
Abstract
Objective:
To evaluate the influence of endogenous testosterone density (ETD) and tumor load density (TLD) in the surgical specimen of prostate cancer (PCa) patients.
Methods:
ETD was assessed as the ratio of endogenous testosterone (ET) to prostate volume (PV). TLD was calculated as the ratio of tumor load (TL) to prostate weight. Preoperative prostate-specific antigen relative densities (PSAD) and percentage of biopsy-positive cores (BPCD) were also assessed. The association of high TLD (above the first quartile) with clinical and pathological factors was assessed by the logistic regression model (univariate and multivariate analysis).
Results:
Between November 2014 and December 2019, ET was measured in 805 cases treated with radical prostatectomy (RP). Median (IQR) of ET and ETD was 412 (321.4–519 ng/dL) and 9.8 (6.8–14.4 ng/(dLxmL)) as well as for TL and TLD was 20 (10-30%) and 0.33 (0.17-0.58%/gr), respectively. As a result, high TLD was detected in 75% of cases. A positive independent association was found between high TLD and ETD. Accordingly, as ETD levels increased, the risk of detecting high TLD in the surgical specimen increased, regardless of PSAD and BPCD.
Conclusions:
At diagnosis of PCa, a positive independent association was found between ETD and risk of high TLD. Subjects with increasing ETD levels were more likely to have high TLD, associated with unfavorable pathology features. The positive association between ETD and TLD in the prostate microenvironment might adversely influence PCa’s natural history.
Keywords
Introduction
Prostate cancer (PCa) is a major health problem in all developing countries, being the second most diagnosed tumor in the aging male.1,2 Although clinically localized disease is the most likely, it does not represent a homogenous category. According to the European Association of Urology (EAU) and National Comprehensive Cancer Network (NCCN) guidelines, three PCa categories can be identified according to the risk of biochemical recurrence; however, the two systems are not equivalent for the latter regarding the inclusion of more advanced tumor stages (cT2c) in the intermediate risk class.1,2 The new tumor grading system, formulated by the International Society of Urological Pathology (ISUP), is considered in both systems and predicts the risk of disease progression more accurately than the Gleason system.1–4 Correctly classifying PCa patients into clinical risk categories is pivotal for discussing treatment options, ranging from monitoring strategies such as active surveillance (AS) and watchful waiting to active treatments, including radical prostatectomy (RP), conformal radiation therapy (RT) and brachytherapy.1,2 However, the detection of unfavorable disease in the prostate specimen (intermediate/high-grade cancers, extracapsular extension (ECE), seminal vesicle invasion (SVI), and positive surgical margins) is a concern for prognostic drawbacks.1,2 While tumor quantitation is pivotal for biopsy specimens, it is still optional for prostatectomy specimens, where it is assessed as the percentage of prostate gland involved by cancer. 1 This is an issue because tumor quantitation in biopsy specimens has been shown to be an independent predictor of aggressive disease in surgical specimens.1,2 Efforts are needed to identify more reliable routine predictors of tumor load (TL) that associates with unfavorable PCa. PCa risk has been related to genetic, dietary, environmental, physical (obesity, metabolic syndrome), and hormonal factors. 1 Endogenous testosterone (ET) is an important marker of prostate growing disorders including benign prostatic hyperplasia (BPH) and PCa, which often coexist. Our group has extensively investigated the role of ET in PCa biology, finding that it may be associated with several unfavorable prognostic factors.5–8 Recently, we focused on the association of ET density (ETD), defined as the ratio of ET to prostate volume (PV), with PCa biology. In low-risk PCa, we recently showed that, in the prostate surgical specimen, ETD was an independent predictor of the risk of high TL as well as TL density (TLD), defined as the ratio of TL to prostate weight.9,10 In intermediate-risk disease, we have also demonstrated that ETD is positively associated with high TL, which predicts unfavorable disease. 11 In this study, we aimed to test the hypothesis of ETD as a predictor of TLD.
