Society for the Study of Interstitial Cystitis (ESSIC) indicating cystoscopy as a diagnostic prerequisite, whereas some others, such as the American Urological Association (AUA) reserve it for complex cases. 6
The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) established cystoscopic discovery of glomerulations or Hunner lesions as an unchallenged diagnostic criterion for IC/BPS. 7 However, NIDDK criteria were used mainly for the purpose of standardization in scientific studies and the strict application of these criteria would miss a significant proportion of patients who actually have IC/BPS. 8 Many experts agreed that the absence of glomerulations or Hunner lesions did not rule out IC/BPS. 9
Cystoscopy appearance of lesions is very similar to malignancy, particularly carcinoma in situ. During visualization of the distended bladder, there may be Hunner’s ulcers, which are often described as a pale central scar with or without a fibrin clot and surrounded erythematous mucosa, with small vessels radiating toward the center. It is specific in the diagnosis of interstitial cystitis. However, it is not common even in patients suffering from it, with some studies describing only between 5% and 10% being present. 10
Reactive hemorrhages are also a sign of interstitial cystitis. This is when on initial examination under cystoscopy, the mucosa appears normal (distended). Still, when deflated and re-inspected, points of capillary bleeding are noted on a background of normal mucosa. 10
The AUA recommends low-pressure hydrodistension for a short period, or if Hunner lesions are present, treat using direct fulguration through diathermy or laser, and/or injection of steroid, for example, triamcinolone. 11
The ESSIC proposal highlighted the importance of excluding confusable diseases (such as carcinoma in situ) as the cause of symptoms and indicated cystoscopy under anesthesia with hydrodistension (HD) and eventual biopsy as a diagnostic prerequisite. 12 Furthermore, cystoscopic and histopathologic findings would enable further documentation and classification of IC/BPS. 12 The European Association of Urology (EAU) 13 and the Japanese Urological Association guidelines, 14 conjoint expert opinions from East Asia, 15 and the Bladder Pain Syndrome Committee of the International Consultation on Incontinence 16 follow the recommendations of the ESSIC. Conversely, the AUA guidelines do not indicate cystoscopy as an integral part of the initial diagnostic evaluation for IC/BPS. 17
We aimed to assess role of cystoscopy as primary initial investigation for interstitial cystitis/bladder pain syndrome and to assess cystoscopic findings in patients of interstitial cystitis.
Materials and methods
Inclusion criteria
Our prospective observational study included 35 female patients aged 18–69 years presenting to the Urology OPD at SMS Hospital with suprapubic or pelvic pain for 6 months, bladder pain that worsens with bladder filling and reduced with voiding, dysuria, urinary frequency and urgency, nocturia, dyspareunia.
Exclusion criteria
Those with history of bladder capacity more than 350 ml, duration of symptoms less than 6 months, day-time frequency less than eight times per day, diagnosis of bacterial cystitis or prostatitis, bladder or ureteral calculi, active genital herpes, any existing urological malignancy, radiation cystitis were excluded from the study.
A detailed medical history of present illness and past illness was obtained for all patients suspected of interstitial cystitis. Complete blood count, renal function tests(serum urea and creatinine) and urine examination was done for all patients. Subsequently all patient urine samples were also sent for urine culture and sensitivity.
The final sample size was 35 patients with the clinical diagnosis of interstitial cystitis.
These included patients were then subject to cystoscopy and the findings of the cystoscopy were analyzed. Hydrodistension and fulguration was performed for patients with mucosal disruption.
Results
All patients were female. The patients’ age ranged from 18 to 69. Most of them were middle aged and the mean age was 46.8 years and median was 47.5 years.
Mean bladder volume was 169 ml and the median value was 150 ml. Renal function of all the patients was within normal limits.
