
Abstract
Objectives:
Lymphatic channels (LC) are not as prominent as blood vessels, so they tend to get damaged during surgical procedures. It can present with chyle leak in the postoperative period. We aimed to study the occurrence of chyle leak in patients undergoing nephrectomy and its management.
Methods:
During the period of January 2021 and January 2023, 158 adult patients underwent nephrectomy for various reasons like non-functioning kidney, donor nephrectomy, and malignancy. We retrospectively analyzed data of patients who had chyle leak after nephrectomies.
Results:
Eight patients out of the 158 patients (5.06%) undergoing nephrectomy developed chyle leak. One out of these eight patients underwent nephrectomy by open approach while seven underwent laparoscopic approach. All eight patients who had chyle leak undergone left sided nephrectomy. Six patients of chyle leak could be managed with dietary modification while two patients needed octreotide therapy for treatment. Higher Body Mass Index (BMI; p-value = 0.012), left sides nephrectomy (p-value = 0.013), h/o pyelonephritis (p-value = 0.005) were associated with higher incidence of chyle leak on univariate analysis. While on multivariate analysis no factor was found to be independently associated with chyle leak. Hospital stay was significantly prolonged in patients with chyle leak (p-value = 0.007).
Conclusion:
Chyle leak is not a very rare complication after nephrectomy. Patients with higher BMI, who undergo left sided nephrectomies and patients who had history of pyelonephritis or infectious complications had higher incidence of chyle leak. Most cases can be managed with conservative management (CM). Chyle leak is associated with a prolonged hospital stay.
Introduction
Lymphatic vessels comprise a network of capillaries, primarily microvessels, and a large system of ducts within the body. These structures transport lymph away from tissues toward the general circulation. These channels also drain the absorbed nutrients from the gastrointestinal tract in the form of chyle and convey it via the thoracic duct into the systemic circulation. Chyle is a milky fluid containing interstitial fluid and absorbed emulsified fat. 1 As lymphatic channels (LC) are not as prominent as blood vessels, they are prone to damage during surgical procedures. 2 Significant lymphatic leakage is seldom seen following urologic procedures. The actual incidence of chyle leak (CL) is challenging to ascertain due to a limited number of high-quality studies in the literature. Urological procedures posing a risk of CL include retroperitoneal lymph node dissection (RPLND), nephrectomies for various indications, pelvic lymph node dissection (PLND), and renal transplant. 1 The incidence varies from <1% to 6% in renal surgeries according to the reported literature. 3 However, when it occurs, it contributes to increased morbidity and stress for the patients. As nephrectomy is one of the most common procedures performed at our center, we planned to study CL following nephrectomy. In this series, we discuss CL, its management, and interpretation after nephrectomy.
Materials and methods
The aim of this study was to investigate the occurrence of CL following nephrectomy in a retrospective cohort. The primary objective was to evaluate the incidence of CL and the success of management strategies at our center. The secondary objective was to identify risk factors associated with CL following nephrectomy.
CL was defined as the drainage of milky fluid from an abdominal drain or wound with lipid content (triglycerides (TG) >110 mg/dl), infection-free, and amylase-free with an output of >100 ml/day. Chylous ascites (CA) occur when there is CL but no pathway for it to exit the abdomen. Often, these terms are used interchangeably. 1 At our institute, we follow a stepwise approach, beginning with a low-fat, high-protein diet with medium-chain triglycerides (MCT) immediately after diagnosing CL. If CL does not subside within 5 days, we add octreotide, which is administered at 100 µg intravenously three times a day for 2 weeks. If these basic measures fail at 10 days, we consider fasting the patient and initiating total parenteral nutrition (TPN). If all these measures fail at 15 days, we plan imaging to locate the potential leak site using lymphangiography, lymphoscintigraphy, or magnetic resonance imaging (MRI), followed by embolization, or surgical ligation. The drain is removed after the drainage falls below 30 ml/day. A normal diet is gradually reintroduced after a period of 4–6 weeks.
We retrospectively evaluated all the patients who underwent nephrectomy for various reasons during the study period from January 2021 to January 2023. All cases were evaluated for age, sex, side, body mass index (BMI), indication for nephrectomy, infection, previous interventions such as surgery or percutaneous nephrostomy placement, surgical approach (open vs laparoscopic), and histological diagnosis. We follow standard steps for laparoscopic transperitoneal nephrectomy. For open nephrectomy, we follow standard steps of transperitoneal or retroperitoneal nephrectomy, depending on etiology, and the surgeon’s preference. We place drain in each case.
