
Abstract
Objective:
We aimed to identify clinical and radiological predictors of the need for surgical intervention in infants with antenatally detected UPJO.
Material and methods:
We prospectively followed infants born with antenatally diagnosed ureteropelvic junction obstruction (UPJO) presented at our outpatient clinics for evidence of obstructive injury with a standard protocol with ultrasonography and renal scintigraphy. Indications for surgery included progression of hydronephrosis on serial examinations, initial differential renal function (DFR) ⩽35% or >5% loss in sequential studies, and febrile urinary tract infection (UTI). Univariate and multivariate analyses were utilized to define the predictors for surgical intervention, while the appropriate cut-off value of the initial Anteroposterior diameter (APD) was determined using the receiver operator curve analysis.
Results:
Univariate analysis revealed a significant association between surgery, the initial APD, cortical thickness, Society for Fetal Urology grade, UTD risk group, initial DRF, and febrile UTI (p-value < 0.05). No significant association between surgery and sex or side of the affected kidney (p-value 0.91 and 0.38, respectively). On multivariate analysis, the initial APD, initial DRF, obstructed renographic curve, and febrile UTI (p-value < 0.05) were the only independent predictors for surgical intervention. An initial APD of 23 mm can predict surgical requirement, with a specificity of 95% and sensitivity of 70%.
Conclusion:
For antenatally diagnosed UPJO, the APD value (at the age of 1 week), DFR value (at the age of 6–8 weeks), and febrile UTI during follow-up are significant and independent predictors of the need for surgical intervention. APD, when used with a cut-off value of 23 mm, is associated with high specificity and sensitivity for predicting surgical need.
Keywords
Introduction
Antenatal hydronephrosis (ANH) is an increasingly encountered problem due to the widespread use of antenatal ultrasound, it is reported in around 5% of pregnancies. 1 Ureteropelvic Junction Obstruction (UPJO) is the leading cause in most cases and has been managed surgically. 2 However, many series reported an increased rate of spontaneous resolution without any significant renal damage in such cases. 3 So, the management protocol has changed toward initial conservative management with elective surgical intervention in selected cases. However, it is still challenging to identify the candidates for early surgical intervention versus those for watchful waiting. Moreover, another challenge is related to getting the precise cut-off values to shift to surgery. Therefore, we aimed to define those factors that can contribute to the proper selection of those patients.
Patients and methods
This is a prospective cohort study that was performed at two tertiary referral centers (Sohag University Hospital and Abu El Reesh Japanese Children Hospital) between January 2018 and June 2021. The study included all cases with ANH due to primary UPJO, detected antenatally and confirmed postnatally at the age of 1 week without any degree of ureteral dilatation. Parents of included infants were thoroughly informed about the protocol of evaluation and follow-up with possible intervention, and the Ethics Committee approved the study of Sohag University.
The initial workup included a complete clinical examination with an ultrasonographic assessment to measure the following: renal pelvis’s maximum anteroposterior diameter (APD) (in mid-renal transverse plane), the maximal cortical thickness, and the Society for Fetal Urology grade (SFUG) of hydronephrosis. 4 Based on this evaluation, the infants were grouped into three groups (P1: low risk, P2: intermediate risk, P3: high risk) according to the urinary tract dilatation (UTD) classification system. 5 In addition, basic laboratory investigations, including serum creatinine, and urine analysis, were done for all patients.
At the age of (6–8 weeks) after birth, the infants were revaluated with ultrasonography in addition to radioisotope scanning with Diethylenetriamine pentaacetate (DTPA) to record the baseline initial DRF and whether the dilated renal unit demonstrated an obstructed curve or not. Obstruction was defined as progressive retention of the radiotracer within the collecting system with continuous upsloping of the time-activity curve (TAC) even after the diuretic administration. In addition, the washout curve was considered as it is typically more revealing than the absolute half-time values, especially in young children.6,7
Patients with bilateral hydronephrosis were further evaluated with Voiding Cystourethrography (VCUG) to exclude vesicoureteral reflux (VUR). Moreover, at the end of this evaluation, infants who had an initial APD of <10 mm, those with ureteral dilatation, initial serum creatinine >0.7 mg/dl and those with neurologic abnormality have been excluded from the study.
