
Abstract
Background:
To investigate urodynamic abnormalities associated with vesicoureteral reflux (VUR) in toilet-trained children.
Methods:
The data of 157 children who were diagnosed with vesicoureteral reflux and referred to our hospital between 2013 and 2022 were retrospectively examined. The urodynamic parameters were analyzed and correlated with age, gender, lower urinary tract symptoms (LUTS), reflux severity, and laterality.
Results:
Overall, 131 (83.4%) patients had abnormal urodynamic findings with a male-to-female ratio of 1:1.4. The most common pathological finding was detrusor overactivity (DO), identified in 101 (64.3%) patients, followed by dysfunctional voiding (DV) in 74 (50.3%) patients. Children with VUR grades II and III exhibited a greater percentage of abnormal urodynamic findings than children with grades IV and V. The prevalence of DO was higher in children younger than 10 years old with unilateral and lower-grade VURs. DV was more frequent in children older than 10 years, with bilateral VUR, and higher grade VUR. The prevalence of LUTS, bowel and bladder dysfunction (BBD), and urinary tract infection (UTI) was higher among children with abnormal urodynamic findings.
Conclusions:
Children with VUR have a high incidence of urodynamic disorders. Urodynamic dysfunction may contribute to the pathogenesis of VUR, especially in mild cases.
Introduction
Vesicoureteral reflux (VUR) is a complex disease as its presentation is variable. Affected patients may suffer from recurrent afebrile and febrile urinary tract infections (UTIs) that leave renal parenchymal scars in some cases. 1 Several factors play an important role in the adverse effects of VUR on the kidneys, including the grade of VUR, detrusor pressure, and dysfunctional voiding.2,3
It has long been recognized that vesicoureteral reflux and bladder dysfunction are inextricably linked. In a VUR population, bladder dysfunction is reported to be prevalent at various rates. According to the results of invasive urodynamic studies (UDS), higher figures of bladder dysfunction (38%–75%) were found compared to what was observed when questionnaires were used (18%–52%). 4
Studies have shown that voiding phase abnormalities contribute to a lower rate of spontaneous resolution of VUR.5 –8 In addition, abnormalities in the filling phase, such as involuntary detrusor contraction, may cause VUR even without dysfunctional voiding. Undiagnosed and untreated lower urinary tract dysfunction (LUTD) is a significant cause of surgical failure. 9 It has been shown that the cure rates of VUR following endoscopic treatment are lower in children with bladder bowel dysfunction, but there are no differences observed following open surgery for children with bladder bowel dysfunction. 7
History taking and physical examination are the hallmark diagnostic tools for the evaluation of LUTD in children. However, UDS can also help to confirm the diagnosis of different LUTD in toilet-trained children. 10
This study aims to evaluate the incidence and type of urodynamic dysfunction associated with VUR severity and age to further define the relationship between VUR and urodynamic dysfunction.
Materials and methods
This retrospective study was conducted on 157 children diagnosed with primary VUR who were referred to the UDS center at Labbafinejad Hospital (Tehran, Iran) during the period 2013–2022.
A questionnaire was used to collect all clinical information, including bladder and bowel habits 11 ; voiding dysfunction history; past medical and surgical histories; and imaging studies. An experienced urologist (F.S.) performed a detailed clinical history and a UDS.
Study participants were neurologically intact children between 5 and 18 years. Exclusion criteria were: urogenital anomalies (meatal stenosis, labial adhesion, ureterocele, posterior urethral valves); neurological disorders (cognitive disorders; spinal cord dysraphism), use of anti-muscarinic or muscle relaxant drugs or alpha-blockers in recent time.
Urinary tract infections were treated promptly with antibiotics, followed by prophylactic low-dose antibiotics and UDS was performed after two negative urine cultures at an interval of 2 weeks.