CL was quantified as mild (<300 ml/day), moderate (300–800 ml/day), and severe (>800 ml/day) as proposed by Zi Qin Ng and He. 4 CL was also classified according to the International Study Group of Pancreatic Surgery, depending on the therapy required for management. Type A CL was managed solely with dietary restrictions, Type B required TPN, somatostatin analogs, maintaining drains, or placing new ones, and Type C includes patients who needed more invasive procedures like embolization and surgery, ICU stay, or had mortality. 5
Statistical analysis
Data were entered into Excel sheets. All statistical analyses were performed using SPSS 23. The appropriate statistical test was used. In univariate analysis, logistic regression was employed to identify the factors associated with CL. Important relevant factors were used in multivariate analysis. A p-value <0.05 was considered statistically significant.
Results
A total of 158 patients were evaluated in the study, eight of whom had CL. The clinical profiles of patients who had CL are summarized in Table 1. Six patients had mild CL while two had moderate CL. We had 75% of patient of Type A CL while 25% Type 2 CL as per the international pancreatic surgery study group. All the cases were evaluated for various possible risk factors and compared with the rest of the patients undergoing nephrectomy. The patient-specific characteristics were compared and are presented in Table 2.
Details of patients with chyle leak.
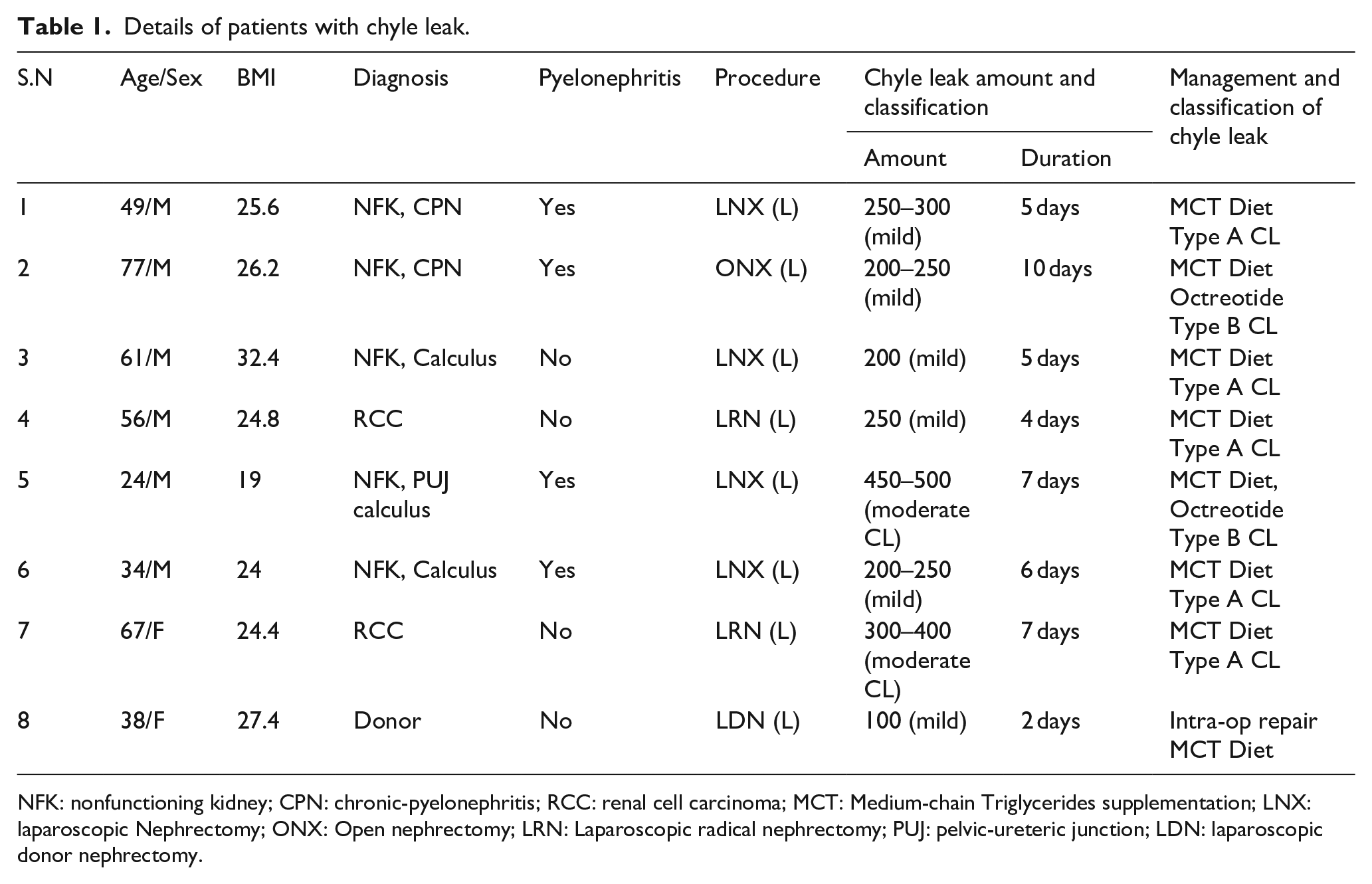
NFK: nonfunctioning kidney; CPN: chronic-pyelonephritis; RCC: renal cell carcinoma; MCT: Medium-chain Triglycerides supplementation; LNX: laparoscopic Nephrectomy; ONX: Open nephrectomy; LRN: Laparoscopic radical nephrectomy; PUJ: pelvic-ureteric junction; LDN: laparoscopic donor nephrectomy.