Early surgical intervention (after the initial evaluation) was chosen in patients with initial differential renal function (DFR) ⩽ 35% with an obstructive curve on renogram or progressive increase in the degree of hydronephrosis with parenchymal affection (cortical thickness <5 mm). Otherwise, the patients were managed non-operatively, by performing follow-up ultrasonography (every 3 months in stable or improving cases and every month in progressive cases), Radioisotope Scan (RIS) (every 3 months for those who had progression of their hydronephrosis). Urine culture was performed in case of suspected urinary tract infection (UTI). Prophylactic antibiotic (amoxicillin) was prescribed for high-risk patients (UTD P3) till the age of 1 year or till the time of pyeloplasty if indicated.
The renogram was dismissed for those who had improved the degree of hydronephrosis on two serial examinations. Resolution of hydronephrosis was defined as APD < 10 mm documented on two consecutive examinations. While the shift to surgical treatment is indicated in patients demonstrating progressive hydronephrosis (defined as progressive increase in the APD associated with transition into a higher SFUG or higher UTD risk group confirmed in 2 consecutive scans), deteriorating renal function (loss of >5% in subsequent RIS), or clinical complications (febrile UTI).
In the case of surgical treatment, a standard open dismembered pyeloplasty was performed according to the technique described by (Anderson-Hynes), 8 and the patients were then followed with ultrasonography and urine analysis carried out at 3 monthly intervals to ensure improvement. A radioisotope scan was performed after 6 months to assess the residual renal function and ensure patent drainage.
Data were analyzed using STATA version 14.2. Data were represented as mean ± standard deviation, median, and range (for quantitative data) and as number and percentage (for qualitative data). Receiver operating curve (ROC) analysis was used to detect the best value of different cut-off points. Survival analysis, taking surgery as the endpoint and UTD risk group as a variable, was done using the Kaplan Meier survival and log-rank test. Cox proportional hazard analysis was used to perform univariate and multivariate analysis with surgery as the endpoint. p-Value was considered significant if less than 0.05.
Results
Between January 2018 till June 2021, 188 neonates presented to our departments with antenatally diagnosed hydronephrosis. After clinical and radiological evaluation, 52 patients were found to have dilated ureter either due to obstructive megaureter, VUR, or posterior urethral valve (PUV). In addition, two patients were diagnosed as having multicystic dysplastic kidneys. These cases were excluded from the study to be managed accordingly.
The remaining 134 infants were diagnosed as having PUJO (unilateral in 104 infants and bilateral in 30 infants) with a total of 164 renal units. After the initial assessment, 37 renal units were managed with early surgical intervention (Anderson Hynes pyeloplasty), and the rest (127 renal units) were managed conservatively according to the scheduled protocol. During the period of follow-up, 17 cases (17 renal units) were missed, and these cases were excluded from our study. So finally, we had 117 patients (92 males and 25 females) with a total of 147 renal units. Improvement was reported in 78 renal units (53.06%), complete in 67 units, and partial in 11 units with residual non-progressive hydronephrosis. The mean time of follow-up was 23.2 ± 7.6 months, while the mean time to resolution was 9.0 ± 5.3 months. Patient demographics are demonstrated in (Table 1).
Baseline characteristics of the study group.
