
Abstract
Objective:
The purpose of study was to report the subjective and objective results of different methods of surgical treatment of cystocele using the transvaginal Mesh-system.
Methodology:
A prospective study was conducted from January 2017 to December 2020 comparing anterior colporrhaphy with vaginal mesh and two distinct types of vaginal wall repair sutures in the surgical treatment of cystocele. The primary endpoint was the incidence rate of vaginal wall erosion complications 12 months after surgery. Secondary endpoints were anatomic outcomes, TVM-related morbidity, and patient satisfaction measured using validated questionnaires.
Results:
In total, 102 patients with stage III-IV cystocele and the average age of 67.2 ± 3.1 years (age range of 47–79 years old) took part in the study. Of the 102 women initially enrolled, 102 (100%) were successfully followed up 12 months after primary surgery. The primary result, the objective erosion development, was radically different in the comparison groups (1.6% against 23.5%, respectively). Analysis of the improved method of operative treatment showed a prominent level of positive, uncomplicated, surgery results of 98.4% (60/61). The anatomic success rate of recovery from cystocele was 99.9% (101/102) 12 months after surgery.
Conclusion:
The suggested method of restoring the anterior vaginal wall in stage III-IV isolated cystocele without signs of incomplete and complete prolapse of the uterus showed a radically positive result. The number of complications was relatively high in the comparison group, but no difference was observed in satisfaction with the anatomical results of the surgery. The percentage of the vaginal wall erosion when using a single-layer suture is 23.5%, when using a two-layer suture is 1.6%
Introduction
Recent studies strongly suggest that the risk of pelvic organ prolapse is 13%–19% throughout life,1,2 and most often patients are operated on for cystocele. 3 The elevated risk of relapse after this procedure is from 30% to 61.7%2,3 and 7% when using prosthetic materials,2–5 which requires the search for new relapse-free technologies and a reduction in the complications number, new treatment methods. As a result, the use transvaginal Mesh-systems (TVM), which are non-resorbable or partially resorbable, has become a forced necessity for the creation of neofascia and nen-unions of the pelvic organs. The use of these implants reduced the frequency of anatomical relapses, but at the same time it caused the development of complications that are characteristic only when using TVM. 6 A number of these complications prompted the Food and Drug Administration (FDA) and the Scientific Committee on Emerging and Newly Identified Health Risks (SCENIHR) to issue restrictions on the use of TVM. 7 Short-term results of TVM show better anatomic and subjective results compared to native plastics, while increasing the risk of re-intervention due to specific complications. 8 Over the last decade, TVMs have decreased in weight to lightweight and ultra-lightweight implants, which correspond to the trends in hernia surgery. 9 A significant reduction in the number of complications during their use was noted. A decrease in the inflammatory reaction of the surrounding tissues to the synthetic material and the number of side effects was established. 10 The number of specific complications during the performance of a certain surgery type using TVM in vaginal surgery and their impact on the quality of women’s life, has not been thoroughly studied until now.11–19
In 2016, the scientific community reported 21 cases of repeated interventions due to the development of complications after TVM surgery in the anterior area (Prolift, Perigee and Avaulta). Indications for re-intervention were erosions, pain, including dyspareunia, apareunia, relapse of prolapse. Unsuccessful attempts at conservative treatment using oestrogen cream, antibacterial therapy, and physical therapy are reported in 63% of cases, and in all cases subsequent excision of the implant was required. Out of 81 patients, 30 (37%) underwent complete excision of the TVM, 49 (61%) underwent partial excision, and in 2 cases (2%) a small area of the mesh was excised. The study indicated the use of various implants: Gynemesh, Mersilene, Prolift, Ultrapro, TVT™, TVT-O™ (Ethicon, Somerville, NJ, USA), IVS™ (Tyco Healthcare LP, Norwalk, CT, USA), Avaulta™ (CR Bard, Covington, GA, USA), Apogee™ (American Medical Systems, Minnetonka, MN, USA), Endo Fast Reliant (Endogun Medical Systems, Kibbutz Haogen, Israel), Gore-Tex, Mycromesh (WL Gore, Flagstaff, AZ, USA), Teflon (Davol/Bard, Cranston, RI, USA).
The Prolift™ system accounted for 40% of all prostheses that were excised. The excision was carried out in 89% of cases by vaginal approach, in 5% of cases by laparoscopic approach in combination with vaginal one and in 1% of cases by laparoscopic approach only. As a result of repeated operations, complications are reported as follows: intestinal injury (one case of sigmoid colon injury and two cases of damage to the serous membrane of the small and large intestines), anuria (one patient) due to damage to both ureters that was not noticed intraoperatively (bilateral ureterocystoneostomy was carried out), two cases of haematomas, one case of bleeding, one case of intestinal obstruction, three cases of urinary tract infection; two cases of fever; one case of wound infection; one subcutaneous abscess and kidney hydronephrosis. 20 There are a limited number of studies that have compared different options for post-operative wound closure using light TVMs and no information on the long-term outcomes of these studies, but the results of such studies are necessary. The purpose of this study was to report the subjective and objective results of different methods of surgical treatment of cystocele using the transvaginal Mesh-system.