Comparing patient characteristics among the two groups (chyle leak vs no chyle leak).
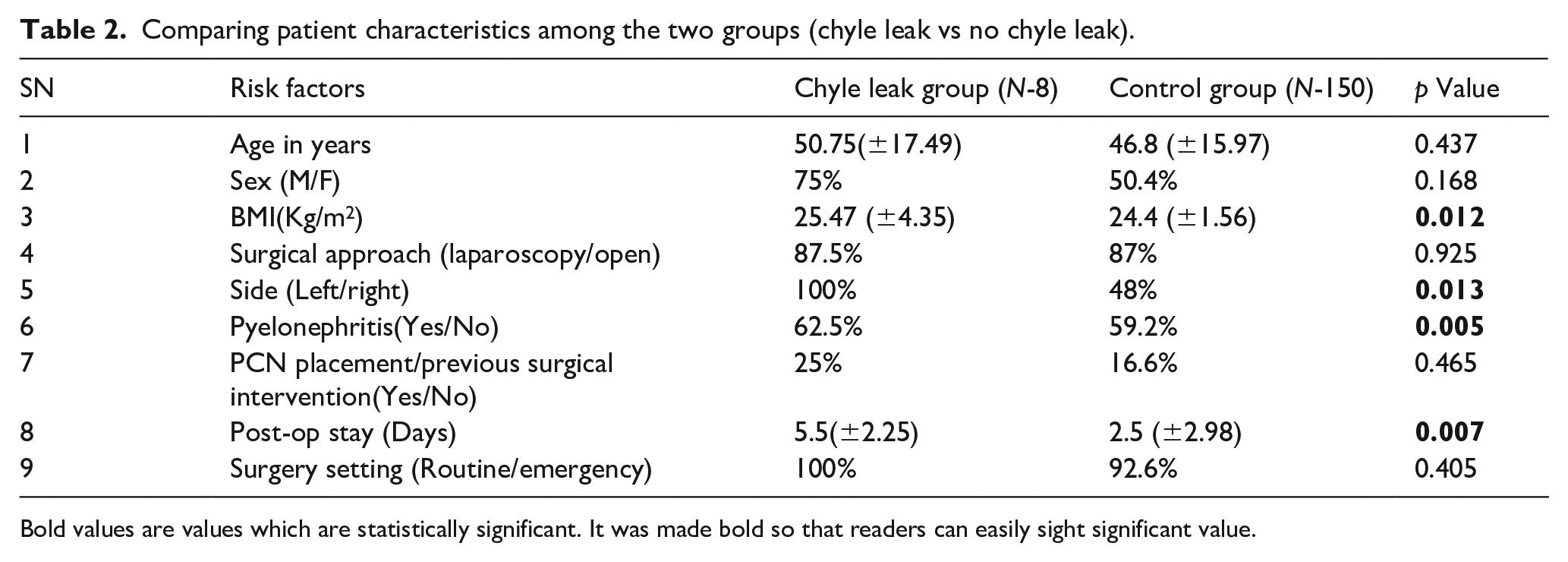
Bold values are values which are statistically significant. It was made bold so that readers can easily sight significant value.
Male patients comprised 75% of the CL group and 50.4% of those without CL (p-value = 0.168). Patients with a high BMI were more prone to CL, and it was statistically significant (p-value = 0.012). There was no statistically significant difference between the laparoscopy versus open nephrectomy group (p-value = 0.925). Left side nephrectomy was significantly correlated with CL (p-value = 0.013). Pyelonephritis was significantly associated with chyle leak (p-value = 0.005). Patients who had CL had an overall longer hospital stay (5.5 vs 2.5 days) compared with the rest of the patients (p-value = 0.007). On multivariate analysis, no factor was found to be independently associated with CL.
Details of patients are given below. They were thoroughly counseled regarding CL.
Case 1
A 49-year-old man who underwent a laparoscopic left nephrectomy for a nonfunctioning kidney (NFK) with renal stones and pyonephrosis. In the post-operative period, he had whitish discharge from the drain, ranging from 150 to 200 ml per day (Figure 1). It was biochemically confirmed to be chyle. He was managed conservatively with a low fat, high protein diet with MCT supplementation and responded within 5 days. His drain output decreased gradually to less than 30 ml per day, and it was removed on post-surgery day (PSD) 6. Histopathology revealed chronic pyelonephritis.