Materials and methods
Study population, evaluation of clinical and pathological features
Institutional Review Board approval was obtained from Azienda Ospedaliera Universitaria Integrata of Verona’s ethical committee. Informed consent for data analysis and publication was obtained for all subjects. Data were collected prospectively but evaluated retrospectively. In a period from November 2014 to December 2019, 805 consecutive PCa patients who did not undergo androgen blockade underwent ET (ng/dL) measurement at our laboratory before surgery, and the test was performed at least 1 month after biopsies between 8.00 and 8.30 a.m. by radioimmunoassay. PSA (ng/mL), age (years), BMI (kg/m2), PV (mL), and percentage of biopsy-positive cores (BPC), defined as the ratio of positive to total cores taken (%), were assessed. PV was calculated by standard TRUS methods. In our Institution, the 14-core transperineal technique was used. In each case, the ratios of BPC, PSA, and ET to PV were calculated, and the relative densities were reported as BPCD (%/mL), PSAD (ng/ml2), and ETD (ng/(dL × mL)), respectively. Clinical staging was assessed according to the 2017 version of the TNM system (eighth edition). Patients were classified into risk classes, as recommended by the EAU guidelines. 1 Preoperative physical status was assessed by the American Society of Anesthesiologists (ASA) system. Surgery was performed by experienced surgeons, either by robotic-assisted radical prostatectomy (RARP) or open approach. Extended pelvic lymph nodes dissection (ePLND) was performed according to guidelines.1,2,8 Prostates were weighted and tumors were graded according to the ISUP system.1–4 Tumor quantitation was assessed as TL, which was defined as the percentage of prostate involved by cancer; specifically, our dedicated pathologist assessed tumor quantitation by visual estimation of all the glass slides after all microscopically identifiable foci of carcinoma were circled with a marked pen, as considered by ISUP association. 12 TLD was calculated as the ratio of TL to prostate weight (%/gr). Surgical margins were stated positive when cancer invaded the inked surface of the specimen. Removed lymph nodes were counted and assessed for cancer invasion. Prostate surgical specimens were staged according to the 2017 version of the TNM system (eighth edition).1,2
Study design and evaluation of primary endpoints
The study investigates the association between preoperative ETD and high TLD in the surgical specimen. The former was evaluated as a continuous variable while the latter as TLD above the first quartile; furthermore, densities relative to PSA and BPC were computed as PSAD > 0.14 (ng/ml2) and BPCD ⩾ median and then assessed as predictors of the risk of high TLD, along with other clinical and pathological factors.
Statistical methods
Continuous variables were measured by means (standard deviation, SD) and medians (interquartile range, IQR). Categorical factors were assessed by frequencies (percentages). Associations between clinical and pathological factors with the risk of high TLD were evaluated by logistic regression model (univariate and multivariate analysis).
The discriminatory performance of significant clinical variables was evaluated by plotting a receiver operating curve (ROC) for each predictor and then computing the area under the curve (AUC). The software used to run the analysis was IBM-SPSS version 26. All tests were two-sided, and p < 0.05 was considered an index of statistical significance.
Results
Demographics of the patient population
The overall cohort included 805 cases operated for clinically localized PCa. Demographics and variations in clinical and pathological parameters are reported in Table 1. According to the EAU system, 172 cases (21.4%) were low-risk, 430 (53.4%) were intermediate-risk and 203 (25.2%) were high-risk. Preoperative physical status was coded ASA I in 82 cases (10.2%), ASA II in 654 patients (81.2%), and ASA III in 69 (8.6%) subjects. Surgery was performed by robotic approach in 715 (88.8%) patients. ePLND was performed in 617 (76.5%) cases, of whom 70 (11.4%) had tumor invasion. The median (IQR) of lymph nodes counted was 28 (24–35). Features of unfavorable tumor grade and stage are detailed in Table 1. The Median (IQR) of ET and ETD was 412 (321.4–519 ng/dL) and 9.8 (6.8–14.4 ng/(dL × mL)), respectively. The median (IQR) of TL and TLD were 20 (10-30%) and 0.33 (0.17-0.58%/gr), respectively.
Demographics of 805 prostate cancer patients treated with radical prostatectomy.