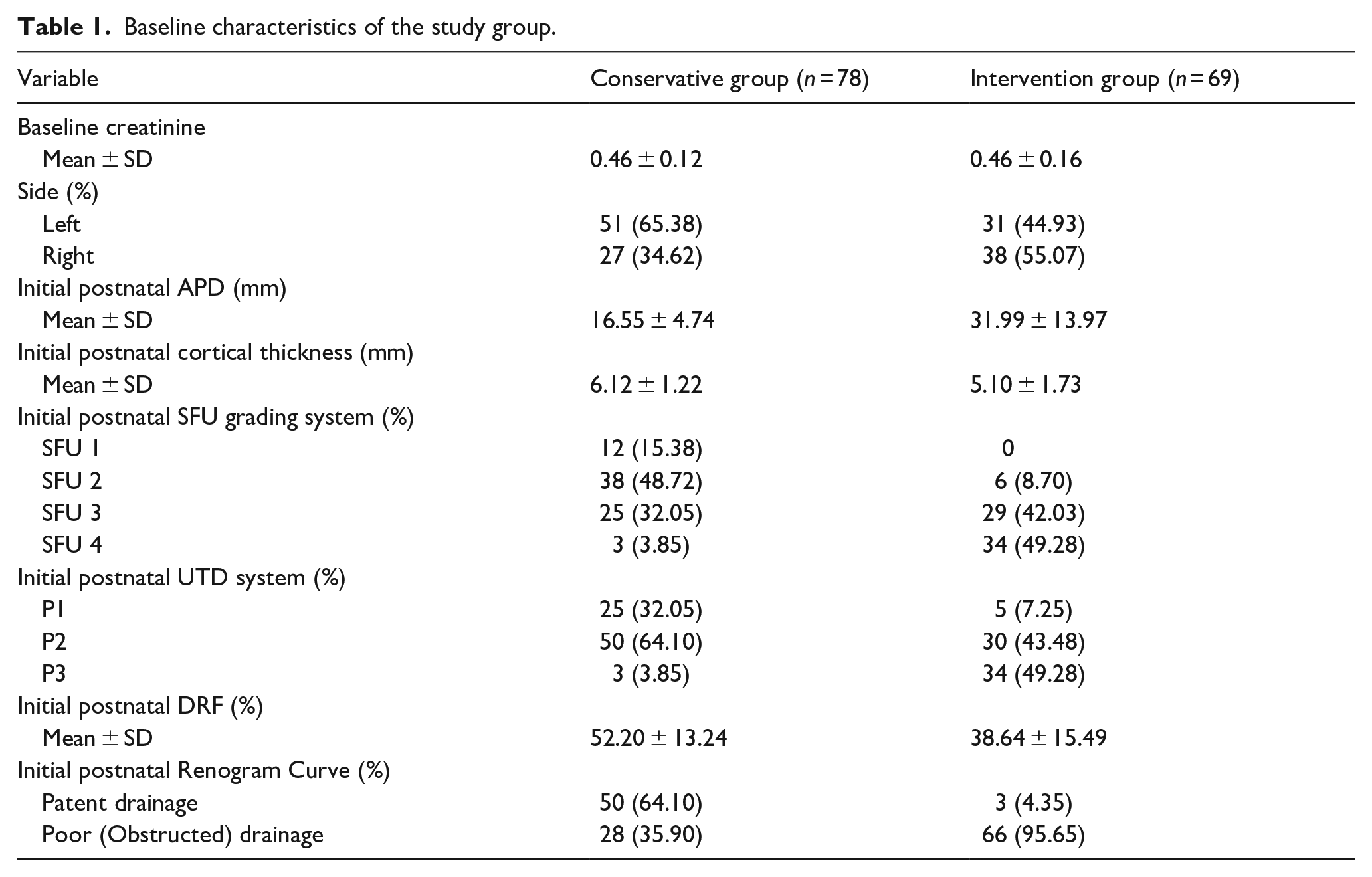
Surgery was needed in 69 renal units (37 after the initial evaluation and 32 after a conservation period). The mean time to surgery was 5.2 ± 3.8 months. Indications for termination of conservative management were >5% loss of renal function in 10 renal units, progression of hydronephrosis in nine renal units, and recurrent UTI in 13 renal units.