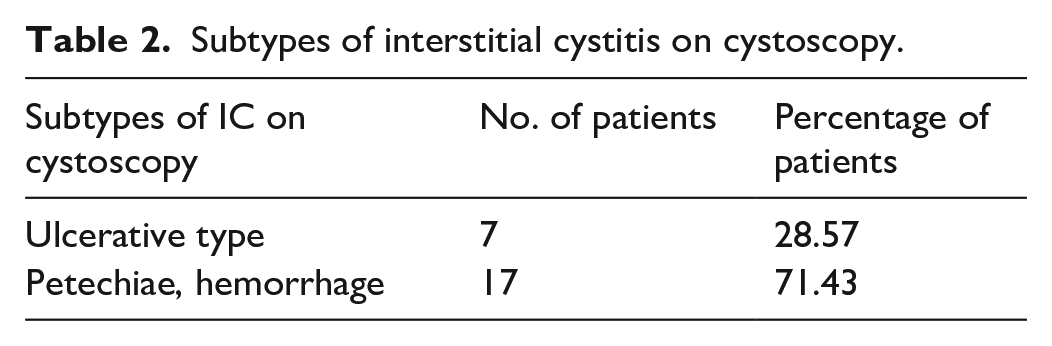
Out of the 35 patients, 11 (31.43%) had a normal cystoscopy (Figure 1 and Table 1). Of the 24 patients (68.57%) with positive cystoscopy, cystoscopy in seven patients (20%) revealed an ulcer. All these seven patients underwent fulguration. In the remaining 17 patients the abnormal findings were petechiae in at least two quadrants and large submucosal bleed (Figure 2 and Table 2).
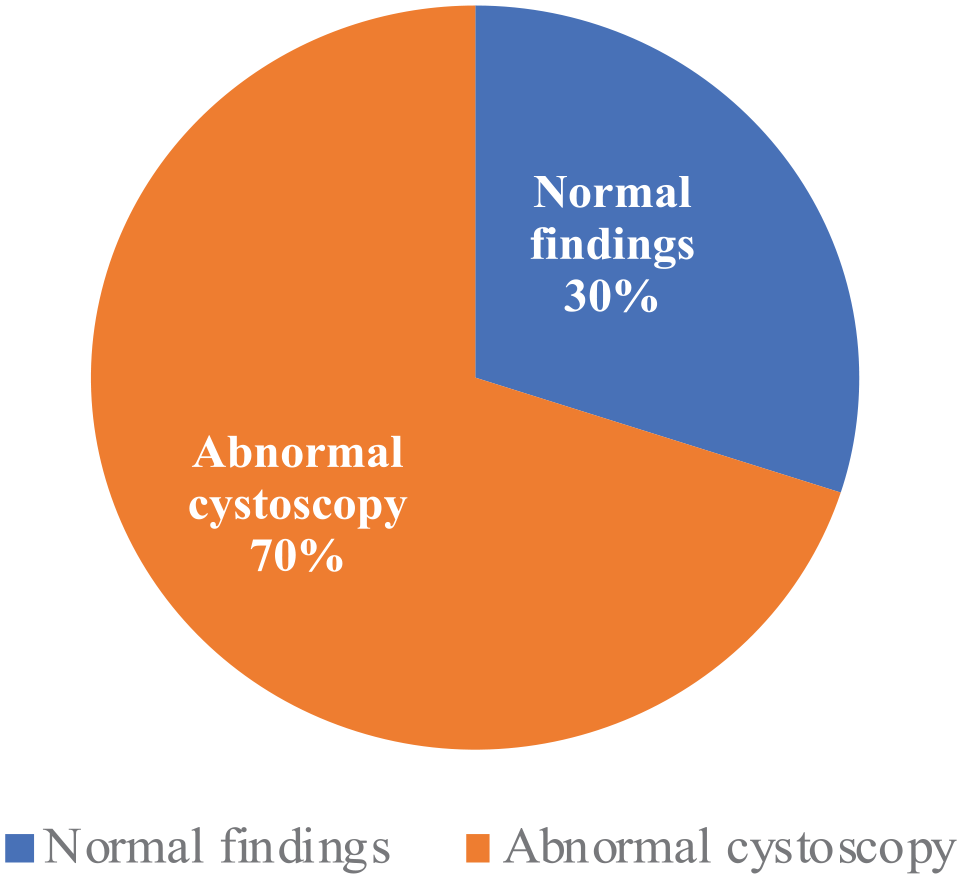
Findings on cystoscopy.