VUR was diagnosed by voiding cystourethrography, and severity was determined according to the International Reflux Study classification. 12
A diagnosis of bladder and bowel dysfunction (BBD) was characterized by having any lower urinary tract symptoms (LUTS) according to ICCS along with fecal elimination problems, which manifested primarily as constipation and/or encopresis.13,14
All patients underwent UDS according to a standardized protocol, which was developed by following the UDS guidelines of the International Continence Society (ICS). UDS was used to determine bladder capacity, bladder compliance, detrusor overactivity (DO), urinary leakage, and the number and amplitude of DOs in the filling phase. Voiding pressure at the maximum flow rate (Qmax), voiding pattern, electromyography (EMG), and post-void residual volume (PVR) were assessed in the voiding phase.15,16
A Medical Measurement Systems urodynamic machine was used for the entire study group. A 5-F Double P-lumen urodynamic catheter was used for saline infusion at room temperature at a rate ranging between 10 and 50 mL/min, depending on the patient’s age. EMGs were performed using peri-anal surface electrodes. Cystometric capacity was categorized according to its relation to age as low, high, and normal. Normal bladder capacity was estimated in milliliters determined by Koff’s formula, 17 (age in years +2) × 30, up to the age of 12 years. Cystometric capacity was considered low if it was below 70% of the expected volume and high if it was above 150%. Bladder compliance was considered normal if it was 10 cm H2O at bladder capacity, or 5% of normal capacity per cm H2O, or approximately 20 cm H2O at expected bladder capacity.15,18,19 The bladder capacity and compliance were determined without considering reflux and urine volume escaping to the upper urinary tract.
A root square of the voided volume was used to estimate the Maximum flow rate (Qmax). Normal values for Qmax were above 11.5 mL/s in children aged ⩽6 years and above 15.0 mL/s in children aged ⩾7 years.
Residual volumes (PVR) over 30 mL or 21% of bladder capacity in children between 4 and 6 years old, over 20 mL or 15% of bladder capacity in children between 7 and 12 years old and over 50 mL, following double voiding in children older than 12 years were considered abnormally high. 20 Involuntary detrusor contractions >15 cm H2O during the filling phase were defined as DO. 19 Dysfunctional voiding was defined, when two urodynamic signs were documented: (1) Intermittent (interrupted) pattern of void in free uroflowmetry, before starting the test and (2) In the end of cystometry, the patient voided again and the second uroflowmetry revealed intermittent pattern. Also, when the Detrusor pressure increased, voiding sign disappeared and when Detrusor pressure decreased voiding started (all proving the effect of pelvic floor muscles hyperactivity (dis coordinated void)). 21
All procedures involving human participants in the study were approved by the Ethics Committee of the Urology and Nephrology Research Center of Shahid Beheshti University of Medical Sciences with the number IR.SBMU.UNRC.REC.1401.020. Written informed consent was signed by the parents or legal guardians of all children, outlining the aim, benefits, and potential adverse effects of the study.
The statistical analyses were conducted using IBM SPSS software (version 26). The mean and standard deviation were described by quantitative variables. Numbers and percentages were also used to define qualitative variables. Chi-square and Fisher’s exact tests were conducted to compare between-groups data. Statistical significance was determined by a p-value of ⩽0.05.
Results
The study included 157 children with 254 reflux units who met the inclusion criteria. There were 69 boys and 88 girls (M/F ratio; 1:1.27), with median patient age at UDS of 8 years (IQR: 5–11). Table 1 demonstrates patients’ demographic data.
Patients’ demographic data.