Materials and methods
A prospective study included 102 patients surgically operated for cystocele without signs of complete or incomplete uterine prolapse from January 2017 to December 2020, comparing anterior colporrhaphy with vaginal mesh use (Parietene™, MacroporousMesh, Covidien, France) and two different types of sutures for the restoration of the vaginal wall in the surgical treatment of cystocele. Surgical interventions were performed involving surgeons who had experience in the use of polypropylene TVM mesh upon transvaginal access in the treatment of genital prolapse. At the time of inclusion in the study, all patients had signs of stage III–IV cystocele. Preoperative assessment consisted of an interview, urogynecological examination and quantification of prolapse using the simplified pelvic organ prolapse quantification (POP-Q) (measurement of total vaginal length at rest and Ba, C/D, and Bp points at maximum, when performing the Valsalva manoeuvre). 21 The patients underwent a routine examination before surgical intervention.
Inclusion criteria: signs of cystocele with an isolated assessment of Ba ⩾ +1 (stage III or IV), without contraindications for the TVM use. The implant had a lambdoid shape of the author’s design, made of polypropylene macroporous lightweight mesh, containing a base with a semicircular cut and elongated edges in its lower part. 10 The surgery was performed under regional anaesthesia or general anaesthesia. The patient was placed in the lithotomy position. The bladder was not catheterised. The surgical field was treated with an antiseptic solution of 10% Povidone-Iodine. Hydropreparation was carried out with 0.9% NaCl solution up to 100 mL with the addition of 0.18%–0.25 mL adrenaline hydrochloride. The anterior vaginal wall was incised with a scalpel in the sagittal direction. The incision depth was up to the opening of the urogenital fascia. After placement of the implant, the vaginal wall was repaired with sutures (Polyglycolide 1-0) using two techniques. In the main group, the proposed method of restoring the anterior vaginal wall included a separate, two-layer, closure of the urogenital fascia with a continuous S-shaped suture, followed by closure of the vaginal wall with a simple single-row encircling suture. In the patients of the comparison group, a continuous single-row suture was used to close the postoperative wound. Secondary endpoints were anatomic results, morbidity connected with TVM, pelvic organ function and patient satisfaction measured using validated questionnaires. In the postoperative period, all patients of the study groups received local therapy in the form of a single daily irrigation of a ready-made officinal form of 5 mL of a solution of hexamidine diisethionate 0.1 g, chlorhexidine digluconate 0.1 g, chlorocresol 0.3 g per 100 mL and vaginal suppositories containing dexpanthenol 0.1 g and chlorhexidine bigluconate 0.016 g, within 30 days from the first day after surgery.
Anatomical results after surgery were assessed according to the POP-Q system for the anterior segment (T, Ba, Cd, Bp). The result was evaluated as anatomically successful at Ba -1; 0 or less. The pelvic organ’s function was assessed according to the MHU (urinary handicap measurement), PFDI-20 (Pelvic Floor Distress Inventory) and PFIQ-7 (Pelvic Floor Impact Questionnaire) questionnaires, 22 which included the assessment of stress urinary incontinence (SUI) symptoms, overactive bladder (OAB). Satisfaction was evaluated according to a four-point scale (++, +, +/−, −). Furthermore, 12 months after the surgery, a vaginal examination was performed to establish signs of a decubitus of the anterior wall of the vagina, in the form of erosion with a visible fragment of the TVM, or a fragment of the TVM determined by palpation. Quantitative changes described by frequency in the sample were statistically evaluated. Qualitative changes were estimated as mean and standard deviations. The non-parametric Wilcoxon test was used to compare the POP-Q values and pelvic organ function indicators. 23
In this study, the authors used a lightweight mesh (46 g/m2) (Parietene™, Macroporous Mesh, Covidien, France), which consists of polypropylene threads, without coating. This study is a long-term prospective observation that compared two methods of surgical wound closure in the treatment of anterior vaginal wall prolapse using TVM method that was previously reported. 10 The primary endpoint was to compare the long-term 12 month surgery result aimed at reducing the number of specific complications. Secondary endpoints were anatomic results, morbidity connected with TVM use and patient satisfaction measured using validated questionnaires.
Results
In the period from 2017 to 2020, 102 patients were enrolled. All of them agreed to take part in the study and completed the study after 12 months. The average age of patients – 67.2 ± 3.1 years (age range 47–79 years old), the average BMI – 29.9 ± 2.3 kg/m2, the average parity – 2.2 ± 1.4. Preoperative anatomical results are presented in Table 1.