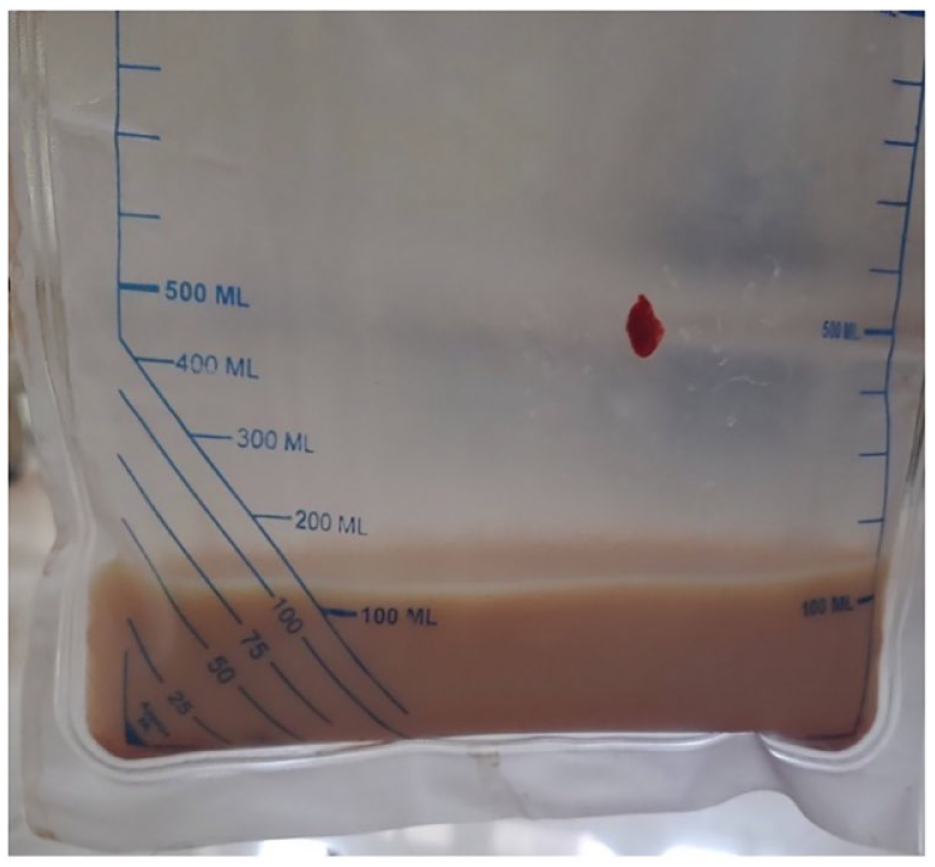
Chyle in drain.
Case 2
This patient was a 71-year-old male with a left NFK. He had a prior history of infected hydronephrosis and nephrostomy placement. He underwent an open left transperitoneal simple nephrectomy. On PSD 2, the drain was removed. He developed thick discharge from the wound site on PSD 3. The fluid was white in color. Biochemical and lab analysis confirmed it as chyle. A stoma bag was applied at the wound region where the chyle was leaking. His daily leakage ranged from 200 to 250 ml/day. He was started on a low fat, high protein diet with MCT supplementation on PSD 3. However, the CL persisted, and he was then started on octreotide injections on PSD 6. He responded well to this, and the leak decreased to a negligible amount in 1 day. He continued on octreotide for 14 days. An ultrasound scan on day 5 of octreotide initiation showed no significant collection. He was then discharged on PSD 11. Histopathology revealed xanthogranulomatous pyelonephritis (XGPN).
Case 3
The patient was a 61-year-old overweight male (BMI 32.4 kg/m2). He also underwent a laparoscopic left simple nephrectomy for an NFK due to renal stone disease and repeated infections. He had CL in the postoperative period, in the range of 200 ml per day. The patient was given a low fat, high protein diet with MCT supplementation, to which he responded well. His drain output decreased gradually and was removed on PSD 5 and patient was discharged.
Case 4
The fourth patient was a 56-year-old male with left renal cell carcinoma. He underwent a laparoscopic left radical nephrectomy. This patient also had post-operative CL in the range of 250 ml/day. He was also managed with a low fat, high protein, and MCT diet, and it gradually subsided over a period of 4 days. The drain was removed on PSD 5 and the patient was discharged.
Case 5
This patient was a 24-year-old male with a left NFK due to secondary PUJO following a history of open stone surgery 6 years ago. He underwent a laparoscopic left simple nephrectomy. In the post-operative period, he started having CL in the range of 450–500 ml/day. He was started on a low fat, high protein diet with MCT supplementation. However, his drain output did not decrease. The patient was very apprehensive and required psychiatric counseling. He was then started on octreotide injections on PSD 5, and gradually his drain output started decreasing. Drain output was nil on PSD 8. Histopathology showed chronic pyelonephritis.