Findings on cystoscopy.
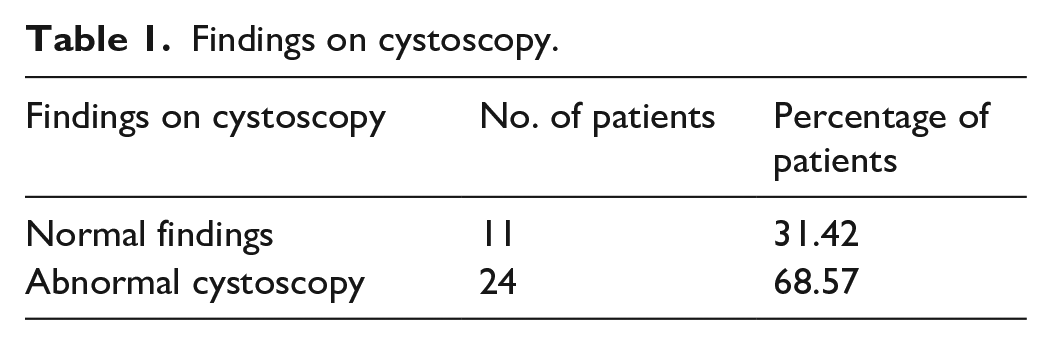
Subtypes of Interstitial cystitis on cystoscopy.
Subtypes of interstitial cystitis on cystoscopy.
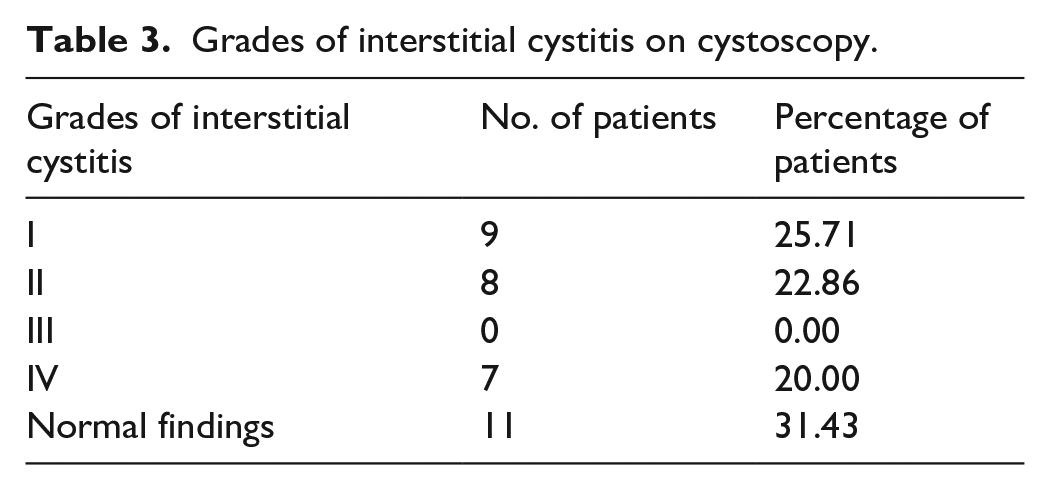
Grade I findings (petechiae in at least two quadrants) were observed in nine patients, Grade II findings (large submucosal bleed) were observed in eight patients, none of the patients had Grade III findings and seven had Grade IV findings (mucosal disruption, ulcer) (Figure 3 and Table 3).
The sensitivity of cystoscopy in detecting the ulcerative type of Interstitial cystitis was found to be 20%.