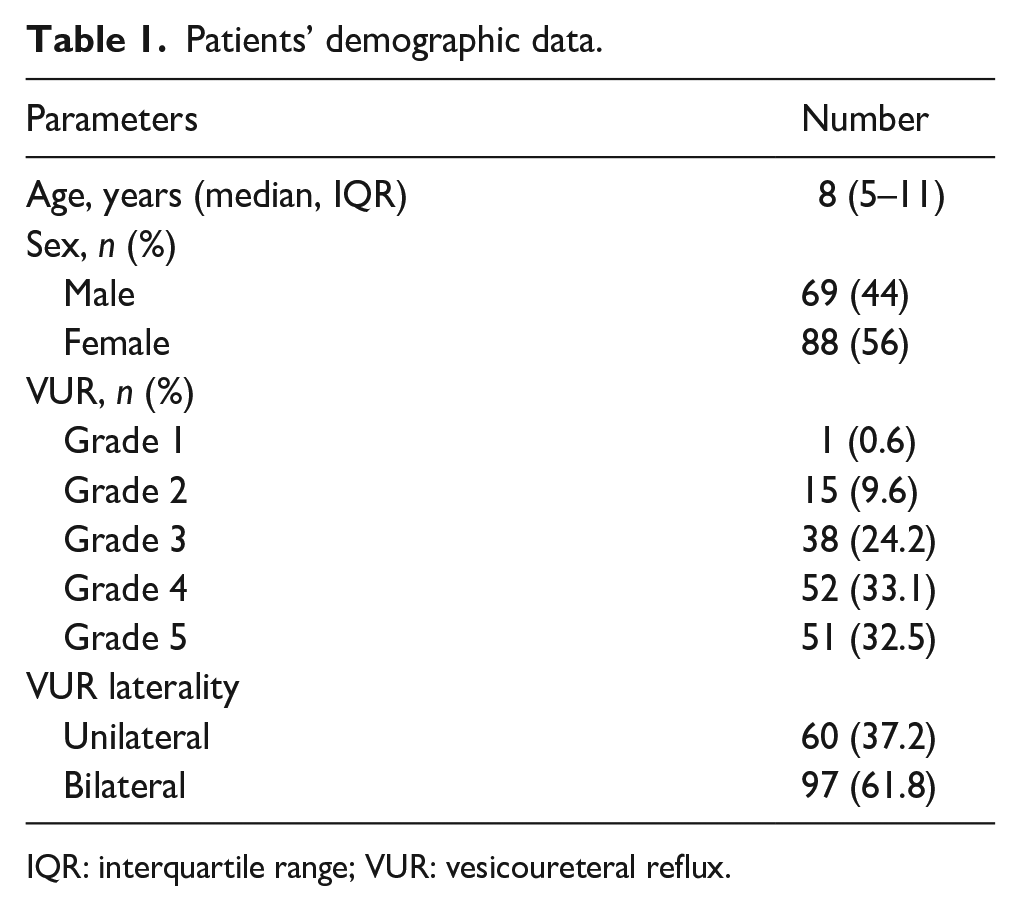
IQR: interquartile range; VUR: vesicoureteral reflux.
LUTS were present at evaluation in 75 (37.2%) participants. Irritative urinary symptoms were reported in 29 (18.4%) patients and obstructive urinary symptoms were reported in 27 (17.1%) patients. Urge incontinence was the most common single presenting symptom (19 patients, 12.1%). Children without LUTS demonstrated a higher prevalence of severe and bilateral VUR than those with LUTS (75.6% vs 54.6%, p = 0.013). On the UDS, 131 children (83.4%) had abnormal UDS findings with a male-to-female ratio of 1:1.4.
DO was found in 101 (64.3%) participants, and the prevalence was higher in children under the age of 10, with unilateral VUR and with lower grade VUR (II, III). The mean number of DOs was 5.4 ± 4.8 with a minimum of 1 and a maximum of 30. Dysfunctional voiding (DV) was found in 79 (50.4%) participants and the prevalence was higher in children older than 10, in children with bilateral VUR and higher grades VUR (VI, V). No significant relationship was observed between age sub categories and abnormal UDS findings (Tables 2 and 3).
Relation of UDS findings and severity and laterality of VUR.
