
Abstract
Introduction:
PCNL (percutaneous nephrolithotripsy) is considered the gold standard treatment for renal stone more than 2 cm. In today’s scenario, supine PCNL is considered equally effective as prone PCNL. The ideal position for supine PCNL is still debatable. We hereby describe our initial experiences of supine PCNL in a novel position.
Methods and materials:
This prospective study includes 60 patients who underwent supine PCNL in the ‘Calcutta position’ in our institute from August 2021 to August 2022. Successful procedure was defined as a complete stone free rate or a clinically insignificant residual stone (<4 mm).
Results:
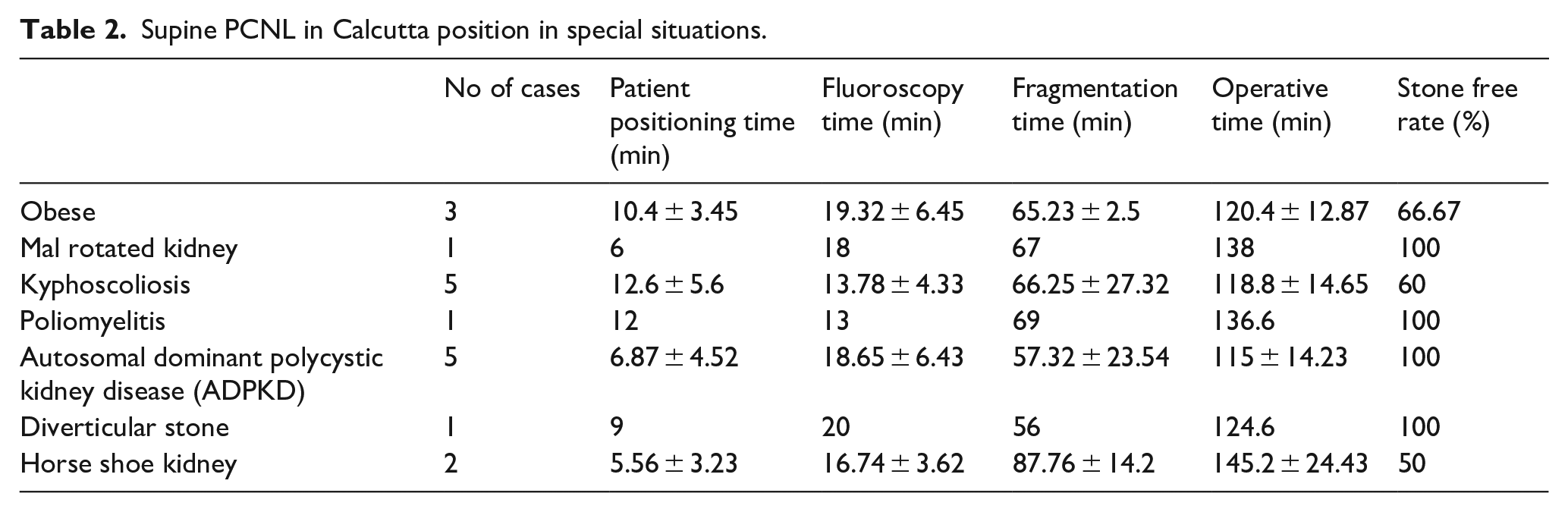
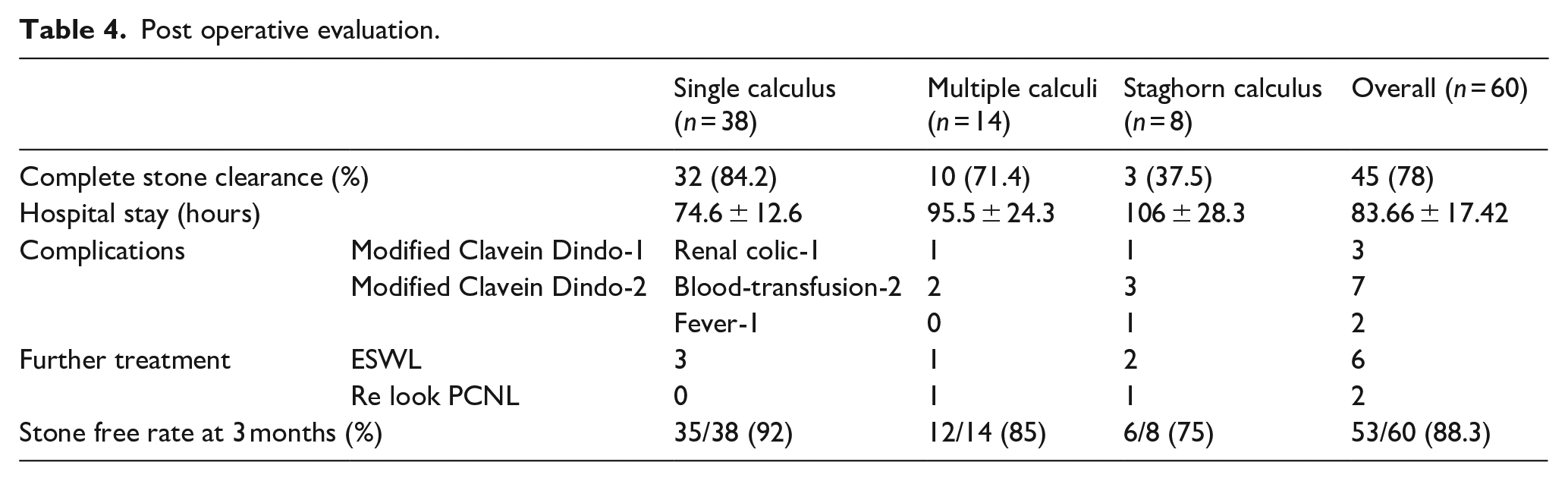
Average Operative room (OR) occupancy time was 130.9 ± 19.63 min. The immediate stone free rate was 84.2%, 71.4% and 37.5% for single, multiple and staghorn calculus respectively. Complications include fever, requirement of blood transfusions and renal colic. The average hospital stay was 83.6 ± 17.42 h. Eight patients (13.3%) required secondary procedures like extracorporeal shock wave lithotripsy (ESWL) or relook PCNL. At 3 months average stone free rates were 92%, 85%, 75% for single, multiple and staghorn calculus respectively. We performed supine PCNL in Calcutta position in obese, kyphoscoliosis, poliomyelitis, autosomal polycystic kidney disease (ADPKD), malrotated kidney and diverticular stone with comparable success.
Conclusion:
Supine PCNL in Calcutta position is a safe and effective option for nephrolithiasis management. Apart from the inherent advantages of supine PCNL it also has the advantages of better C-Arm and nephroscope manoeuvrability. Supine PCNL in Calcutta position was performed in a variety of scenarios with comparable results.
Introduction
Nephroloithiasis is quite prevalent in India, with an expectancy of 12% in total population to be prone to renal stone. 1 The surgical treatment options available are open pyelolithotomy and nephrolithotomy or minimally invasive techniques like percutaneous nephrolithotomy (PCNL), laparoscopic and robotic pyelolithotomy. Among the minimally invasive procedures PCNL has statistically significant shorter operative time, lower mean drop of haemoglobin as well as stone free rate. 2 Prone PCNL was first described by Fernström and Johansson 3 in 1976. Since then it has been considered to be the gold standard treatment for large kidney stones of size ⩾2 cm. 4 The advancement of newer imaging modalities has revolutionised this treatment option with decreased invasiveness, morbidity, and improved ergonomics and outcome.
In 1987 Valdivia first performed supine PCNL. Supine PCNL has some inherent advantages for which it has been adapted by several centres. However, its popularity is still less among the urologists. The lack of adequate training in supine PCNL from education centres and trepidation of colonic injury may be responsible for it. Valdivia-Uria 5 reported that, PCNL when performed with the patient in the supine position offers a wide variety of advantages.