Results of measuring the vaginal profile of cystocele patients before and after surgical treatment (N ± n, cm), (DI).
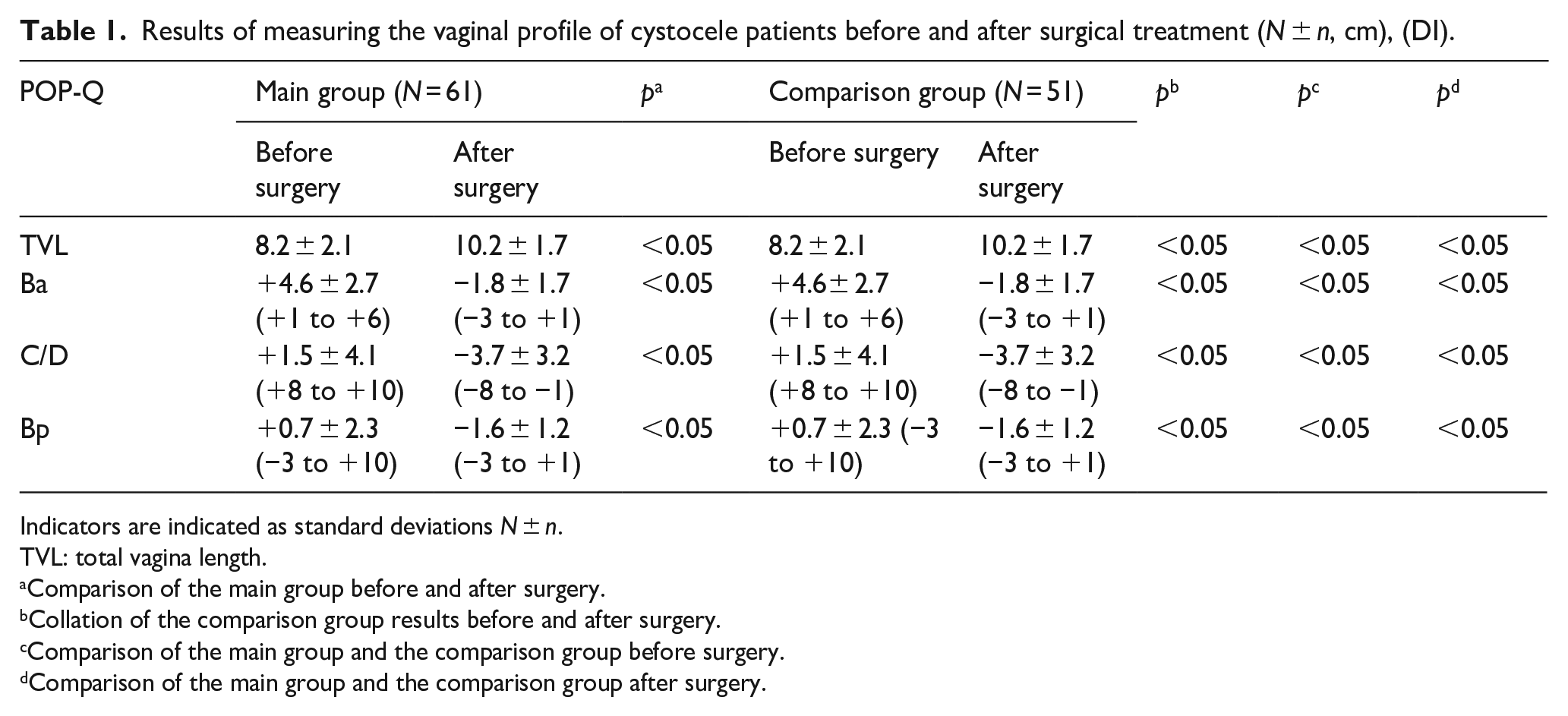
Indicators are indicated as standard deviations N ± n.
TVL: total vagina length.
Comparison of the main group before and after surgery.
Collation of the comparison group results before and after surgery.
Comparison of the main group and the comparison group before surgery.
Comparison of the main group and the comparison group after surgery.
Surgical interventions were performed under regional anaesthesia in 90/102 (88.2%), under general anaesthesia in 12/102 (11.8%), the average surgery time was 33.0 ± 14.0 min range (20–70 min). In addition, prerectal plication was performed in 102/102 patients (100%), perineorrhaphy in 100/102 patients – (98.0%). In 101/102 (99.1%) cases, antibiotics were prescribed for prophylactic purposes (Cefazolin 2.0 g intravenous injection) immediately before the start of the surgical intervention. Intraoperative complications were recorded: bladder injury in 1/102 (0.9%) patients, bleeding from the incision area of paravesical spaces in 2/102 (2.0%) patients, in all cases of these complications the TVM placement was not refused.