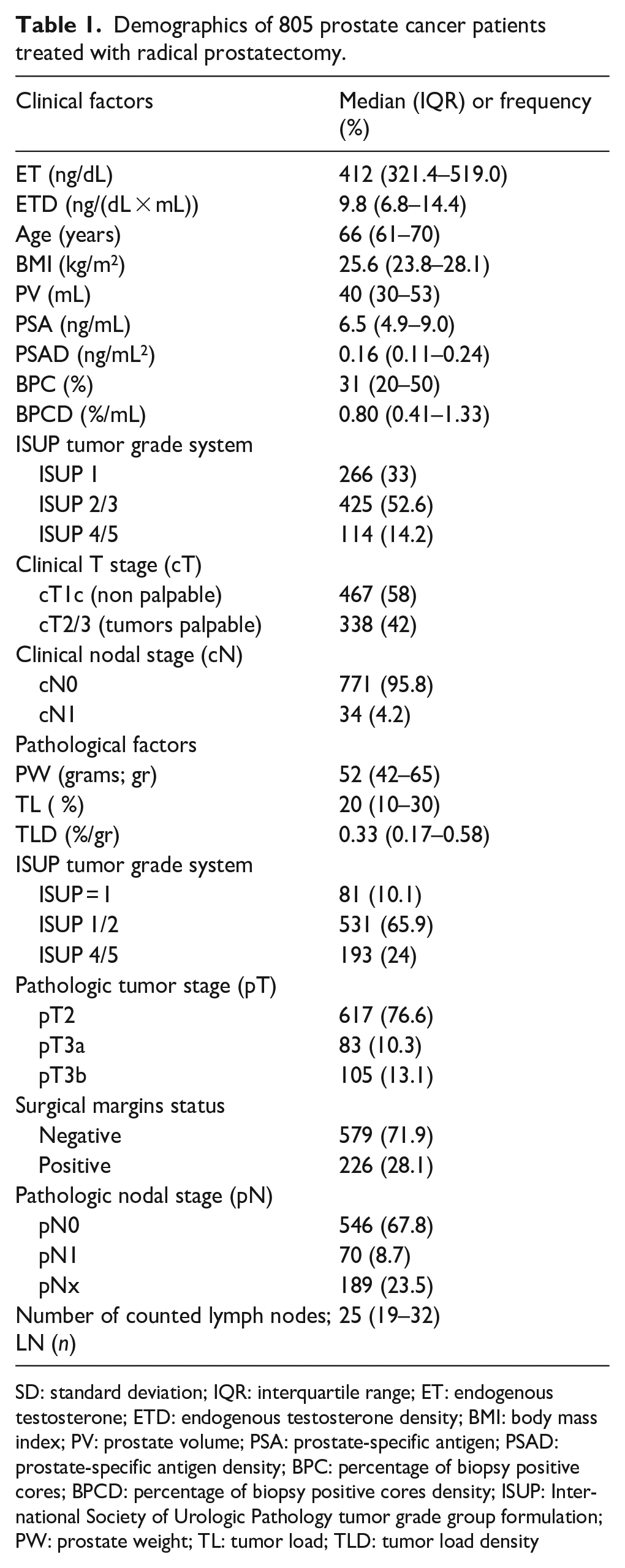
SD: standard deviation; IQR: interquartile range; ET: endogenous testosterone; ETD: endogenous testosterone density; BMI: body mass index; PV: prostate volume; PSA: prostate-specific antigen; PSAD: prostate-specific antigen density; BPC: percentage of biopsy positive cores; BPCD: percentage of biopsy positive cores density; ISUP: International Society of Urologic Pathology tumor grade group formulation; PW: prostate weight; TL: tumor load; TLD: tumor load density
Associations of high TLD with ETD and other parameters
Table 2 shows the associations between high TLD and clinical and pathological parameters. Accordingly, high TLD was found in 75% of cases. A positive association was found between high TLD and ETD as well as with other unfavorable clinical and pathological features. The positive association between high TLD and ETD remained independent after adjusting for BMI and all other clinical parameters, of which only PSAD > 0.14 and BPCD above the median (>0.80%/mL) remained significant. BPC ⩾ 50%, ISUP grade groups 2/3 through 4/5, which were significant on univariate analysis, lost significance in the multivariate model. Other clinical parameters showed no association. In the surgical specimen, high TLD was associated with increasing an increase in undifferentiated tumors that were more likely to have an unfavorable stage for ECE, as well as SVI and positive surgical margins; moreover, pelvic lymph nodes invasion, which was significant on univariate analysis, lost significance in the multivariate model, as shown in Table 2.
Factors predicting high tumor load density (TLD) in the surgical specimen of 805 prostate cancer patients treated with radical prostatectomy.