Few recent meta-analyses concluded that PCNL in supine position is as effective as prone PCNL in terms of stone free rates, complication rates, requirement of transfusions and operative time.6,7 Several positions for supine PCNL have been described in literature like Galdako modified Valdivia position, Giusti position, Barts flank free approach, complete supine position and many more with inherent pros and cons of each position but there is no consensus to date about the ideal position for supine PCNL.
In our study, we describe our initial experiences of performing supine PCNL in ‘Calcutta position’ a modified decubitus in various case scenarios and their outcome upto 3 months of follow up.
Methods and materials
The study was performed from August 2021 to August 2022. Ethical clearance from the institutional ethical committee was obtained and all protocols as per the Declaration of Helsinki were followed. During this period 60 patients underwent supine PCNL in Calcutta position. Informed written consent was obtained from all patients who were included in the study. The patients were evaluated preoperatively with detailed history, clinical examination, and laboratory investigations like complete blood count, renal function test, coagulation profile and ASA (American society of anaesthesiologist) grading. For renal stones, all patients were imaged with contrast-enhanced computed tomography (CECT) scan with CT urography to assess the renal anatomy as well as extra renal structures about 1–3 weeks before surgery. All supine PCNLs were operated on under general anaesthesia.
All patients had sterile urine culture reports within the last 1 week. In case of any positive urine culture, appropriate antibiotic treatment was given and the procedure was undertaken only after the urine culture was sterile. Preoperatively all patients received intravenous third generation cephalosporins.
Technique
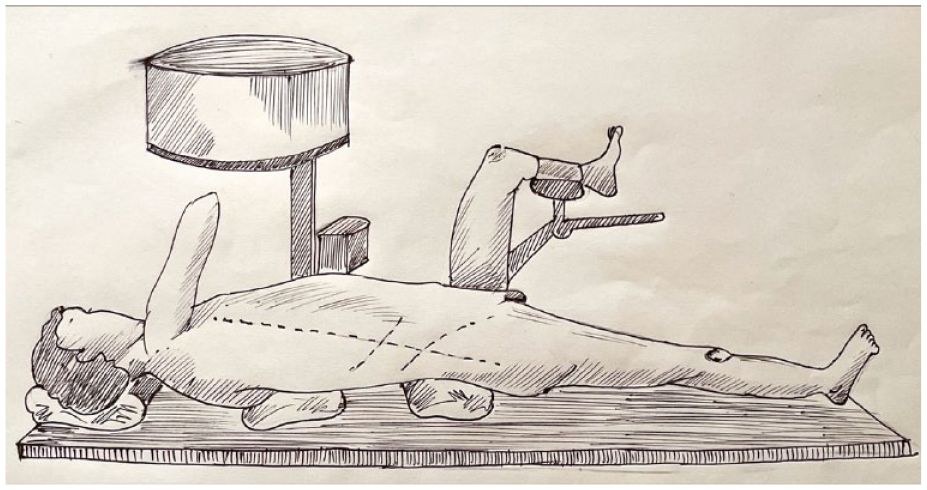
Our study describes a modified position for supine PCNL which have been termed as ‘Calcutta position’. The anesthesised patient was placed in complete supine position at the lateral edge of the operating table and the ipsilateral leg of the PCNL side was set straight on the operating table on the detachable leg plate as shown in Figures 1–4. The contralateral leg was flexed and abducted at the hip joint and supported on a single stirrup keeping an adequate place for a second surgeon to perform transurethral cystoscopy and placement of a ureteral catheter for retrograde pyelography for PCNL and if required endoscopic combined intra renal surgery (ECIRS).