An indwelling urinary catheter was installed immediately after surgery and left in place in 101/102 cases (99.1%). The average catheterisation duration is 1.0 ± 0.1 days. In 13/102 (12.7%) women, urinary retention was observed for more than 1 day that required additional catheterisation for 2.1 ± 1.1 days in the range of (1–10) days. The average duration of pain in the postoperative period was 10.2 ± 2.4 (5–14) days according to the analogue scale of VAS 4.2 ± 2 of 10 (2–10) due to pain in the perineum. The average length of stay in the hospital was 1.9 ± 1.1 days, the range was (1–7) days, the main reason for the delay in discharge from the hospital was the need for the bladder catheterisation in case of atony or hypotonia. Postoperative discomfort in the perineum region was assessed after 12 months and was defined as satisfactory (+, +/−) or very satisfactory (++) in 100/102 (98.0%) patients, unsatisfactory (−) in 2/102 (2.0%) patients. Assessment of the discomfort level after 12 months showed a statistically significant difference compared to the initial assessment before surgical intervention (р > 0.05).
The assessment results according to the POP-Q system after surgery 12 months after are shown in Table 1. The anatomic success rate of cystocele recovery was 99.9% (101/102) 12 months after surgery. The results of the assessment using the POP-Q system were statistically significantly different after 12 months of observation, from the initial assessment of anatomical parameters compared to the measurements made before the operation (р > 0.05). Functional disorders of the pelvic organs that are connected with genital prolapse and MHU, PFDI, PFIQ indicators were assessed before and after surgical intervention. The results of the pathological symptoms assessment are presented in Table 2.
Results of pelvic organ function assessment in patients with cystocele before surgery and 12 months after surgery (N ± n) PFDI-20 (74.4–52 (p < 0.05)), PFIQ-7 (42–8.6 (p < 0.05)).
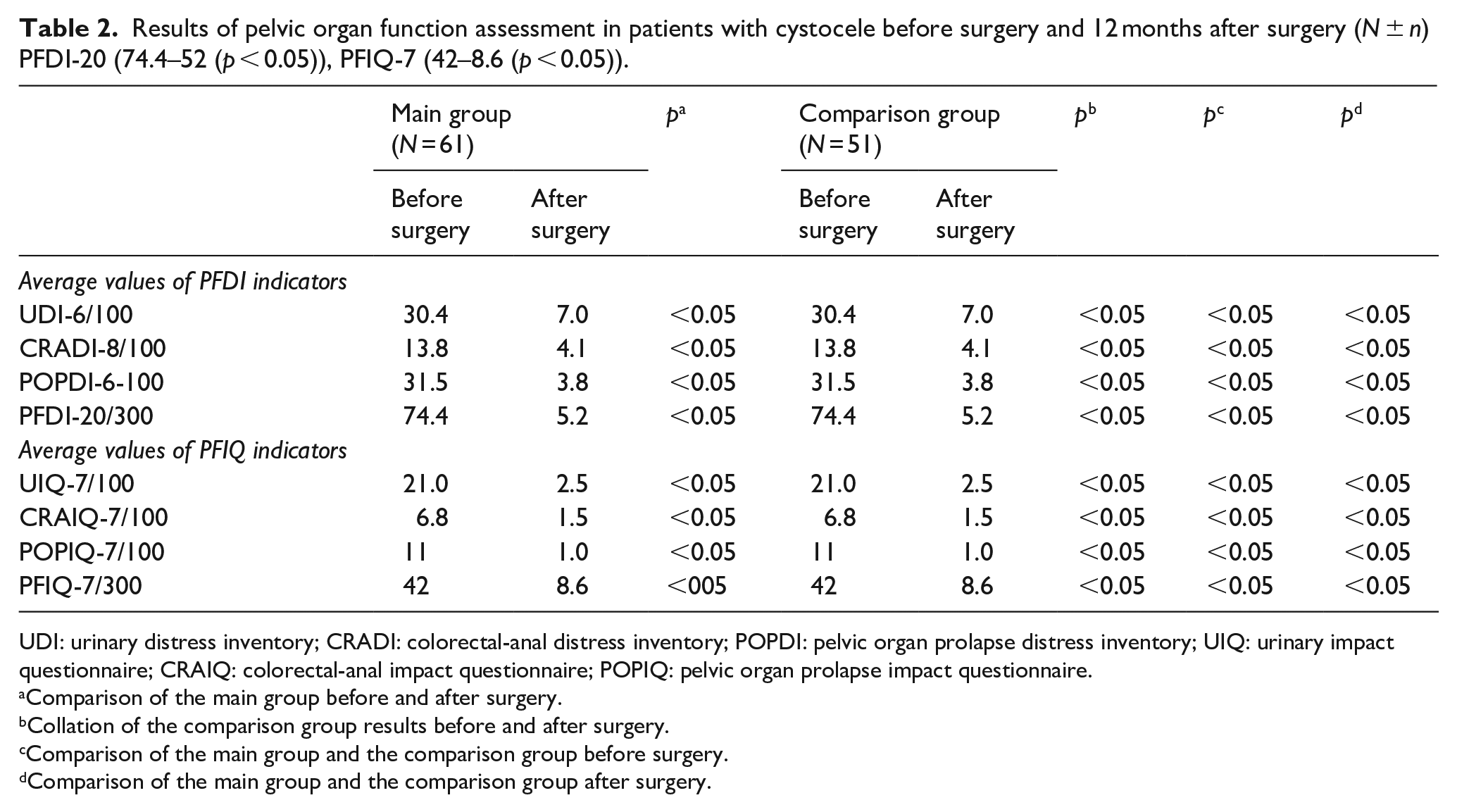
UDI: urinary distress inventory; CRADI: colorectal-anal distress inventory; POPDI: pelvic organ prolapse distress inventory; UIQ: urinary impact questionnaire; CRAIQ: colorectal-anal impact questionnaire; POPIQ: pelvic organ prolapse impact questionnaire.