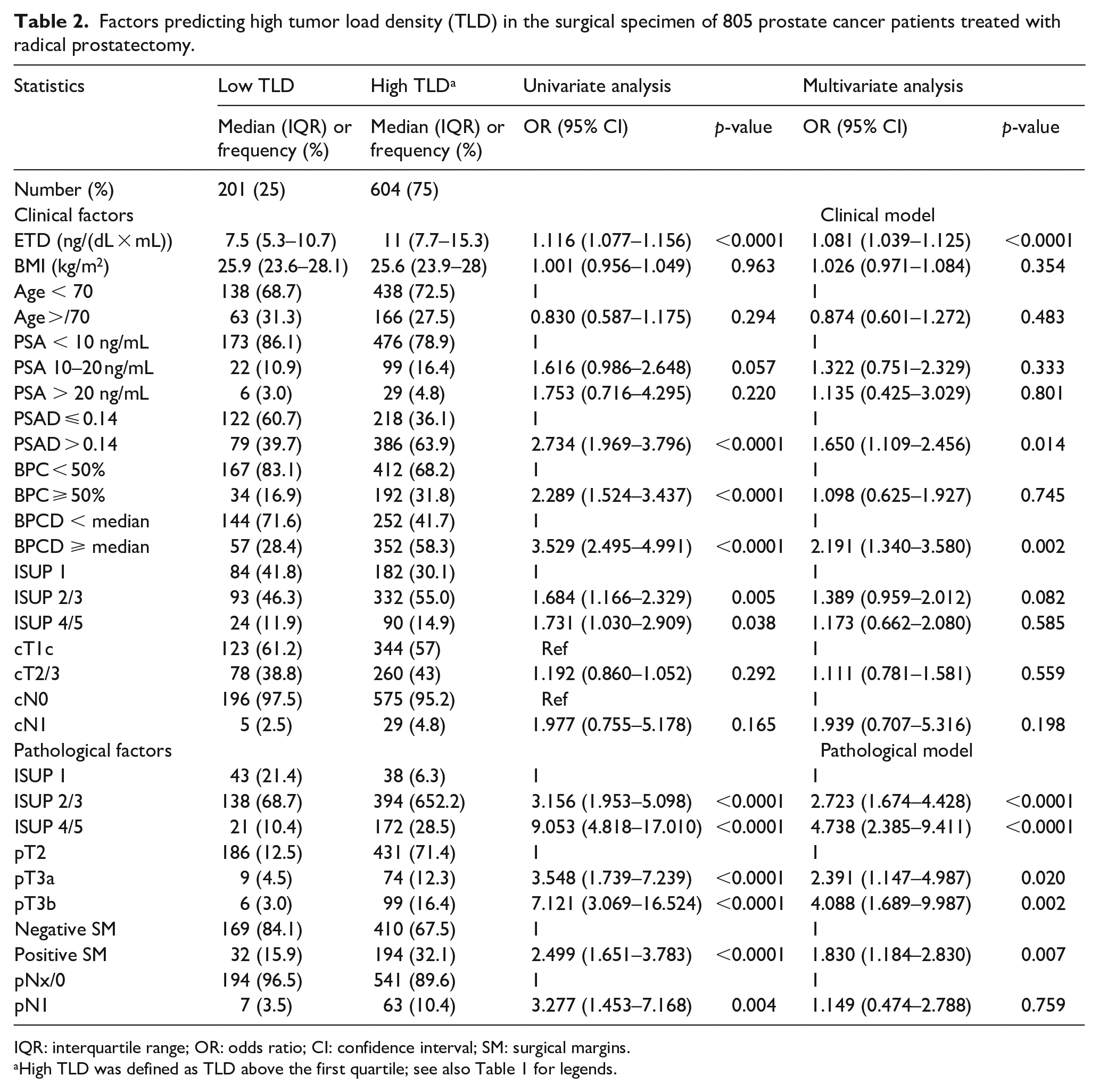
IQR: interquartile range; OR: odds ratio; CI: confidence interval; SM: surgical margins.
High TLD was defined as TLD above the first quartile; see also Table 1 for legends.
The clinical impact of ETD on predicting the risk of high TLD
The independent impact of preoperative ETD on the risk of high TLD in the surgical specimen is summarized in Table 3. Accordingly, as ETD levels increased, the risk of detecting high TLD in the surgical specimen increased, regardless of other clinical parameters, including PSAD > 0.14 (ng/ml2) and BPCD ⩾ 0.80 (%/gr), which remained significant. Further details are reported in Table 3. Figure 1 shows the positive association between preoperative ETD and the risk of high TLD, while Figure 2 shows the discriminatory performance of ROC curves for ETD, PSAD, and BPCD, evaluated as continuous variables, in predicting high TLD in the surgical specimen. Details are reported in the legend of each figure.
The impact of endogenous testosterone density (ETD) in models predicting the risk of high tumor load density (TLD) in 805 prostate cancer patients treated with radical prostatectomy.