Case 6
The sixth patient was a 34-year-old male with left-sided NFK due to stone disease. He underwent a laparoscopic left simple nephrectomy. In the post-operative period, he developed CL in the range of 200–250 ml per day. He was started on an MCT diet. His drain output gradually decreased, was removed on PSD 6. Histopathology showed chronic pyelonephritis.
Case 7
The patient was a 67-year-old woman with left-sided metastatic RCC. She underwent laparoscopic left cytoreductive nephrectomy. The patient had enlarged hilar lymph nodes and lymphatics. The LCs were coagulated with Ligasure. However, the patient developed CL in the post-operative period with an output of 400 ml per day. She was started on a low fat, high protein diet with MCT supplementation. After 5 days, her drain output decreased to a minimal amount. After this, her drain was removed, and she was discharged.
Case 8
A 38-year-old woman underwent a left laparoscopic donor nephrectomy. Intraoperatively, visible CL was seen in the hilar region (Figure 2). The patient had extensive adhesions near the renal hilum. After completion of the donor nephrectomy, the area of the leak was overrun with an absorbable suture. The drain output was in the range of 100 ml/day. She was started on an MCT diet. It gradually decreased, the drain was removed on PSD 3 and then discharged.
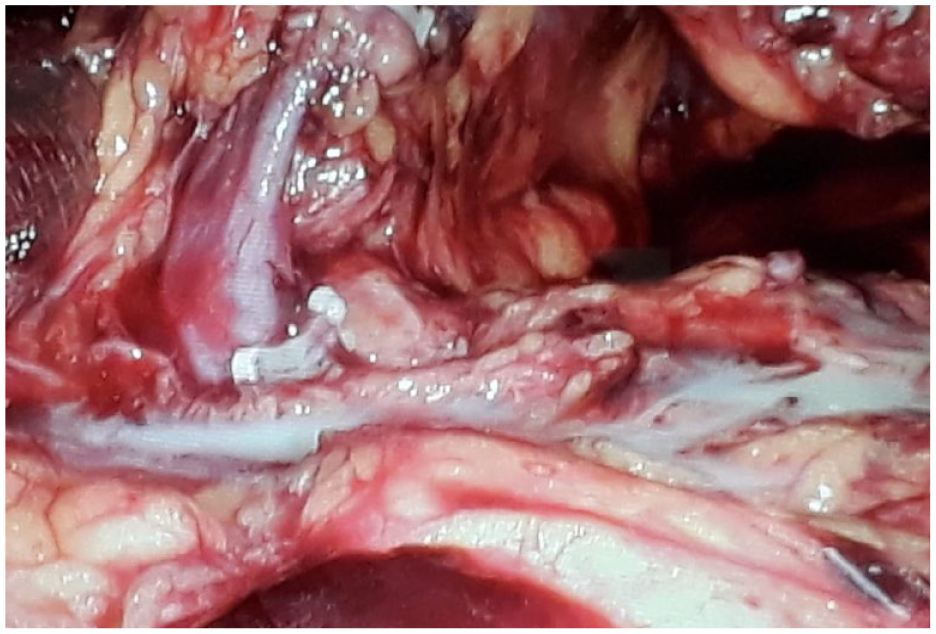
Intraoperative chyle leak during laparoscopic left donor nephrectomy.
Discussion
Preventive measures are important to avoid CL. Ligation of lymphatics with clips or sutures is of utmost importance during hilar and retroperitoneal dissection. 6 The use of the Ligasure device for coagulation of lymphatics was significantly associated with CL after liver transplant. 7 Meticulous dissection is needed in the paraaortic region to prevent damage to the cisterna chyli. We could detect CL during one case of left LDN, where a suture ligation of the CL site was performed.
The amount of CL depends on the severity and site of the injury. Injury to the cisterna chyli or thoracic duct will result in a high output CL. 8 Management also depends on the amount of CL and its response to conservative management (CM). In our study, 75% of patients with CL can be managed with diet modification only.
Drain placement after nephrectomy is important as it provides information about potential hemorrhage and allows for the detection of CL. CL often becomes evident once patients start oral intake in the postoperative period. Many centers routinely advocate for drain placement, while others do not.3,9 This discrepancy may be the reason for having more cases of chylous ascites (CA) in follow-up. Once a normal diet is resumed, fats and lipid content are absorbed in the intestine. Short-chain fatty acids are taken into circulation by the portal venous system, while long-chain fatty acids are absorbed by lymphatic capillaries in the intestine and form chylomicrons. 10 This process also carries lymph, which is rich in lymphocytes and serves immune functions. This understanding forms the basis of CL management by recommending a medium-chain triglyceride (MCT) and low fat diet to minimize leakage and allow time for healing.