Comparison of the main group before and after surgery.
Collation of the comparison group results before and after surgery.
Comparison of the main group and the comparison group before surgery.
Comparison of the main group and the comparison group after surgery.
The analysis of results after the surgical intervention 12 months after indicated a decrease in the number of cases of urination disorders and the defecation. The function of the pelvic organs function was assessed using standardised questionnaires. Most patients in the study groups showed a significant improvement in the quality of urination after surgical intervention, which was assessed after 12 months. 100/102 (98.0%) patients expressed satisfaction with the results of the surgical intervention after 12 months of observation following the surgical intervention.
The suggested methods did not significantly affect the number of cases of stress urinary incontinence (Table 3). No statistically significant difference was found in the comparison groups before and after surgery. A statistically significant (p < 0.05) decrease was observed in the number of patients who noted signs of urinary retention and chronic pelvic pain. No statistically significant decrease was observed in the number of patients with symptoms of urge incontinence before and after surgery, respectively, and in the comparison groups (p > 0.05). At the repeated follow-up at 12 months, 1/61 (1.6%) patients of the main group and 1/51 (2.0%) patients of the comparison group reported persistent pain or spontaneous pain, with a mean score of 2.3/10 cases according to VAS scale.
Results of surgical intervention in patients with cystocele using TVM (N ± n, cm).
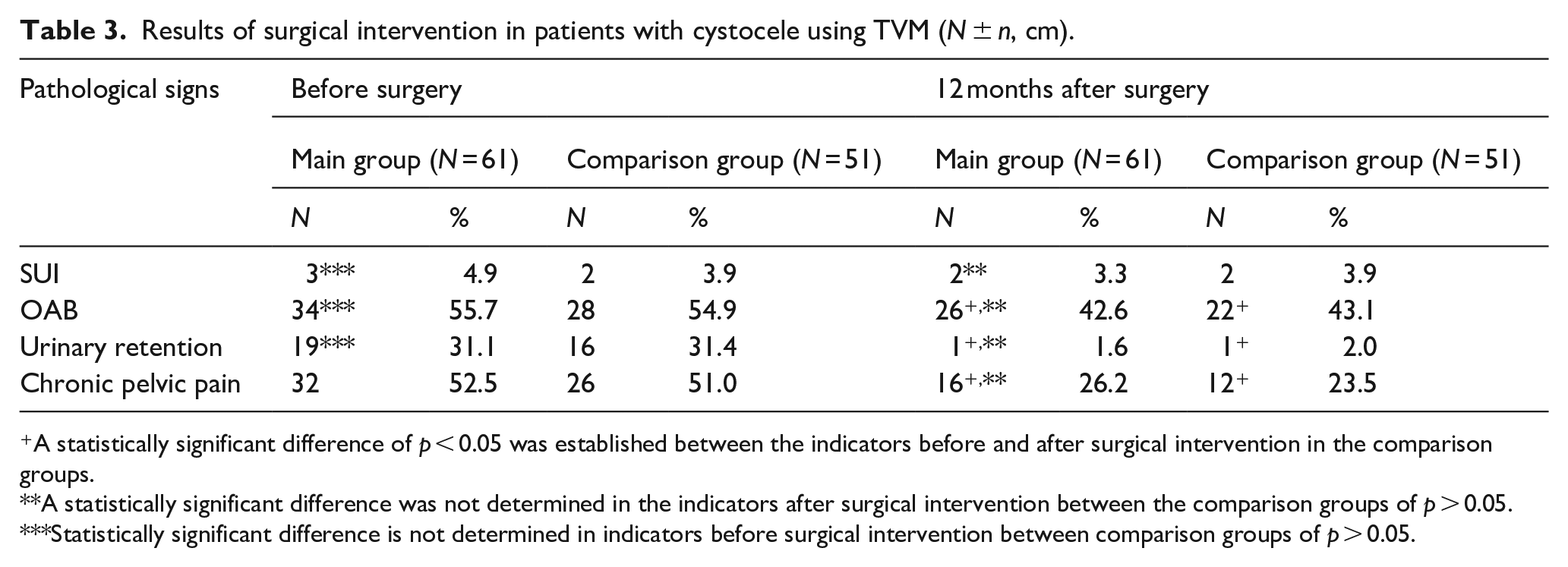
A statistically significant difference of p < 0.05 was established between the indicators before and after surgical intervention in the comparison groups.