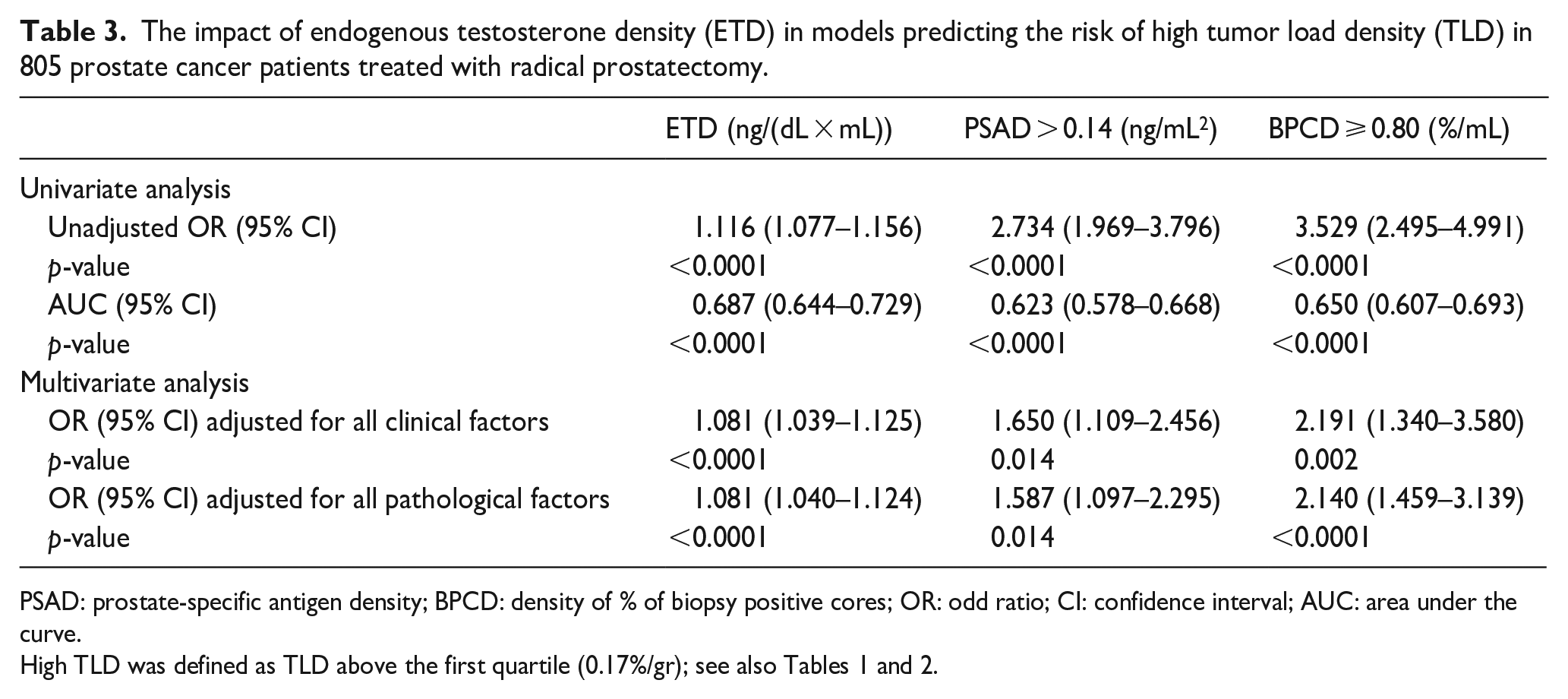
PSAD: prostate-specific antigen density; BPCD: density of % of biopsy positive cores; OR: odd ratio; CI: confidence interval; AUC: area under the curve.
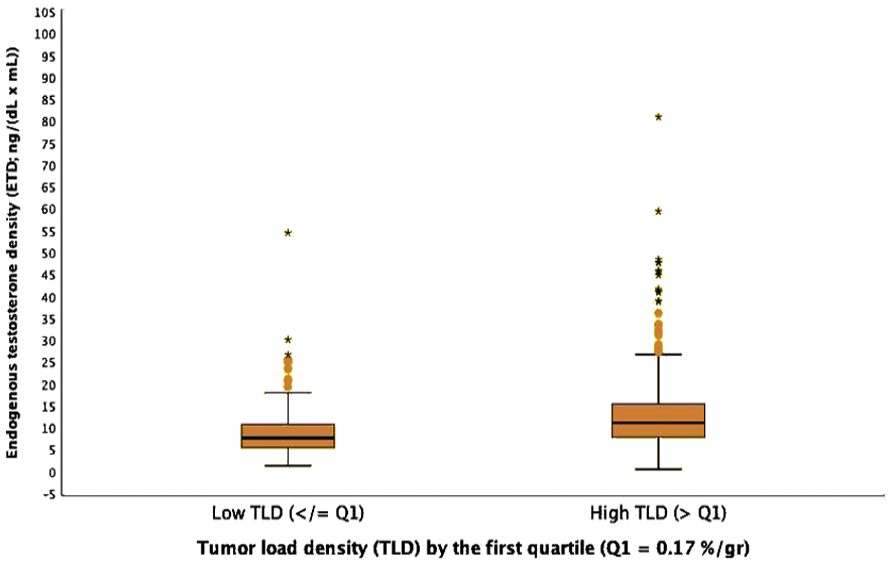
The diagram shows the positive association between preoperative endogenous testosterone density (ETD), the ratio of endogenous testosterone to prostate volume, and high tumor load density (TLD) in the surgical specimen, defined as the ratio of TLD to prostate weight. Accordingly, increasing ETD levels are associated with the risk of high TLD, defined as values above the first quartile (odds ratio, OR = 1.116; 95% CI: 1.077–1.156; p < 0.0001). For further details, see Tables 2 and 3 and the results.