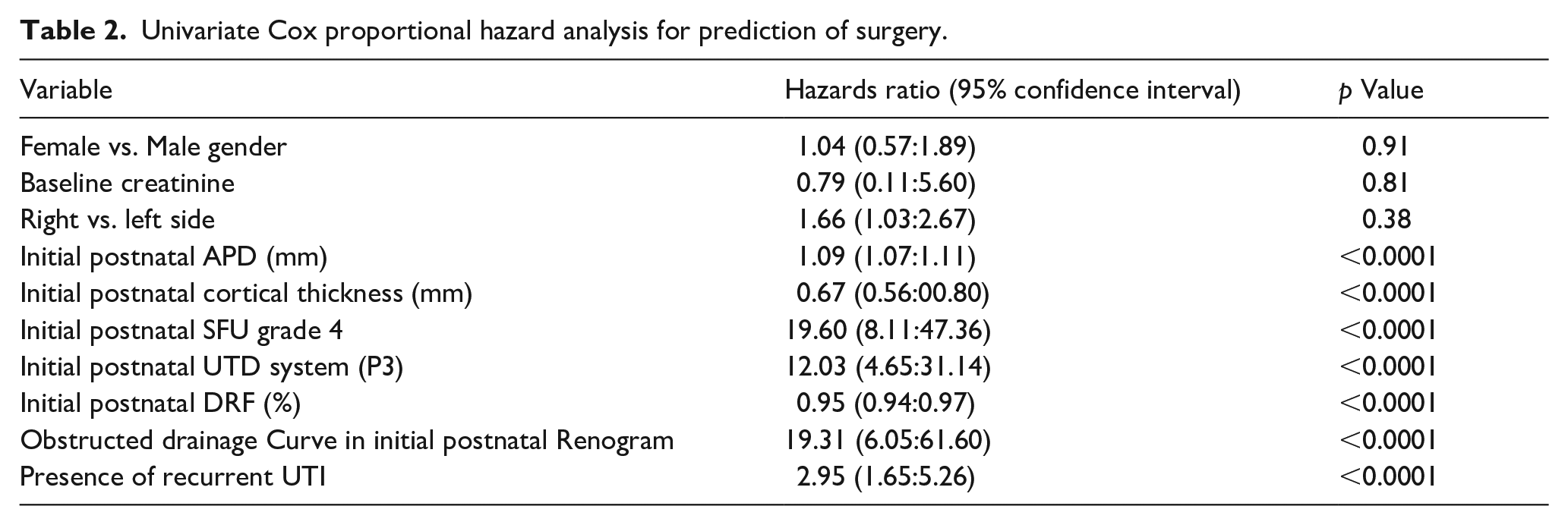
With the statistical analysis of the surgically managed patients, univariate analysis revealed no significant association between surgery and gender or side of UPJO (p-value 0.91 and 0.38, respectively). Furthermore, surgical intervention was linked to the initial grade of hydronephrosis, APD, Cortical Thickness, initial DRF, and occurrence of recurrent UTI (p-value < 0.05) (Table 2). Survival analysis taking the UTD risk group as a variable and surgery as an endpoint revealed that the UTD risk group P3 (high risk) is significantly associated with the need for surgery (Figure 1).
Univariate Cox proportional hazard analysis for prediction of surgery.