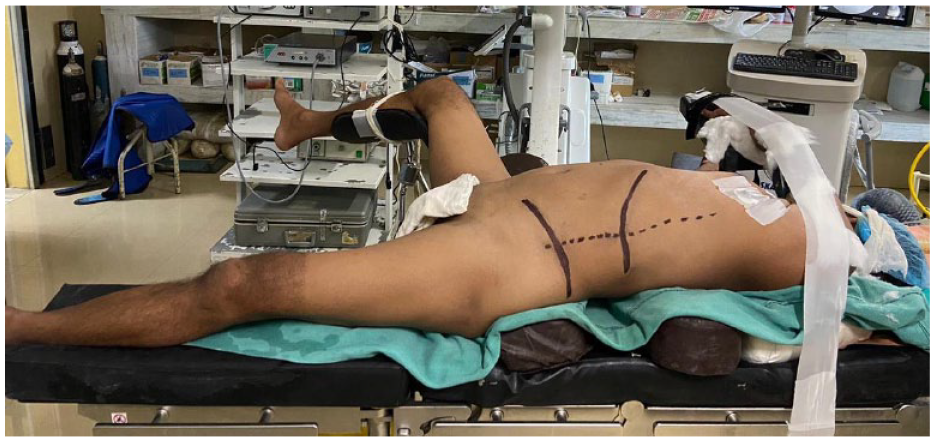
Calcutta position for supine PCNL for left renal calculus.
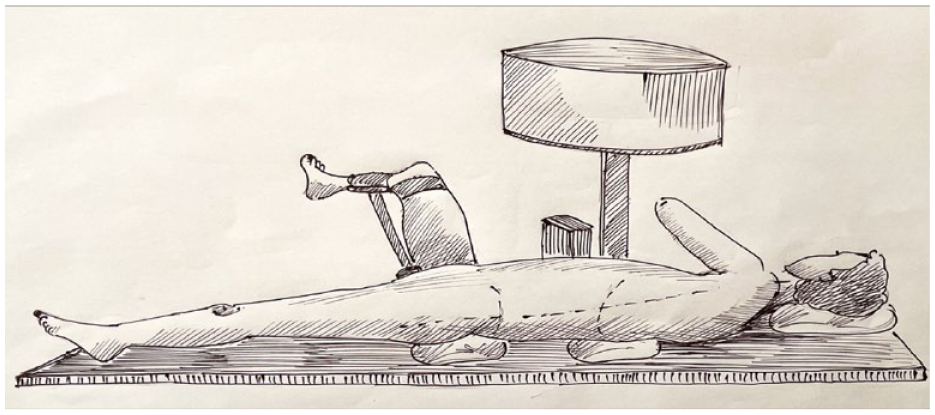
Schematic diagram showing Calcutta position for left renal calculus.

Calcutta position for supine PCNL for right renal calculus.
Schematic diagram showing Calcutta position for right renal calculus.
Two bolsters were placed in horizontally to the torso, one below the shoulder and another below the hip. The ipsilateral arm was brought across the chest to the contralateral side and supported on a stirrup to avoid any stretch over the brachial plexus. A tilt of 10°−15° was achieved by the bolster below the shoulder only. This decreases the torque compared to Galdako-Valdivia position (Figures 1–4). This manoeuvre also kept the flank free for adequate puncture access compared to the Valdivia’s position for supine PCNL where a bolster was placed at the flank or complete supine PCNL where the flank was less exposed. This made use of image-guided access relatively easier. Fluoroscopy was easier and more conventional in Calcutta position (antero-posterior view can be obtained with minimal rotation). The surgeon’s hands being away from the operative and radiological field hence there is less danger of radiation exposure during fluoroscopy. The C-arm could be manoeuvred both cranio-caudally and antero-posteriorly in this position of the patient with no hindrance.
This position gave access to a simultaneous ureteroscopic approach if required similar to other supine PCNL. The added advantage was that the prolonged procedure did not cause any sacral plexus injury.
All the punctures were done fluoroscopy-guided with surgeon doing cystoscopy and retrograde pyelography at first and then doing the puncture. The tracts were secured with a hydrophilic guide wire and coaxial dilatation by Alken metal dilator was done upto required diameter (24/28/30 Fr). 20.8 Fr Wolfe nephroscope is used mostly. If a second puncture was needed we dilated tract upto 18 Fr and mini nephroscope was used. Pneumatic lithotripsy was done with EMS pneumatic lithotripter with 3.00 and 1.00 mm probes for standard and mini nephroscope respectively. After surgery in case of an infected system, bleeding or significant residual stone a nephrostomy tube was kept otherwise Double J stent or ureteric catheter was kept. All patients had undergone catheterisation which was usually removed within 48 h. The operative complications were evaluated according to Modified Clavein Dindo classification. 8
Postoperative care
The post-operative evaluation of the patient was individualised. All patients were evaluated post operatively with an plain X-ray and/or ultra-sonography of kidney ureter and bladder (KUB). In the case of patients requiring any intervention non contrast computed tomography was performed. We considered complete stone clearance and residual fragment of stone up to <4 mm as stone free rate (SFR).