Somatostatin analogs like octreotide and lanreotide, which are used for the management of CL, act on vascular somatostatin receptors and decrease lymphatic excretion. This action leads to decreased traffic of lymphatic fluid through the channels and provides time for healing. Total parenteral nutrition (TPN) provides complete bowel rest and aids healing at the leakage site. The combination of an MCT diet, somatostatin analog and TPN comprises the conservative management (CM) of CL. 11 As reported in the literature, most patients with CL at any site in the body respond to this management.
We reviewed English literature regarding CL and CA after nephrectomies, focusing on studies from 2010 to the present (Table 3). There are few case series and multiple case reports. The majority of these indicate that CL was successfully managed with CM.12,13 Those who did not respond to these measures underwent various interventions, including radiological procedures, minimally invasive procedures, or major surgeries.3,6,14 The exact timing for considering these invasive procedures varied across different reports from 6 days to 8 weeks.2,3,15 Delay can be associated with complications like a cachexic condition due to nutritional loss, infections due to poor immunity, and anxiety and depression caused by uncertainty regarding treatment measures.
Articles on chyle leak and chylous ascites.
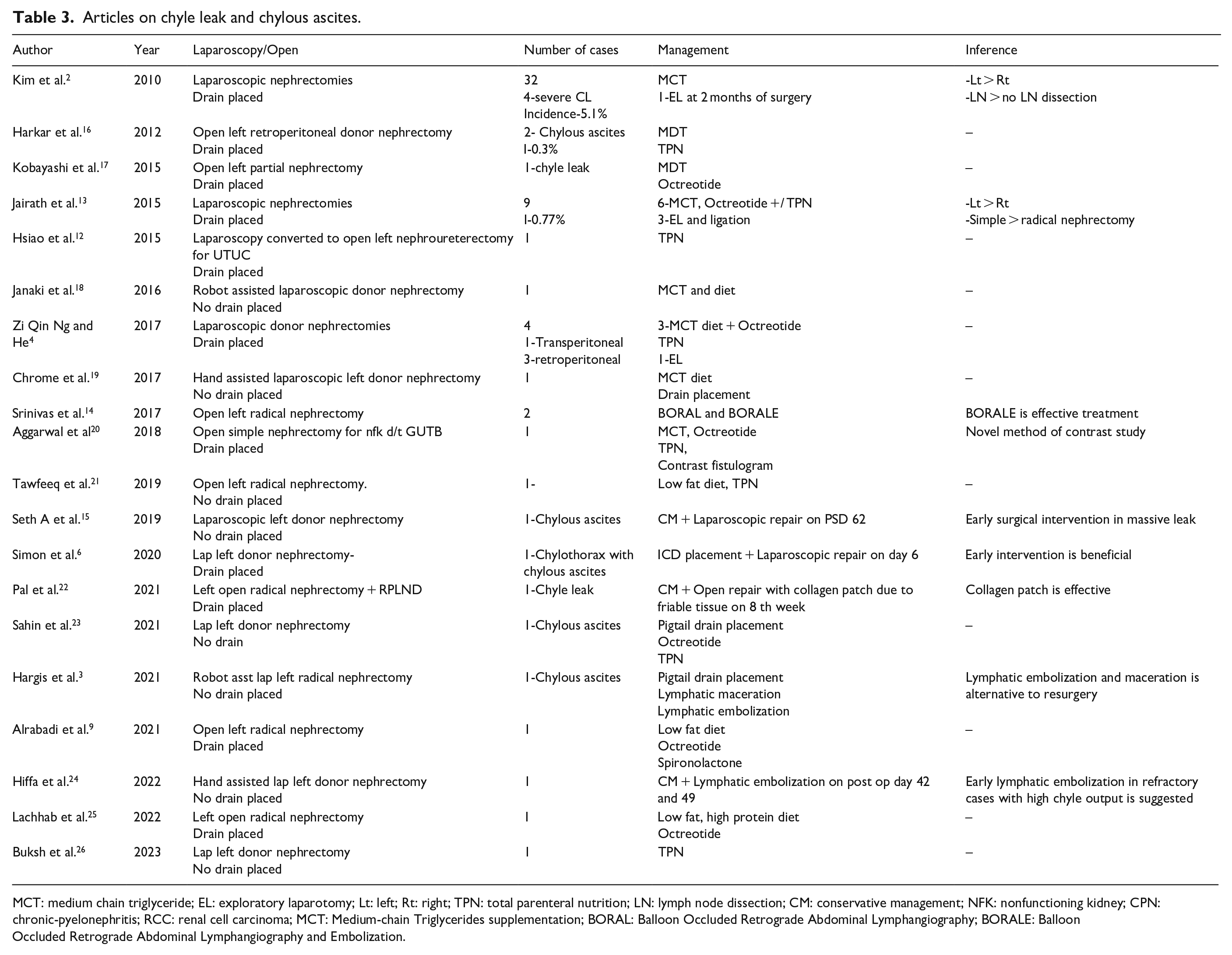
MCT: medium chain triglyceride; EL: exploratory laparotomy; Lt: left; Rt: right; TPN: total parenteral nutrition; LN: lymph node dissection; CM: conservative management; NFK: nonfunctioning kidney; CPN: chronic-pyelonephritis; RCC: renal cell carcinoma; MCT: Medium-chain Triglycerides supplementation; BORAL: Balloon Occluded Retrograde Abdominal Lymphangiography; BORALE: Balloon Occluded Retrograde Abdominal Lymphangiography and Embolization.