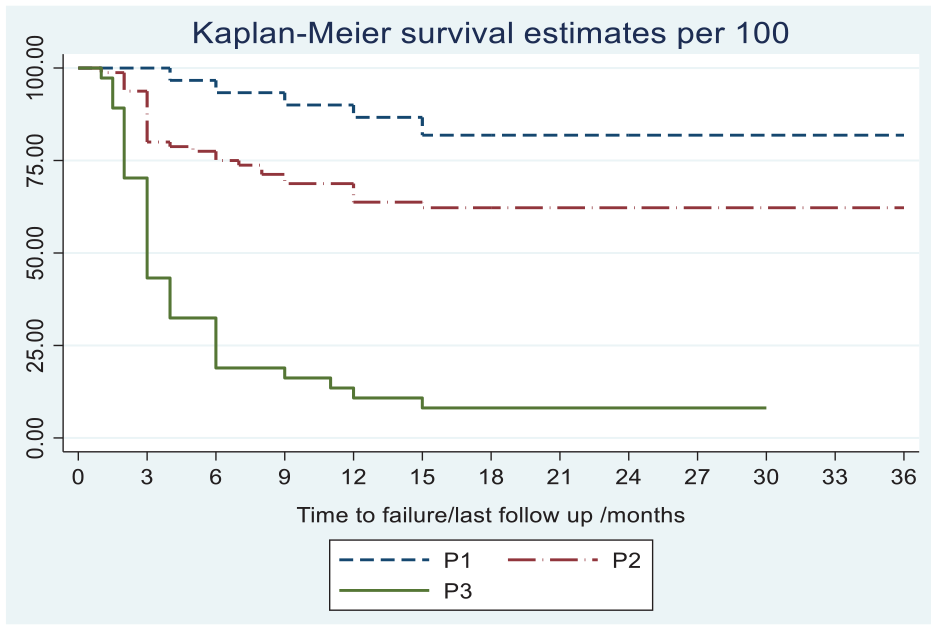
Kaplan-Meier survival analysis showing the association between initial postnatal UTD system and surgery.
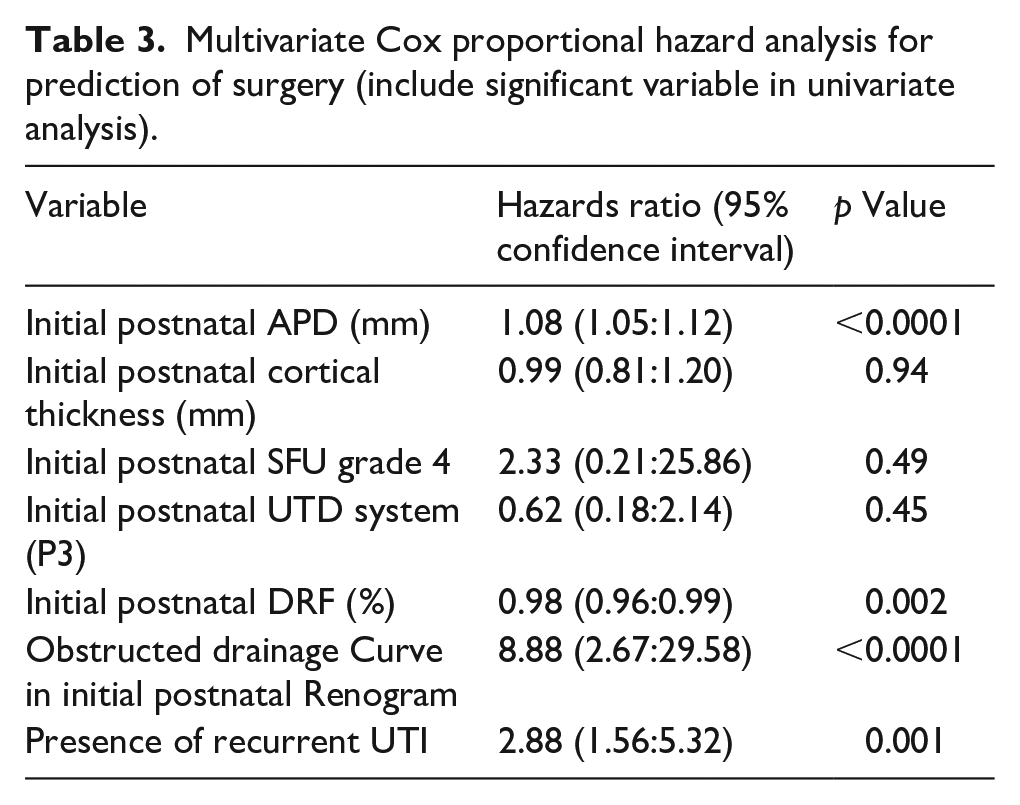
However, on studying our data with the multivariate analysis, the initial APD (p-value < 0.0001), initial DRF (p-value < 0.002), presence of obstructive curve on renogram (p-value < 0.0001), and occurrence of recurrent UTI during follow up (p-value < 0.0001) were the only significant and independent predictors for surgery (Table 3). Using ROC analysis (Figure 2) to determine the sensitivity and specificity of different cut-off values of the initial APD. An initial APD of 23 mm can predict surgical requirement, with a specificity of 94.9% and a sensitivity of 69.6%.