A statistically significant difference was not determined in the indicators after surgical intervention between the comparison groups of p > 0.05.
Statistically significant difference is not determined in indicators before surgical intervention between comparison groups of p > 0.05.
The results of evaluating the effect of different methods of restoring the vaginal wall upon using TVM are presented in Table 4. The method of TVM closure suggested by the authors in the surgical treatment of cystocele showed that the signs of a TVM decubitus ulcer in the area of the anterior vaginal wall were identified in 12/51 (23.5%) patients of the control group. In contrast, only one (1.6%) case of decubitus ulcer formation on the anterior vaginal wall was recorded in the main group. During the case analysis, it was established that the cause of the decubitus ulcer formation was the TVM twisting and the possible existing extragenital pathology of the patient in the form of chronic obstructive bronchitis in connection with bronchial asthma and type II diabetes. In other patients of the main group, who were diagnosed with type II diabetes mellitus, decubitus ulcer formation in the TVM area was not established.
The result of the effect assessment of different methods of the vaginal wall repair in the surgical treatment of cystocele in female patients using TVM (N ± n, cm).
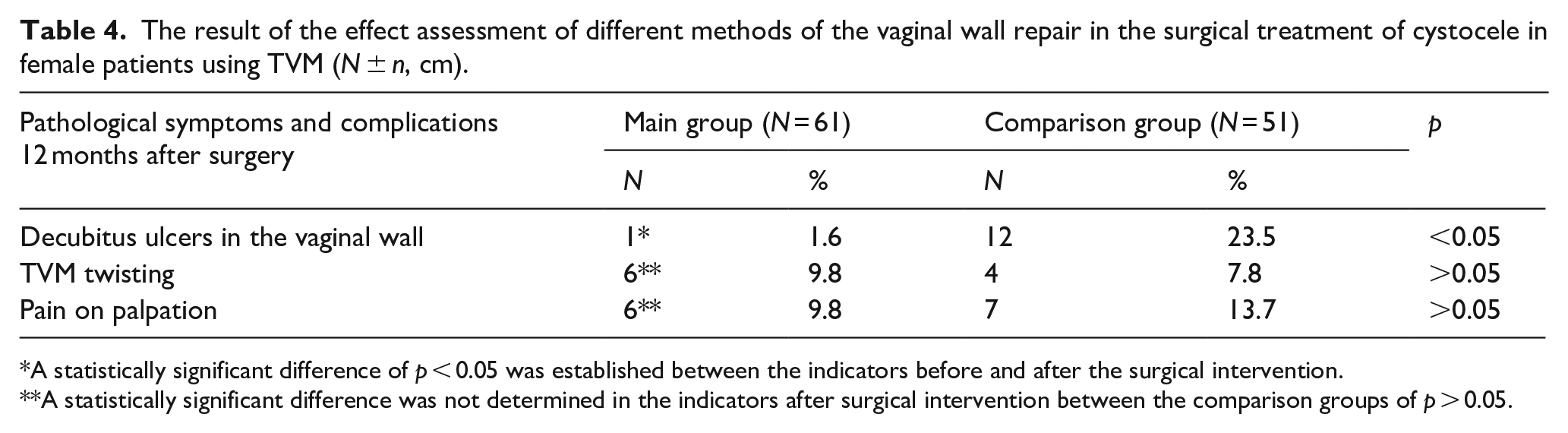
A statistically significant difference of p < 0.05 was established between the indicators before and after the surgical intervention.
A statistically significant difference was not determined in the indicators after surgical intervention between the comparison groups of p > 0.05.