Jairath et al. 13 in their case series, encountered nine cases of CL after laparoscopic nephrectomies for various indications. Three of these nine patients required surgical intervention with ligation at the lymphatic leak site. Two of these cases presented as CA in follow-up, while one had CL from the port site.
Kim et al. 2 reported an incidence of CA in 5.1% (32/622) of cases in their study. One case required surgical exploration and ligation due to refractory CL. CM was implemented for up to 2 months in this patient. They recommended clipping and ligation of lymphatics during nephrectomy to prevent CL. Left-side nephrectomy and procedures involving lymph node dissection were significantly associated with leakage.
Zi Qin Ng and He. 4 reported four cases of CL in their series. One patient who underwent left LDN required surgical intervention. The patient underwent laparoscopic exploration and ligation of the suspected site with 4-O prolene on post-surgery day (PSD) 36, but the leak persisted. Lymphoscintigraphy could not detect the leak site. An open exploratory laparotomy was performed on PSD 79, and the leak site was repaired in two layers. The patient was discharged on PSD 104. This case exemplifies how CL can be morbid.
Hippa et al. 24 in their case report of chyle leakage (CL) after laparoscopic hand-assisted left donor nephrectomy, noted a persistent leak. The patient underwent lymphoscintigraphy and embolization on post-surgery day (PSD) 42 at an interventional radiology lymphatic center. However, the leak still persisted, and the patient again underwent MR lymphangiography to detect the site of the leak and underwent embolization again on PSD 49. This report emphasizes the importance of having access to expert resources and centers that can employ interventions like embolization in the management of CL, thus avoiding surgery.
Hargis et al. 3 in their case report, described a patient who underwent robot-assisted laparoscopic left radical nephrectomy. At 7 weeks, the patient presented with abdominal distension and was found to have chylous ascites (CA). A drain was placed, and treatment was initiated. In view of the persistent high drain output, the patient was planned for intervention after 1 week of treatment. Lymphangiography detected the site of the leak, and the lymphatics below this leak were macerated using a needle to block them. The leak persisted, and the patient required lymphatic embolization after 1 week with lipiodol and N-butyl cyanoacrylate. Afterward, the leak was resolved. This report emphasizes the importance of early management using a less invasive approach once a high output leak is detected.
Simon et al. 6 reported a rare case of chylothorax after left LDN, which was managed with intercostal drain placement and early laparoscopic ligation of the leak site on PSD7.
Pal et al. 22 described a case of CL that occurred after a left radical nephrectomy and extended retroperitoneal lymph node dissection (RPLND) done for a renal mass. Due to the high output of CL, the patient underwent lymphangiography, and lipiodol injection, but the leak persisted. The patient was then planned for open surgical repair. Multiple leak sites were noted, and attempts to close them with sutures failed due to friable tissue. A collagen patch was used to seal the leak, and it proved successful. This report provides an alternative intraoperative management option when tissue is friable. Also it suggests stepwise management of invasive procedures for CL.
Srinivas et al. 14 employed Balloon Occluded Retrograde Abdominal Lymphangiography (BORAL) and Balloon Occluded Retrograde Abdominal Lymphangiography and Embolization (BORALE) for the successful treatment of three patients with CA. Two of them had undergone a nephrectomy for cancer.
In the reviewed literature, reinterventions to stop chyle leakage were carried out from 6 days to 2 months post-surgery. This suggests variability in the timing of treatment escalation.
CL often leads to prolonged hospital stays, as many studies have noted.16,22,24 In our study, although no patient required invasive treatment, hospital stays were still significantly longer for patients with CL.
Various methods of invasive management are available and have been tried in the past for patients with CL who are not responding to conservative management (CM). The method that is feasible, accessible, and where expertise is available should be utilized for treatment to avoid delay and failure. We have developed a algorithm based on our experience and reviewed literature for CL (Figure 3).