Multivariate Cox proportional hazard analysis for prediction of surgery (include significant variable in univariate analysis).
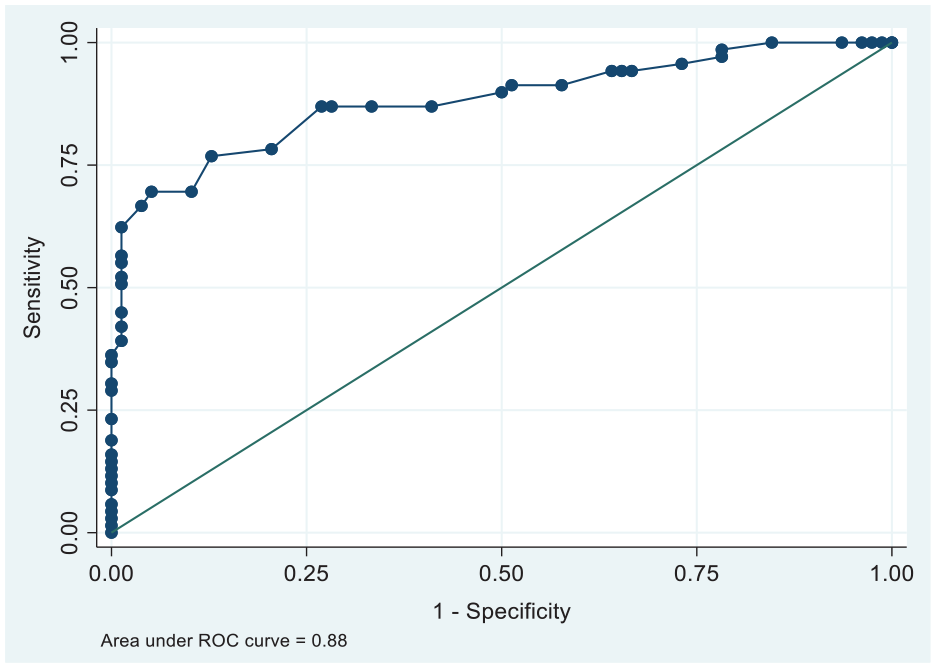
Receiver operating curve for anteroposterior diameter.
Discussion
The therapeutic approach for ANH caused by UPJO has shifted from primary surgical intervention to initial conservative management with elective surgery in selected cases. Although there is general agreement that progressive hydronephrosis, significant DFR impairment, and the presence of symptoms (UTI, pain) are reasonable indications for pyeloplasty, precise cut-offs for the previous factors are still debated.
Many authors recommend expectant management for antenatally diagnosed UPJO,9 –12 which has become standard practice at many centers. The main goal is to avoid unnecessary surgeries while preserving renal function. The argument for that is the high liability for spontaneous resolution, mainly in the first year of life. 13 In this series, we report the resolution of hydronephrosis in 78 renal units (53.06%), including complete in 67 renal units and a partial one in 11 renal units. Many cases had initial criteria that indicate surgical intervention, such as initial high-grade hydronephrosis. However, those patients had improved hydronephrosis during the follow-up. In addition, 28 renal units had an initial obstructed drainage pattern that showed improvement in subsequent studies. Therefore, based on these initial data, those patients successfully managed and avoided unnecessary intervention.