In the main group of 12 patients, in whom the obesity symptoms were established in combination with the abovementioned extragenital pathology, only 1/12 (8.3%) of cases of decubitus ulcer formation were observed. The obtained result suggests that the proposed method, closing the anterior vaginal wall, when using TVM in patients with cystocele against the background of extragenital pathology, reduces the risk of complications by seven times, and can be recommended as a method of preventing complications of surgical treatment of cystocele. The analysis of cases of decubitus ulcer formation of the anterior vaginal wall in the comparison group did not establish a connection with a certain extragenital pathology. In these patients, signs of connective tissue dysplasia were found in 10/12 (83.3%) of cases, type II diabetes in 2/12 (16.7%) of cases, chronic obstructive bronchitis in 2/12 (16.7%) of cases, symptoms of chronic constipation in 5/12 (41.7%) of cases, obesity BMI > 29.9 kg/m2 in 7/12 (58.3%) of cases. The combination of extragenital pathology and obesity was established in 7/12 (58.3%) of cases.
Induced pain during physical examination at 12 months was reported by 2/61 (3.3%) patients in the main group and 3/51 (5.9%) in the comparison group with a mean VAS score of 3.3/10. The need for dissection of the mesh in the region of the lateral vaults of the vagina required by 1/61 (1.6%) patients of the main group and 1/51 (2.0%) patients from the comparison group, which helped completely eliminate pain in the area of placement of the TVM without its complete excision. In total, 1/61 (1.6%) patients in the main group and 12/51 (23.5%) patients in the comparison group underwent re-surgery for erosion of the vaginal wall in the volume of the incised visible fragment of the TVM with repeated closure of the vaginal wall with a single-layer continuous Polyglycolide 2-0 suture.
Discussion
The conducted study and analysis of its results convincingly showed that the use of a two-layer suture in the anterior vaginal wall recovery in patients with stage III-IV cystocele using TVM made it possible to reduce by seven times the number of specific complications observed in the case of the use of braided polypropylene implants. However, the suggested method did not affect the number of relapses during surgical treatment of cystocele. It should also be emphasised that the treatment impact received by patients after surgery on the number of specific complications cannot be directly assessed based on this study data. A literature review of 33 studies in the Cochrane database, which were connected with surgical treatment of cystocele, showed a different orientation of these studies with a mean and low level of evidence, which makes it difficult to compare with this study. All studies published in the last 20 years report various forms of objective assessment of operative intervention results for genital prolapse and the use of diverse types of TVM, some of which are currently withdrawn from production and are not used due to the 2011 FDA recommendations. Only nine studies completely describe the results of surgical treatment of cystocele using different TVM types.11–19
A review of 16 studies in the Cochrane database showed a high percentage of specific complications in the form of erosion of the vaginal wall. However, these studies did not report a vaginal wall recovery method that could show any significant difference in terms of risk of re-surgery or unsatisfactory functional and anatomical aspects, especially because the use of TVM itself is connected with the risk of specific complications (shrinking, exposure, pain, dyspareunia). It was established that the risk of developing erosion according to meta-analysis is 11.3% (101/896). According to this study, erosion of the vaginal wall was observed in 12.7% (13/102) of cases, which does not differ from the results provided in literature reviews on this topic. However, the method suggested by the authors made it possible to reduce the percentage of this complication from 23.5% (12/51) in the observation group to 1.6% (1/61) in the main group. It should also be noted that the age category of patients affected the possibility of developing such complication as erosion of the vaginal wall, these data are contradictory and require further study. 20
In the described study, 102 cases from 102 treated patients were fully analysed. The study results showed that a positive anatomical result of cystocele recovery was achieved in 99.9% (101/102) 12 months after the surgery. The assessment was carried out according to the POP-Q scale. The total vaginal length increased from 8.2 ± 2.1 to 10.2 ± 1.7 cm after the surgery, the Ba point changed from +4.6 ± 2.7 to −1.8 ± 1.7, the Bp point changed from +0.7 ± 2.3 to −1.6 ± 1.2 cm 12 months after treatment. Similar positive results from the anatomical structures reconstruction in the case of pelvic organ prolapse using polypropylene mesh were presented in the study of Delroy et al., 12 the anatomical success rate was 82.5% 1 year after surgery. The Ba point changed from +2.8 to −1.9 cm after the surgery, the Bp indicator was 3.0 cm before the surgery and 3.5 cm after it. The total vaginal length did not statistically change after the use of polypropylene mesh. Also, according to study by Stanford et al., 21 the success of the use of lightweight polypropylene mesh for the treatment of cystocele is also confirmed by positive changes in each point of the POP-Q scale. The anatomical success rate was 97.4% 24 months after the surgery.