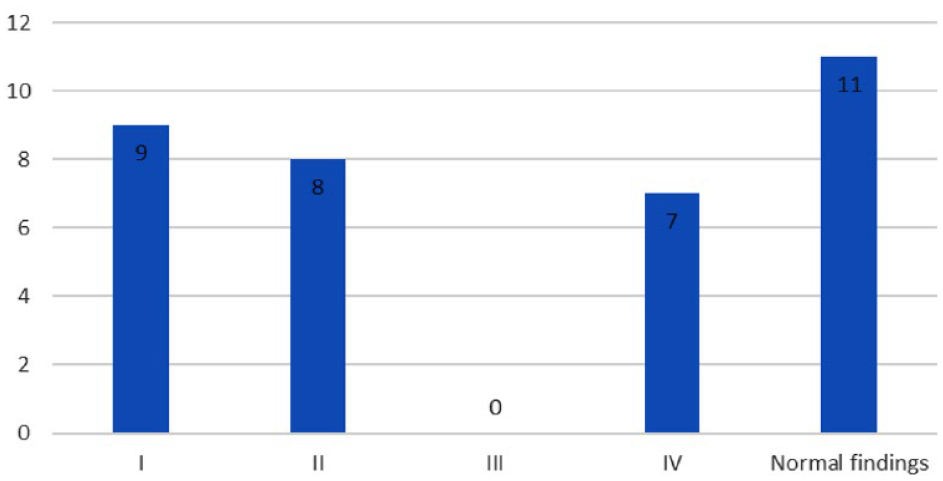
Grades of interstitial cystitis.
Grades of interstitial cystitis on cystoscopy.
Discussion
We noted grade II findings in 22.86% of the IC patients.
We did not note any case with Grade III findings. Meanwhile Chen et al. 19 found grade III findings in 44.2% of the patients.
Our study found ulcers in 7 out of 35 patients (20%). Meanwhile Aihara et al. 18 who also included 30 patients in their study, found glomerulations in 23 patients and two had Hunner’s ulcers. Chen et al. 19 on the other hand found 55.76% of the patients showing Hunner’s ulcers. Such vast differences in the grading percentages across the studies may be reflective of the generally small sample size of these studies that is prone to result in varying percentages. They may also indicate the difference in risk factors across the regional distribution of these studies, including ours. It may also be due to the differences in the clinical practices and the fact that this is a diagnosis of exclusion makes for a diagnostic number that is heavily dependent on the ability of the centers to rule out other causes of cystitis.
We found that cystoscopy was sensitive (20%) in detecting ulcerative type of the interstitial cystitis. On the contrary, Ottem and Teichman 20 reported that cystoscopy with hydrodistension provided little useful information above and beyond the history and physical examination findings.
Conclusion
Cystoscopy when done in a patient with clinical suspicion of interstitial cystitis can detect about 20% of the cases of ulcerative type which offers immediate relief upon hydrodistension and fulguration. Therefore, when done in those with clinical suspicion in an early stage, the cystoscopy might yield a higher sensitivity. Larger studies comparing the diagnostic value of cystoscopy and those evaluating the impact of earlier use of cystoscopy guided interventions are needed.
Footnotes
Acknowledgements
We would like to express our special thanks of gratitude to our patients and staff in Urology Department, SMS Medical College.
Author contributions
Dr Angadjot Singh, Post-Doctoral Trainee – Conception, Design, Materials, Data collection and processing, Analysis and interpretation, Writing. Dr Shivam Priyadarshi, Senior Professor and Head of Department– Design, Supervision, Analysis and Interpretation, Writing, critical review. Dr Somendra Bansal, Assistant professor– Design, Supervision, Analysis and Interpretation, Writing, critical review. Dr Sanyam Nandwani, Post-Doctoral Trainee – Conception, Design, Materials, Data collection and processing, Analysis and interpretation, Writing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics committee approval
Approved by Institutional Ethics Committee
• Institute name – SMS Medical College, Jaipur, Rajasthan, India
• Approval number – 288 MC/EC/2022
Patient consent
Obtained.