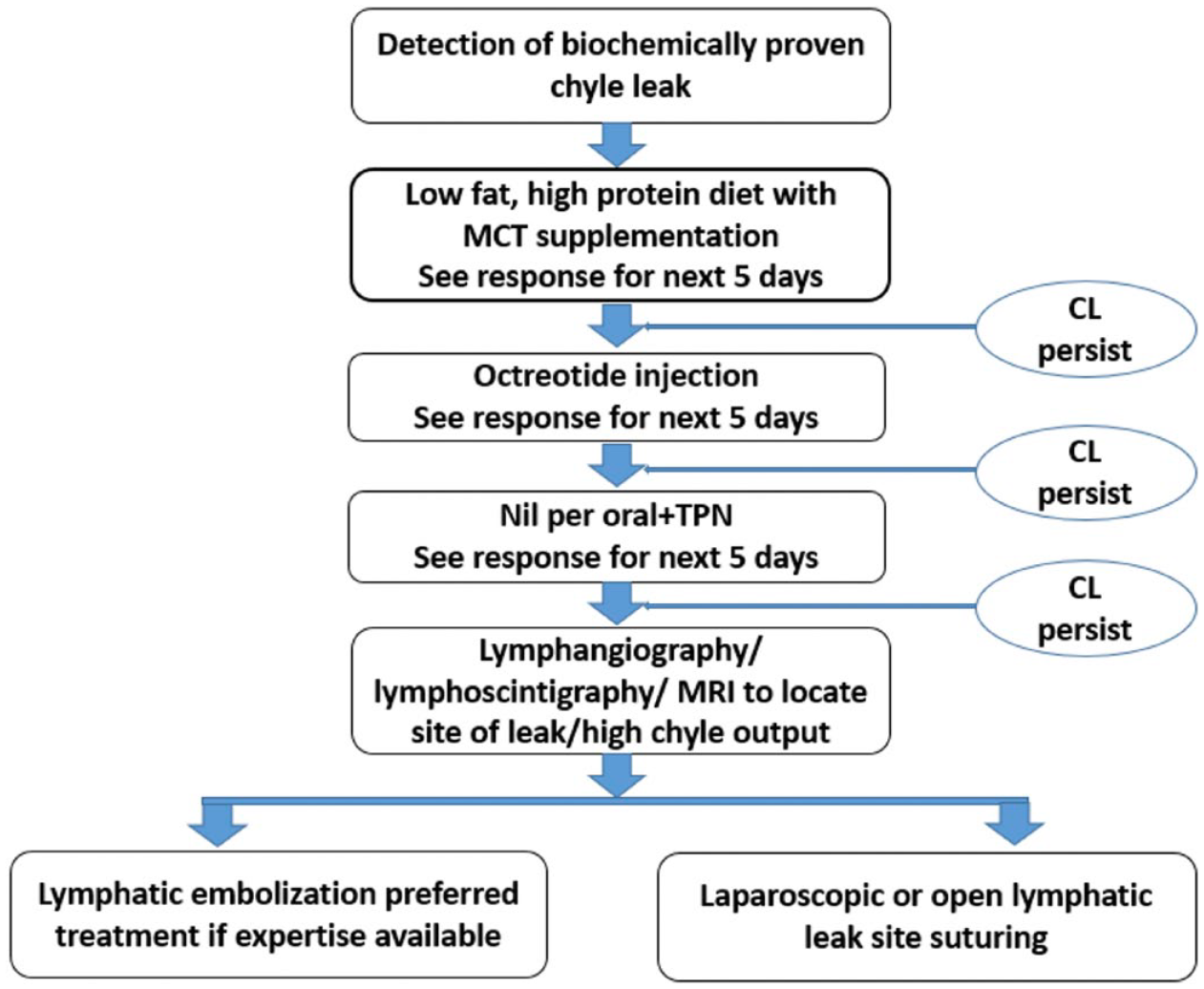
Algorithm for management of chyle leak.
Rose et al. 11 developed an evidence-based treatment algorithm for the management of CA after surgery. In their review, they noted that prolonged treatment with CM increased patient morbidity and length of stay. They suggested that a trial of conservative management (CM) be given for 21 days, and escalation of management should occur if it fails at 21 days or if the drain output exceeds 750 ml per day. Lymphangiography and/or embolization is preferred first rather than going directly for surgery, depending on the availability of facilities. The same trend is noted in recent literature.
The limitations of this study are firstly, it being retrospective. Secondly, the study has a small number of patients. More high-quality studies, designed in a prospective manner, are needed to form an evidence-based protocol for the management of this rare complication.
Conclusion
Chyle leak after nephrectomy is seen more frequently after left-sided nephrectomies, in obese patients, and in patients with pyelonephritis. It is associated with prolonged hospital admission. Conservative measures form the backbone of management. A low threshold should be kept for invasive management if conservative measures fail.
Footnotes
Author’s contribution
All authors have read and approved the manuscript. The following authors have contributed as outlined below: Concept – SS, DB; Design – SS, AS, GRC; Data acquisition – SS, AA; Data analysis – SS, DB; Manuscript preparation – SS, DB, MS; Critical analysis and editing – SS, SN, GRC. Post-operative Chyle Leak Following Nephrectomy: Inference from tertiary care center and Review of Literature.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical clearance
Institute Ethics Committee.
Consent
Obtained.