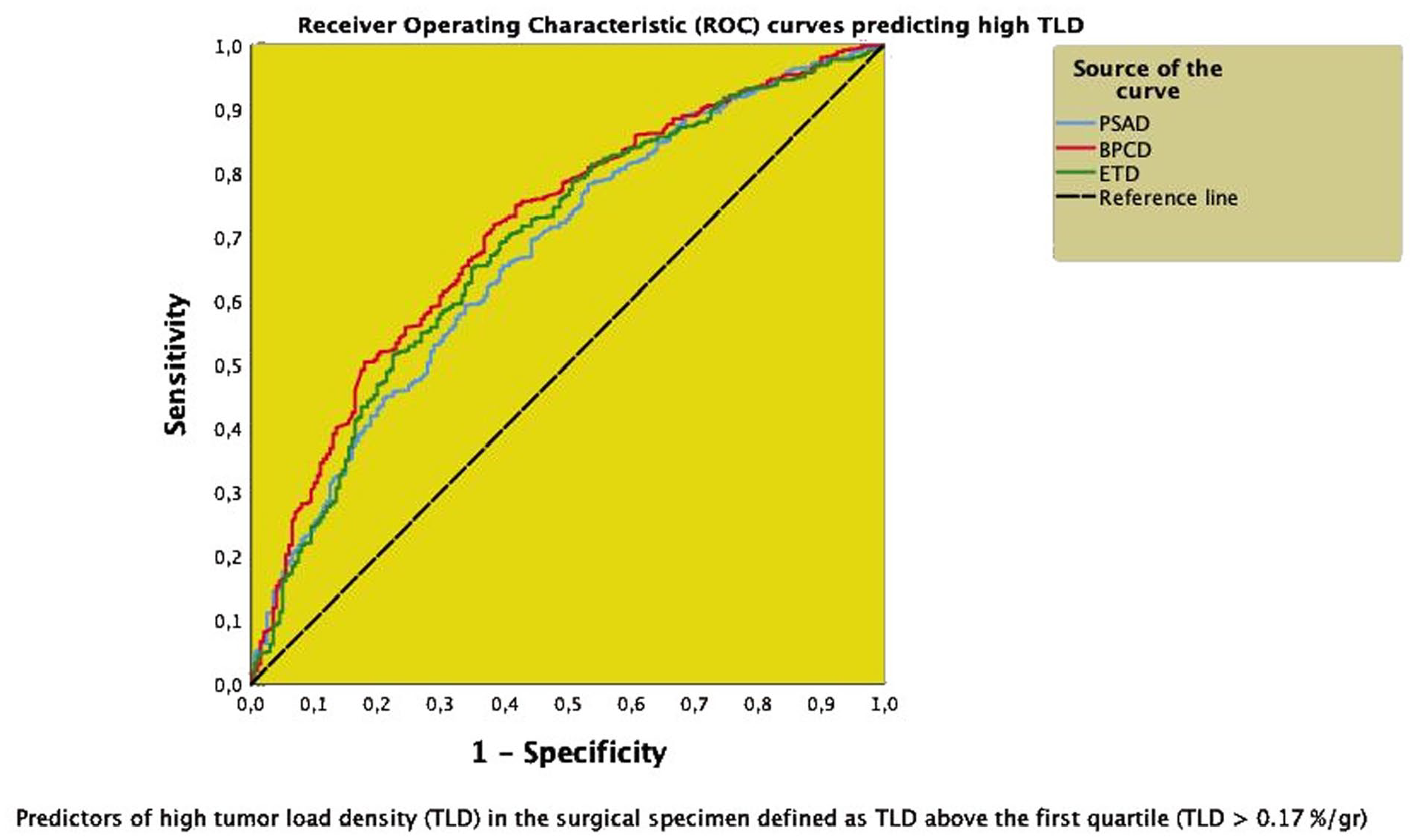
Comparing receiver operating curves (ROC) of endogenous testosterone density (ETD), prostate-specific antigen density (PSAD), and biopsy-positive core percentage density (BPCD), assessed as continuous variables, to predict the risk of high tumor load density (TLD), the ratio of tumor load to prostate weight, assessed as above the first quartile. The discriminatory power of each curve was evaluated as the area under the curve. Accordingly, the discriminatory power of ETD (AUC = 0.687; 95% CI: 0.644–0.729; p < 0.0001) was closer to BPCD (AUC = 0.710; 95% CI: 0.670–0.751; p < 0.0001) but larger than PSAD (0.673; 95% CI: 0.630–0.715; p < 0.0001). See also Figure 1, Tables 2 and 3, and results for further details.