Furthermore, the decisive problem with conservative management is to identify infants in whom renal function will be preserved and those in whom it will deteriorate. In our series, patients were meticulously monitored for anatomical and functional changes. We offered early surgical intervention (within 3 months after birth) for 37 renal units. And for those who were on conservative management, 32 renal units were shifted to surgical intervention due to progressive hydronephrosis, decreased DRF > 5%, or recurrent UTI. The mean time to conservative management failure (time to surgery) was 5.2 months, which was comparable to 5.6 months as reported by Onen et al., 14 and less than other reports of 9–11.15,16
While the indications for surgery in our cohort are comparable to the published literature,14,15,17 our exciting finding was about the 30 patients with bilateral PUJO. Bilateral PUJO does not seem to be a contraindication for an initial trial of conservative management, supposing that the infant has normal chemistry and urine output. Onen et al. 7 have reported a trial of initial conservative management for 19 newborns diagnosed with bilateral PUJO with a high-resolution rate. In our series, we have dealt with each renal unit separately and resolution was reported bilaterally in nine patients and unilaterally in 16 patients. Regarding DTPA results in those patients, the absolute number of DFR was not our primary concern but the pattern of drainage (either obstructive or not), in addition to cortical thickness loss on serial ultrasonographic examinations.
The surgical intervention rate varied widely among several published studies ranging from 12% to 52%.14 –19 In our series, the rate of surgical intervention was 47%, which is considered relatively high. The explanation for this finding is that we work as tertiary referral centers. Most of our patients have higher grades of hydronephrosis as denoted on initial examinations, where 91 renal units (62%) had SFU grades 3–4. A published study by Onen 14 that presents low-rate surgical intervention at 12% shows only 15% of patients with grade 3–4 hydronephrosis. In addition to the relatively smaller sample size, we think that the prospective nature of our study and the frequency of follow-up influenced our surgical intervention rate.
In this cohort, we found that the initial APD, initial DRF with an obstructive curve on renogram, and recurrent UTI were predictors of the need for surgical intervention. While, Cortical thickness, SFU grade 4 hydronephrosis, and UTD P3 (high risk) were not. These results are similar to reports published by other centers.15 –19
Survival analysis taking the UTD risk group as a variable and surgery as an endpoint revealed a significant link between the high-risk group and the need for surgical intervention; however, on the multivariate analysis, this link was found to be insignificant (p-value > 0.05). To the best of our knowledge, this prospective analysis is the first one to address the relation between the UTD system and the need for surgery in antenatally diagnosed UPJO.
Many studies have proposed UTI as an indication for surgical intervention.17,19,20 In our series, despite the antibiotic prophylaxis given to high-risk patients (UTD P3), 21.7% of the operated renal units were associated with recurrent UTIs. Two of our patients were admitted to the intensive care unit for neonatal sepsis. Using ROC analysis, our data revealed that an APD of 23 mm (best cut-off) can portend surgical need, with a specificity of 95% and sensitivity of 70%. With this cut-off value, only 5% of the operated patients might not have undergone surgery if put on conservative management. Some authors reported different cut-off values ranging from 16 21 to 24.3 mm. 15 Based on our data, using a lower APD, for example, 15 mm, can result in unnecessary surgical intervention in up to 58% of the operated cases.
Limitations of our study come from the small number of cases and the relatively short follow-up period. Therefore, a longer period of follow-up is required to assure persistent improvement for both intervention and conservative groups of the study.
Conclusion
In conclusion, for antenatally diagnosed UPJO, the APD value (at the age of 1 week), DFR value (at the age of 6–8 weeks), and occurrence of recurrent UTI during follow-up are significant and independent predictors of the need for surgical intervention. APD, when used with a cut-off value of 23 mm, is associated with high specificity and sensitivity for predicting surgical need.
Footnotes
Acknowledgements
I would like to express my sincere gratitude to my professors Dr. Esam El din Salem, Dr. Abdelmoneim Abouzeid, Dr. Hany Abd Elraoof and Dr. Hazem Elmoghazy who helped me with this work by their excellent guidance, skillful help and endless persistent support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.