Follow up
The patients were followed up on 3, 6 and 12 months with plain film KUB and/or kidney ultrasonography based on stone characteristics. CT scan was done only if the patients were symptomatic or intervention was planned.
Results
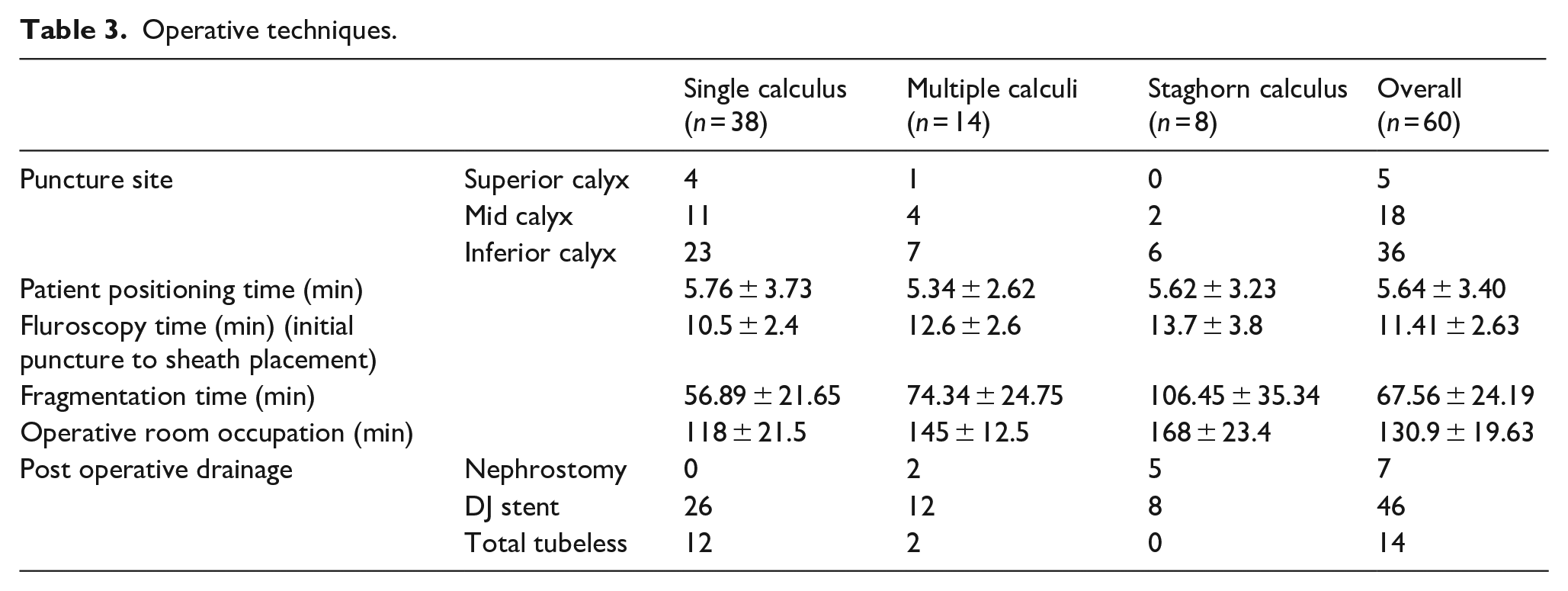
The results are summarised in Tables 1–4. All punctures were done under fluoroscopic guidance. Among these 60 patients, 38 patients had a single puncture and the remaining 22 required a second puncture site for complete clearance of stone. In 31 patients we dilated the nephrostomy tract upto 24 Fr, in 18 patients upto 28 Fr and in 11 patients upto 30 Fr.