In the study of de Tayrac et al., 22 the degree of anatomical success in the treatment of the anterior vaginal wall prolapse with mesh was 89% compared to classic anterior colpography. In the mentioned study using the transvaginal Mesh-system, only 2% (2/102) patients rated the surgery result as unsatisfactory. An improvement in the quality of life due to a reduction in the number of complaints specific to genital prolapse was established. The severity index of urinary retention decreased from 31.1% in the main group and 31.4% in the comparison group before surgery to 1.6% and 2.0%, respectively, after surgery. The degree of chronic pelvic pain decreased from 52.5% in the main group and 51.0% in the comparison group to 26.2% in the main group and 23.5% in the comparison group after surgical intervention. The rate of stress urinary incontinence and bladder overactivity did not statistically change before and after surgical treatment of cystocele. Thus, the severity of complaints connected with pelvic organ prolapse in the main group was statistically less after the surgery, where the author’s method of repair with a two-layer continuous suture was used. In the study of Maher et al., 23 the rate of stress urinary incontinence (low evidence level) and bladder damage (medium evidence level) were higher relative to reconstruction with native tissue. In this study, with the use of TVM quality of life indicators were assessed before surgery and at the final stage of the study, using questionnaires PFDI-20 (76.4–4.3 (p < 0.05)), PFIQ-7 (41–8.4 (p < 0.05)), confirming obtained objective results of treatment. Similar data were obtained by a number of other studies, positive subjective changes regarding the symptoms connected with pelvic organ prolapse in patients after surgical treatment with the use of a lightweight prolene mesh were found through a survey.12,13,16
In this study, when using TVM, in the studied groups, no signs of cystocele relapse were recorded. The anatomical and functional results of this study and the number of specific complications is consistent with the latest literature data.20–24 Maher et al. 23 also indicated a low risk of relapse after the use of prolene meshes relative to native tissue in the treatment of vaginal prolapse. Stanford et al. 21 indicated a specific complication rate in 11% 24 months after mesh treatment, mesh extrusion occurring in less than 1% of patients. When using the Gynemesh and Gynemesh-Soft meshes, the frequency of closing the vaginal mucus membrane was 48%, in connection with which a re-surgery was performed, 7% of women underwent complete removal of the mesh. 20 In addition, this study with the use of TVM and the use of two different types of sutures for the anterior vaginal wall repair showed that, in general, 13/102 patients (12.7%) received surgical interventions due to complications, including 1/61 (1.6%) patients of the main group and 12/51 (23.5%) from the comparison group. No complications were observed after re-surgery. Relapses were not found in re-operated patients. The obtained results make it possible to state that the development of specific complications does not increase the number of relapses in the operated area.
Therefore, the present study made it possible to evaluate the effectiveness of the use of a light polypropylene vaginal mesh (Parietene™, MacroporousMesh, Covidien, France) in the treatment of stage III-IV cystocele without signs of complete and incomplete uterine prolapse using two types of sutures for the restoration of the vaginal wall, the long-term results of the impact of the author’s method of restoring the anterior wall of the vagina were evaluated by comparing two groups of patients with the use of different types of sutures. A positive anatomical result was observed in both studied groups. The rate of the vaginal wall erosion was significantly lower in the main comparison group. Subjective genital symptoms, quality of life of patients also improved after the use of TVM in the main group and in the comparison group. The long-term success of cystocele treatment was expressed in the decrease in the number of re-surgeries, pathological symptoms and postoperative complications, more positive changes were observed in the main group.
Conclusions
The results of this study are the successful application of the author’s method of restoring the vaginal wall using a double-row suture in the treatment of pelvic organ prolapse, the degree of long-term complications and the morbidity of patients associated with the use of a transvaginal mesh were established. The anatomical success rate of restoring the anterior vaginal wall was 99.9% 1 year after surgery in the main and comparison groups. The satisfaction percentage with the pelvic organs function in women was 98.0% in both study groups of patients. The suggested method of the restoring the anterior vaginal wall with a two-layer suture for an isolated stage III-IV cystocele without signs of incomplete and complete uterine prolapse made it possible to reduce the number of specific complications in seven times in the form of vaginal wall erosion from 23.5% to 1.6%. The total percentage of specific complications when using a lightweight mesh is 12.8% (13/102) of the vaginal wall erosion. The suggested method can be recommended for use by surgeons who use transvaginal Mesh-systems for surgical treatment of cystocele. The treatment efficiency with this method depends on the severity level of cystocele, the accompanying pathology of the patient and the professional skills of the surgeon.
The author’s technology of transvaginal treatment method of cystocele using lightweight prolene mesh still requires improvement and further study. The high degree of anatomical success of the use of transvaginal lightweight mesh in the treatment of prolapse and the high probability of developing complications specific only to this complications system stimulate further study into this direction of TVM use. The comparison of the mentioned study results with the conclusions of others is complicated due to the variability of currently existing studies, which do not provide sufficient information about the use of the method for resoring the anterior vaginal wall, and the short period of patients’ observation. Long-term studies with a larger sample of patients are required for assessing the possible complications of the use of lightweight mesh in the treatment of cystocele using the two-layer suture method.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.