Discussion
Currently, the ISUP grading group is the most important system for predicting the natural history of PCa after primary treatment; moreover, it has been incorporated into the main systems for stratifying patients into prognostic risk classes.1,2 As tumor grade increases along groups, the 5-year biochemical risk-free survival also decreases.3,4 For example, 5-year biochemical risk-free survival of grade groups 1–5 after RP was 96%, 88%, 63%, 48%, and 26%, respectively; moreover, the hazard ratios of groups 2–5 were 2.2, 7.3, 12.3, and 23.9, accordingly. 3 However, tumor upgrading in the surgical specimen remains an issue.1–4 Our study showed a positive association between specimen tumor quantitation and the ISUP system. As tumor grade increased across groups, patients were more likely to have high TLD in the specimen, regardless of ECE and/or SVI. On the other hand, high TLD was independently predicted by the clinical density factors, including PSAD, BPCD, and ETD. The association of clinical density factors with a pathological factor (TLD) is novel for the literature dealing with this topic. Interestingly, as preoperative ETD increased, the risk of detecting high TLD increased; therefore, patients with increasing ETD at diagnosis were more likely to have tumors with unfavorable grade and stage in the surgical specimen, which are predictors of unfavorable prognosis.
As the ISUP tumor grade system, tumor quantitation in both biopsy and prostate specimens is an important parameter for assessing PCa biology. However, only the former is widely used to predict the risk of tumor upgrading, upstaging, and the risk of lymph node invasion, while the latter, although reported in a standard model by the pathologist, is rarely considered.1,2,12 Indeed, biopsy tumor quantitation has been shown to be an effective prognostic parameter for stratifying low- and intermediate-risk patients in the NCCN system and CAPRA system.1,2,13 Currently, biopsy tumor quantitation is the main parameter included in the most accurate nomograms for predicting lymph node invasion. 14 Recently, a multicenter study, while showing that currently available nomograms have similar performances and limitations, also demonstrated that the older nomograms performed better than the updated ones, thus suggesting that multiparametric resonance imaging (mpMRI) parameters did not add relevant information to increase predictive power; furthermore, these results were explained for the high operator dependence of the procedure. 15 In addition, tumor quantitation together with the ISUP system represent important parameters for managing AS protocols.1,2 On the other hand, tumor quantitation evaluated as TL is also an important parameter for the evaluation of PCa biology, being positively associated with tumor grade, extension, and progression. 12 However, current academic literature has almost ignored this important topic.
Our study showed a positive association between high TLD and risk of unfavorable PCa, including cancers associated with adverse pathology by grade and stage. Accordingly, subjects with high TLD were more likely to be associated with tumors with unfavorable pathology. In our opinion, TLD is more effective than TL in assessing tumor features, as it is related to gland density; therefore, prostates with the same tumor loads may show low and high densities, with the latter associating with features of aggressive PCa. For example, the biology of tumors with TL of 10% may be more severe when referred to a gland of 30 gr (TLD = 0.33) instead of 60 gr (TLD = 0.16). This is the first study to demonstrate the efficacy of this parameter, which was independently predicted by ETD, BPCD, and PSAD. These results also correlate with our recent findings showing that BPCD can be predicted by both ETD and PSAD.10,11 In our opinion, these results may have implications for computing future nomograms and stratifying patients within each clinical risk category.