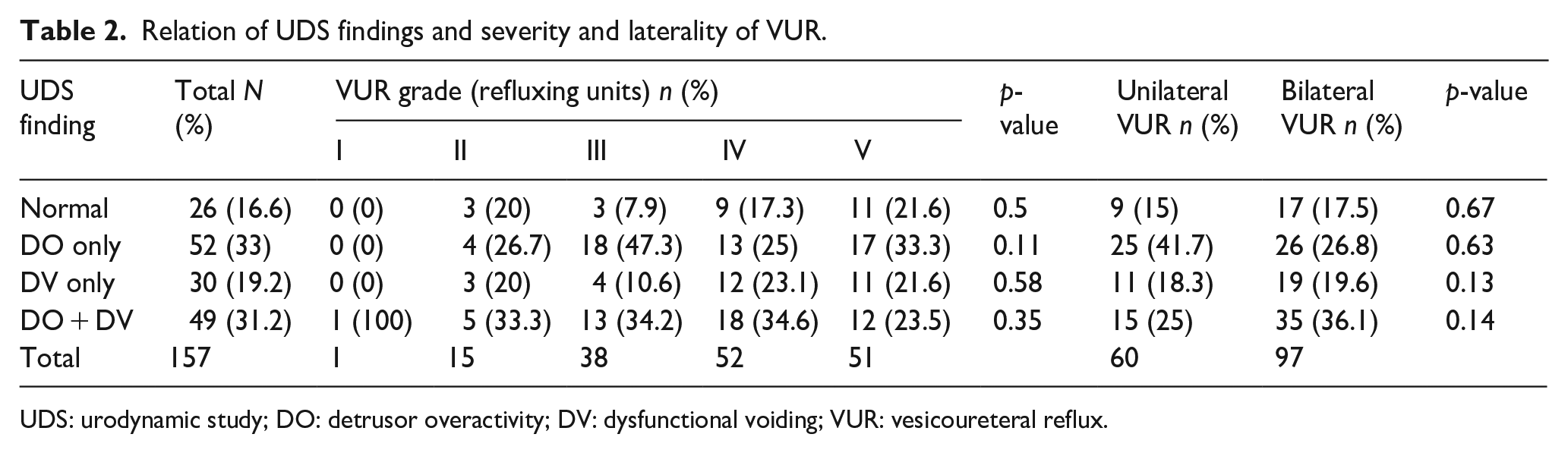
UDS: urodynamic study; DO: detrusor overactivity; DV: dysfunctional voiding; VUR: vesicoureteral reflux.
UDS findings in age subcategories.
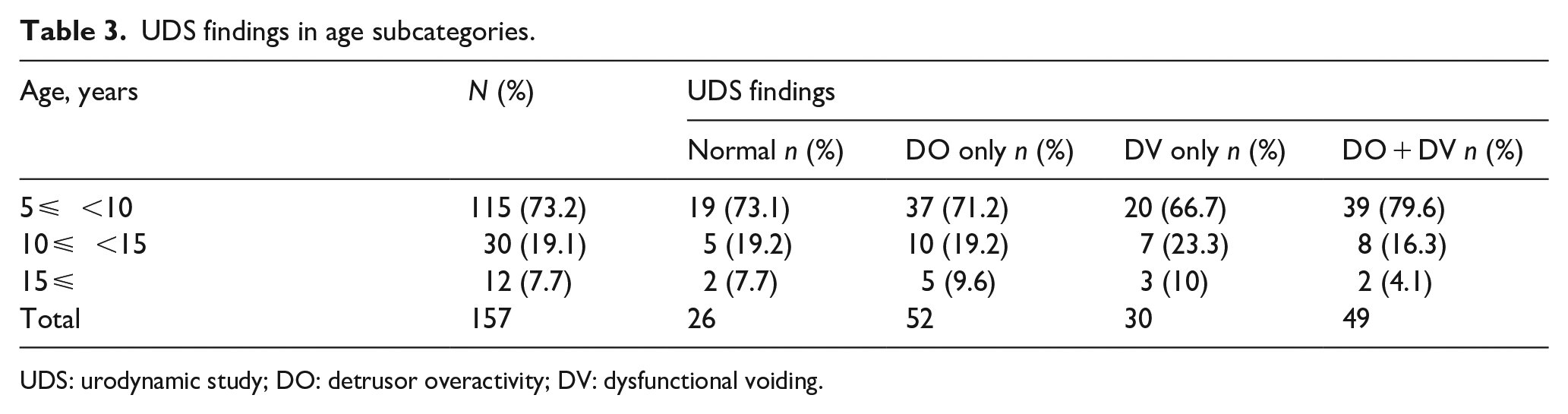
UDS: urodynamic study; DO: detrusor overactivity; DV: dysfunctional voiding.