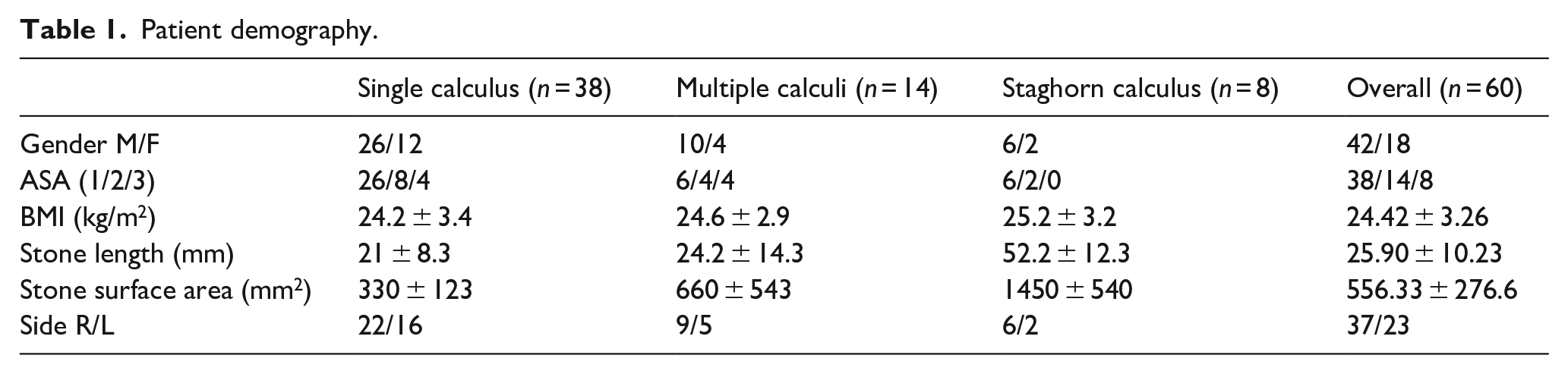
Patient demography.
Supine PCNL in Calcutta position in special situations.
Operative techniques.
Post operative evaluation.
The mean time required for patient positioning, fluoroscopic time (puncture to sheath placement), fragmentation time and overall OR occupation time were 5.64 ± 3.40, 11.41 ± 2.63, 67.56 ± 24.19 and 130.9 ± 19.63 min respectively. No intraoperative complication was noted during the whole series. The post-operative drainage was individualised. Forty six patients underwent Double J (DJ) stent placement. Fourteen patients had an ureteric catheter placed which was taken out within 24 h, and seven patients required nephrostomy tube placement either due to haemorrhage or residual stone. Nephrostomy tube if placed was removed within 2 days post-operatively.
Discussion
Percutaneous nephrolithotomy (PCNL) has shown beyond doubt its efficacy and stood the test of time for management of kidney stones and other related renal diseases when compared to open surgical methods and extracorporeal shock wave lithotripsy. 9 Most of the pioneers who gradually established the operative procedures of PCNL were in an accord to choose prone position for PCNL.3,10 However none of their reports provided a logic for prone position. Even after that it became the standard and remained the only practised position in PCNL for almost two decades. 11
Prone position for PCNL has some drawbacks, which includes ventilator and circulatory difficulties as well as patient discomfort, more common among the in obese patients. 12 Prone positioning may lead to increased intraocular pressure (IOP), which reduces perfusion pressure to the optic nerve and may cause vision loss. 13 Direct pressure to the periorbital region can lead to increased intraocular pressure and loss of vision as the result of central retinal artery occlusion. 14 The change of position during the procedure is also a clumsy task, because usually ureteral catheter are placed in the lithotomy position before positioning the patient to prone. 15 As patients are usually anesthetised in supine position, turning them to prone is both time consuming and has the risk of neck and limb injury and dislodgement of the endotracheal tube. In some occasions where patients are unable to lie prone due to their body habitus such as ankylosing spondylitis, severe lordosis or kyphosis or hip or lower limb contractures supine PCNL is ideal. 9 So supine position for PCNL has have several advantages over other positions for surgeons, anaesthetists as well as patients.