PCa biology is closely related to ET, which has been correlated with aggressive cancer features; however, the topic remains highly controversial because controlled studies are missing and the hormone is not periodically measured, as recommended.16–18 Accordingly, the association between ET and aggressive PCa has been detected as positive, inverse, or null.16,17 In a Japanese study including 82 PCa patients undergoing RP, preoperative ET was an independent predictor of non-organ confined disease after adjusting for PSA and pathological Gleason score; so far, low ET levels were associated with unfavorable disease in the surgical specimen, including high-grade cancer with extra-prostatic extension; however, the study was limited by the number of cases, the retrospective nature and that it was dated. 19 In a larger American study including 326 cases treated with surgery, low preoperative ET levels were associated with advanced disease in the surgical specimen; however, the study was limited by the retrospective nature and for not consider the testosterone diurnal variations. 20 A large study including 879 patients treated with RP showed that lower ET levels predicted advanced-stage disease in the surgical specimen, regardless of PSA and biopsy Gleason score; however, the study was limited by being retrospective and dated. 21 Recently, a large study including 762 patients showed that low ET levels were associated with tumor aggressiveness, as assessed according to the D’Amico risk classes, and metastatic disease; furthermore, it showed that lower ET levels associated with unfavorable disease features in the surgical specimen of 152 patients treated with primary RP; however, this study has several limitations due to being retrospective, including several primary treatments (RP, RT, AS, hormonal therapy), including metastatic cases, and not evaluating PV, PSAD, and tumor quantitation in biopsy and surgical specimens. 22 Our study shows for the first time the importance of evaluating ET and tumor quantitation as density factors. Accordingly, patients with increasing densities of ET, PSA, and BPC are more likely to have high TLD, which associate with the risk of unfavorable pathology in the involved prostate. So far, evaluation of preoperative ETD as PSAD and BPCD is a novel method to assess total testosterone associations in patients diagnosed with PCa.
The findings of our study provide an opportunity to speculate on basic science theories relating ET to PCa biology. A decrease in ET levels occurs physiologically in middle-aged men. 23 Several studies investigating the associations between ET and aggressive PCa have shown that prostate growth is strictly dependent on ET at very low levels, but when ET levels decrease to critical points, testosterone deficiency has negative effects on androgen-dependent cell differentiation and division; moreover, to the extent that prostate cells are continuously exposed to low ET levels, the risk of cancer induction increases.23–25 These theories are supported by the results of our study. ETD, along with other clinical tumor features (PSAD, BPCD) was an independent predictor of high TLD in the surgical specimen. The risk of TLD increased with increasing ETD, thus indicating that a prostate environment with high ETD might hurt cell renewal, with drawbacks associated with cancer induction and progression.
Models for predicting tumor quantitation in prostate specimens are missing. While tumor quantitation in biopsy specimens is an intensively evaluated parameter in several nomograms for predicting disease issues, prostate specimen tumor load is a factor almost ignored in the current academic literature. Our study showed an effective clinical model for evaluating TLD features by ETD and other density parameters, including PSAD and BPCD.
The model could find applications in clinical practice for the evaluation of PCa patients who need further stratification within each clinical risk category for upgrading and upstaging, events that are more likely to occur in the low and favorable intermediate-risk classes, as well as for downgrading and downstaging, events that are more likely to occur in the unfavorable intermediate and high-risk classes, respectively.1,2 Furthermore, when RT is the chosen option, the model might be an effective tool for patient counseling and radiation treatment planning. In addition, the results of our study could be the subject of novel updated nomograms for predicting the risk of unfavorable disease. Finally, prospective clinical trials are needed to confirm our clinical model.
Our study has several limitations. Prostate volumes were not all measured in our institution. ET was measured only once, not periodically, as recommended. 18 A central pathology review of external biopsies was not performed. Results of mpMRI were not evaluated for not being available in all patients. Genetic tests were not performed. Analysis of maximal cancer involvement of each core was not computed for not being available in all patients. Finally, the nature of the study was retrospective. Our study has strengths, as well. All prostate specimens were assessed by our dedicated pathologist. ET was measured in the morning which is the appropriate interval for evaluating the levels of the hormone, which decreases in the afternoon. 26 Data were prospectively collected. It was a single-center study and the patient population was homogenous for ethnicity (Caucasian) and for ET measurements, which were all performed at our laboratory.
Conclusions
At diagnosis of PCa, a positive independent association was found between ETD and risk of high TLD in the surgical specimen. Accordingly, subjects with increasing ETD levels were more likely to have high TLD associated with features of unfavorable pathology, predicting an adverse prognosis. The positive association between endogenous testosterone and tumor load densities in the prostate microenvironment might influence PCa’s natural history adversely.
Footnotes
Acknowledgements
None.
Author contributions
ABP provided the study design and conception, the manuscript’s drafting, statistical analyses, and interpretation of data. A Bianchi, SG, AP, ES, GM, RO, FM, GMP, A Baielli, FA, FD, SV, and DD carried out data collection. FM, RR, AV, AG, MB, AT, MAC, and AA provided supervision and critical revision of the manuscript for important intellectual contents. All authors read and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Institutional review board statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Azienda Ospedaliera Universitaria Integrata of Verona.
Informed consent statement
Informed consent was obtained from all subjects involved in the study.
Data availability statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to ethical reasons.