Moreover, a comparison of UDS with patient history indicated a higher prevalence of LUTS, BBD, and UTI in children with abnormal UDS findings (Table 4).
Relation of UDS abnormality with LUTS, UTI and BBD.

UDS: urodynamic study; LUTS: lower urinary tract symptom; UTI: urinary tract infection; BBD: bladder and bowel dysfunction.
A comparison of the severity and laterality of VUR and UDS findings showed that children with lower VUR grades (II and III) and children with unilateral VUR had a higher prevalence of abnormal UDS findings than children with higher VUR grades (IV and V) and children with bilateral VUR. These differences were not statistically significant (p = 0.5 and 0.67 respectively) (Tables 2 and 5).
Relation of LUTS with VUR laterality and grade.
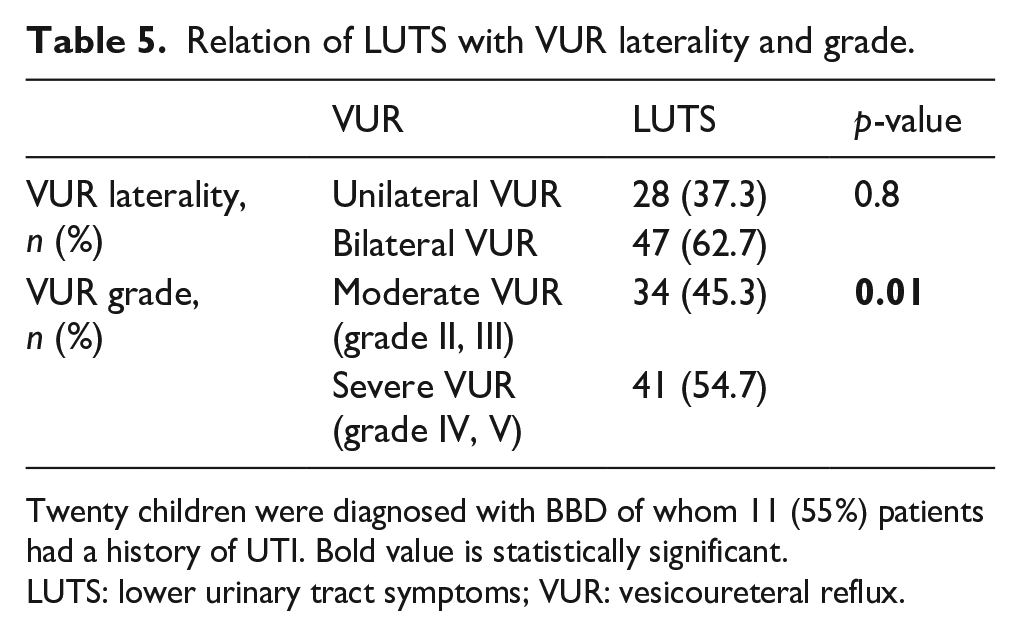
Twenty children were diagnosed with BBD of whom 11 (55%) patients had a history of UTI. Bold value is statistically significant.
LUTS: lower urinary tract symptoms; VUR: vesicoureteral reflux.
Discussion
The relationship between bladder dysfunction and VUR in otherwise healthy children is becoming increasingly evident.22,23 Although bladder dysfunction may contribute to VUR, the extent of its involvement is unclear. Based on the available data, it is difficult to estimate its true incidence in the VUR population. There has been a wide variation of incidences after toilet training age ranging from 18% to 75%.24 –26
A high rate of bladder dysfunction was observed among our patients. The prevalence of UDS abnormalities and LUTS was higher in patients with lower grades and unilateral VUR. In addition, LUTS was more prevalent in patients with abnormal UDSs. The presence of UTI was significantly correlated with the diagnosis of BBD and abnormal UDS findings.