The increased chances of colonic and splanchnic injury in the supine position is not established. On the contrary, the colon is moved laterally and posteriorly to the kidney in the prone position due to abdominal compression.15,16 In the supine position, the colon floats away from the kidney making the colon less vulnerable to injury. However, this difference being only hypothetical, the wisest way to avoid colonic injury is to preoperatively evaluate and plan with CT scans and puncture under ultrasound guidance. 17 In Calcutta position as the ipsilateral side of our patients remains completely supine there is less chances of colon injury as shown by Falahatkar and Allahkah 18 in his complete supine PCNL procedure.
Although severe anaesthetic complications are seldom seen in prone position but anaesthetist are more comfortable with supine position of the patients especially obese patients and high risk anaesthetic patients.19,20 As little irrigation fluid falls on the patient, the risk of hypothermia is also decreased. As the kidney remains in its normal anatomical position, anterior displacement of kidney is also less common compared to the modified supine position or prone position. 21 Despite the fact that the supine position is being accepted more and more and becoming popular worldwide, many urologists still remain reluctant to use any method other than the classical prone position or its variants.22,23
The Calcutta position as described has some inherent benefits apart from all the advantages of supine PCNL. This position circumvent the limitations of nephroscope manouverability and surgeon’s ergonomics of Galdako-Valdivia position. Giusti’s position was previously developed to overcome the potential difficulties of nephroscope manouverability of Galdako-Valdivia position. In Giusti’s position a cushion was placed vertical to the torso under the patients flank for rotation. In ideal condition a standard swim noodle having an approximate diameter of 7 cm is placed to reach a rotation not further than 15°–20°. 24 In our position we had placed two small bolsters, one below the shoulder and one below the hip horizontal to the torso of the patient attaining a tilt of about 10°−15° only at the shoulder limiting the torque. In Calcutta position the flank is kept free providing more space for puncture as well as nephroscope manouverability. The ipsilateral straight leg also gives more ergonomical advantage of reaching the superior calyx from lower calyceal puncture. This also decreases the number of pressure points as well as risk of sacral plexus injury and deep vein thrombosis. The C-arm can be rotated in both cranio-caudal and antero-posterior axis assisting in more accurate multiplaner puncture. A major drawback of conventional supine PCNL is fluoroscopic overlap of vertebra over renal calyces and stone. It is eliminated due to limited tilt of torso in Calcutta position. Average fluoroscopic time of 11.41 ± 2.63 min was comparatively less than previous study of about 16 min. 25
In our study we had performed supine PCNL in Calcutta position for almost all types of stones, various body habitus and variable kidney morphology with almost comparable results with other literature. We achieved a stone free rate of 78% which is comparable to other positions of supine PCNL.9,21
Conclusions
The Calcutta position for supine PCNL is modified technique which may change the approach for supine PCNL in near future. In this early experience of ours we have achieved almost comparable results compared to recent literature in almost all varieties of stone and stone burden as well as multiple difficult scenarios. As our experiences grow this Calcutta position will gain acceptance among urologist in near future. Although this study has a limited sample size a larger comparative study will definitely explain all the pros and cons of this approach.
Footnotes
Acknowledgements
We would like to express our special thanks of gratitude to our patients and staff in Urology Department, IPGME&R.
Author contributions
Dr Sunirmal Choudhury: Conception, design, supervision, processing, writing, critical view. Dr Partha Pratim Sinha Roy: Design, materials, data collection, analysis, interpretation and writing, literature review. Dr Dilip Kumar Pal: Conception, design, analysis, interpretation, critical review. All authors have read and approved the manuscript.
Consent for publication
All the authors have unanimously given consent for this article to be published in your esteemed journal.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent for participation
Approved by Institutional Ethics Committee. Institute name: Institute of Post Graduate Medical Education and Research, Kolkata, India. Approval No. IPGME&R/IEC/2021/375. Date-22/07/2021.
Availability of data and material
All the data including master chart, operative details are available at your earliest request.
Patient consent
Obtained.