Depending on the severity of the VUR, there was an interesting difference in the incidence of bladder dysfunction. The prevalence of UDS abnormalities was higher among children with lower grades and unilateral VUR. Accordingly, bladder dysfunction may play a role in the development of mild VUR. The vesicoureteral junction could be marginally competent in some children who are stressed by a dysfunctional bladder causing an obstruction to the outflow. 27 In contrast, the vesicoureteral junction anomaly most likely contributes to the development of more severe VUR, as evidenced by the low incidence of bladder dysfunction among this population of children. 27 Considering the absence of video urodynamics in our center, results were solely determined by the UDS. It could be speculated that bladder dysfunction would have higher rates in higher grades of VUR if a video urodynamic study was conducted and the amount of urine that escaped into the upper urinary tract could be measured.
In our population, DO was the most common type of bladder dysfunction. It was more prevalent in younger children, lower VUR grades, and unilateral VUR. Overactive bladder occurs in younger children who are transitioning from infantile to adult patterns of urination. According to this theory, the problem is caused by delayed maturation of bladder automatism control, which prevents the disappearance of uninhibited bladder contractions that normally dissipate as the bladder matures and an adult voiding pattern is acquired. 28 This bladder contraction may cause the urethral sphincter to contract, resulting in high intravesical pressure and mild VUR. However, DV is believed to be a learned behavior that develops in response to uninhibited bladder contractions and manifests after the toilet training period.14,26,29,30 In this case, outflow obstruction is more prominent, resulting in severe bladder tissue dysfunction. This is consistent with our observations that DV is more prevalent in children with bilateral VUR, higher VUR grades, and older children.
According to recent studies, VUR is present in 14% to 46% of children with idiopathic LUTD.31,32 Based on our results, 47.7% of our patients with VUR also had LUTS. Although some studies have focused on bilateral reflux as an associated factor with LUTD.32,33 In our study, the rate of LUTS was significantly higher in patients with unilateral and mild VUR.
In several studies, it has been demonstrated that children with LUTS and VUR have a higher prevalence of UTIs. 4 They also have a lower cure rate following endoscopic treatment. 34 According to our study, the prevalence of UTI was higher among participants with LUTS and abnormal UDSs. Proper management of LUTD has been shown to reduce the rate of UTI and improve the resolution of VUR.8,12,35,36
An untreated underlying LUTD is one of the primary causes of surgical failure in patients with VUR. 34 Considering the relationship between LUTS and VUR, some authors recommend evaluating all children with VUR for abnormal UDS findings.9,37
There is an increased risk of developing bowel dysfunction in patients with bladder dysfunction. 38 An American Urological Association (AUA) meta-analysis revealed that BBD significantly delayed the resolution of primary VUR. 7 The presence of BBD is an important risk factor for UTI in children, particularly toilet-trained children. 7 In our study, 13% of the participants had BBD, of which more than half had urinary tract infections.
The presence of BBD increases the risk of breakthrough UTI in children with VUR even while on prophylactic antibiotics. 39 As a consequence, there is an increased risk of renal scarring.39,40
Recent research has demonstrated that antibiotic prophylaxis is more beneficial for patients with BBD compared to those without BBD.41 –43 Therefore, it is imperative to evaluate BBD when planning management for patients with primary VUR.
The results of the present study must be interpreted in light of several limitations. An inherent limitation of the study is the retrospective collection of data that caused the pdet q max values to be missing data. Also, the limited number of participants precluded interpreting the results.
Conclusion
This study demonstrates the heterogeneity of the VUR population and suggests that bladder dysfunction may play a role in the pathogenesis of VUR, especially in mild cases. Additionally, these results indicate the need for UDS investigations to be included in the evaluation and treatment of children with VUR.
Footnotes
Acknowledgements
None.
Author’s contributions
FS: Project development, supervision, Review and editing manuscript. BN: supervision, Review and editing manuscript, Data collection and management. AM: Writing and editing original draft, Data collection and management. MA: Writing and editing original draft, Analysis and interpretation of data, Data collection and management. HR: Writing and editing original draft, Analysis and interpretation of data, Data collection and management. MD: Review and editing manuscript, Data collection and management.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written Informed consent was signed by all children’s parents or legal guardians.
Institutional review board statement
All procedures involving human participants in the study were approved by the Ethics Committee of the Urology and Nephrology Research Center of Shahid Beheshti University of Medical Sciences with the number IR.SBMU.UNRC.REC.1401.020.