
Abstract
Introduction:
The aim of this study was to identify possible risk factors for urethral rupture and to evaluate the effect of urethral rupture repair on long-term functional outcomes and complications.
Materials and methods:
The medical records of consecutive penile fracture patients were retrospectively reviewed. Penile fracture patients with and without urethral rupture were compared according to demographics, clinical and intraoperative findings. Comparisons of postoperative functional results of the groups were performed using the 5-item version of the International Index of Erectile Function (IIEF-5) and the International Prostate Symptom Score (IPSS). Finally, among them, long-term penile complications including penile curvature, painful erection, palpable nodule, and paresthesia were assessed.
Results:
Fifty-three patients participated. Patients with urethral rupture (n = 8) were older (44.50 ± 10.69, 36.58 ± 10.33 years, p = 0.052). There was no significant difference in fracture etiology (p = 0.64). Urethral bleeding was present only in patients with urethral rupture (p < 0.001). Although no bilateral corpus cavernosum rupture was encountered in penile fracture patients without urethral rupture, this rate was significantly higher in those with urethral rupture at a rate of 62.5% (p < 0.001). The time from surgical repair to sexual activity was similar in both groups (p = 0.66). There was no significant difference in IPSS and IIEF-5 scores, the presence of erectile dysfunction and complication rates (p > 0.05).
Conclusions:
Older age is a possible risk factor for a concomitant urethral rupture with penile fracture and it seems to be associated with urethral bleeding and bilateral corpus cavernosum involvement. Additionally, urethral rupture repair neither adversely affected functional outcomes nor increased penile complication rates.
Introduction
Penile fracture is a transverse tear of the tunica albuginea and is often caused by sexual intercourse with a prevalence of about 1/100,000. 1 Since penile fracture is rare, concomitant urethral rupture has only been reported as case reports or case series in the literature. The reported frequency of concomitant urethral rupture is variable at 1.4%–23.5%. A concomitant urethral injury complicates penile fractures and requires specialized management. 10 In the presence of concomitant urethral rupture, delayed surgery or conservative management is not recommended.10,11 It is recommended that a urinalysis should be performed for all penile trauma cases, and evaluation of urethral rupture should be performed in the presence of hematuria. 10 No published study has compared penile fracture patients with and without urethral rupture in terms of functional outcome and complications. Pariser et al. compared concomitant urethral rupture to penile fracture patients without urethral rupture but only in terms of possible risk factors. 9
The aim of the current study was to identify possible risk factors for urethral rupture concomitant with penile fracture and to evaluate the effect of urethral rupture repair on sexual and urinary functional outcomes and long-term penile complications.
Materials and methods
Data was collected on the basis of retrospective review of the medical records of 57 consecutive patients who underwent immediate surgical repair for penile fracture in a single tertiary referral center (Kocaeli University) between January 2003 and September 2020. Clinical and demographic data included age at the time of the fracture, education level, fracture etiology, symptoms, clinical findings, intraoperative findings including location of tunical tear and presence of urethral rupture, the time between fracture and surgery, hospital stay time, and post-hospitalization elapsed time to resumption of sexual activity. In addition, functional outcomes, such as appearance of erectile dysfunction and lower tract urinary symptoms, penile complications including penile curvature, presence of palpable nodule, painful erection, and paresthesia/numbness, and follow-up time between surgery and the most recent visit of the patient were collected from the patient charts. One patient who received preoperative oral phosphodiesterase type 5 inhibitor treatment, one patient who had multiple systemic diseases and reported preoperative ED, and two who did not have postoperative follow-up were excluded. The remaining 53 patients were included.
During the follow-up period, all patients completed the IIEF-5 and IPSS questionnaires. The patients’ erectile functional status was determined based on the results of the IIEF-5 questionnaire administered at the most recent follow-up visit. ED was defined as having an IIEF-5 score of <22. In follow-up, a Qmax less than 15 ml/s was considered suspicious of stenosis and in this circumstance urethroscopy was performed.
The study protocol was approved by the Local Ethics Committee (KU-GOKAEK 2021/313).
Surgical technique
In all patients, a subcoronal incision with circumcision was used to deglove the penile shaft and expose the tunica albuginea and spongiosa urethra, except in one patient when a penoscrotal incision was used for complete urethral rupture. The hematoma was evacuated, and the tunical defect was identified and repaired with interrupted absorbable sutures. An artificial erection with saline was performed after repair of the tunical defect to exclude the presence of other defects.
The corpus spongiosum was always inspected for possible concomitant traumatic injury to penile trauma before the defect in the tunica albuginea was repaired. Cystoscopy was performed in case of suspected urethral injury. If a urethral defect was identified, a simultaneous repair was performed. Partial urethral lesions were primarily closed with simple 3-0 or 4-0 absorbable sutures; the continuous suture technique was used in two cases, while in the remainder the interrupted suture technique was used. In cases of a complete urethral lesion, the urethral edges were dissected, trimmed, spatulated and closed with interrupted 3-0 or 5-0 polydioxanone sutures to ensure tension-free end-to-end anastomosis. A compressive dressing was always left in place.
Statistical analyses
All data were analyzed with Statistical Package for Social Science, version 21 (IBM Inc., Armonk, NY, USA). Descriptive statistics were used in the analysis of quantitative data. Kolmogorov-Smirnov test was used to test the normal distribution of continuous variables. Student’s t-test was used to compare means. Mann-Whitney U test was used to compare medians. Fisher’s Exact Test was used to compare two sets of categorical data. A p < 0.05 was considered significant.
Results
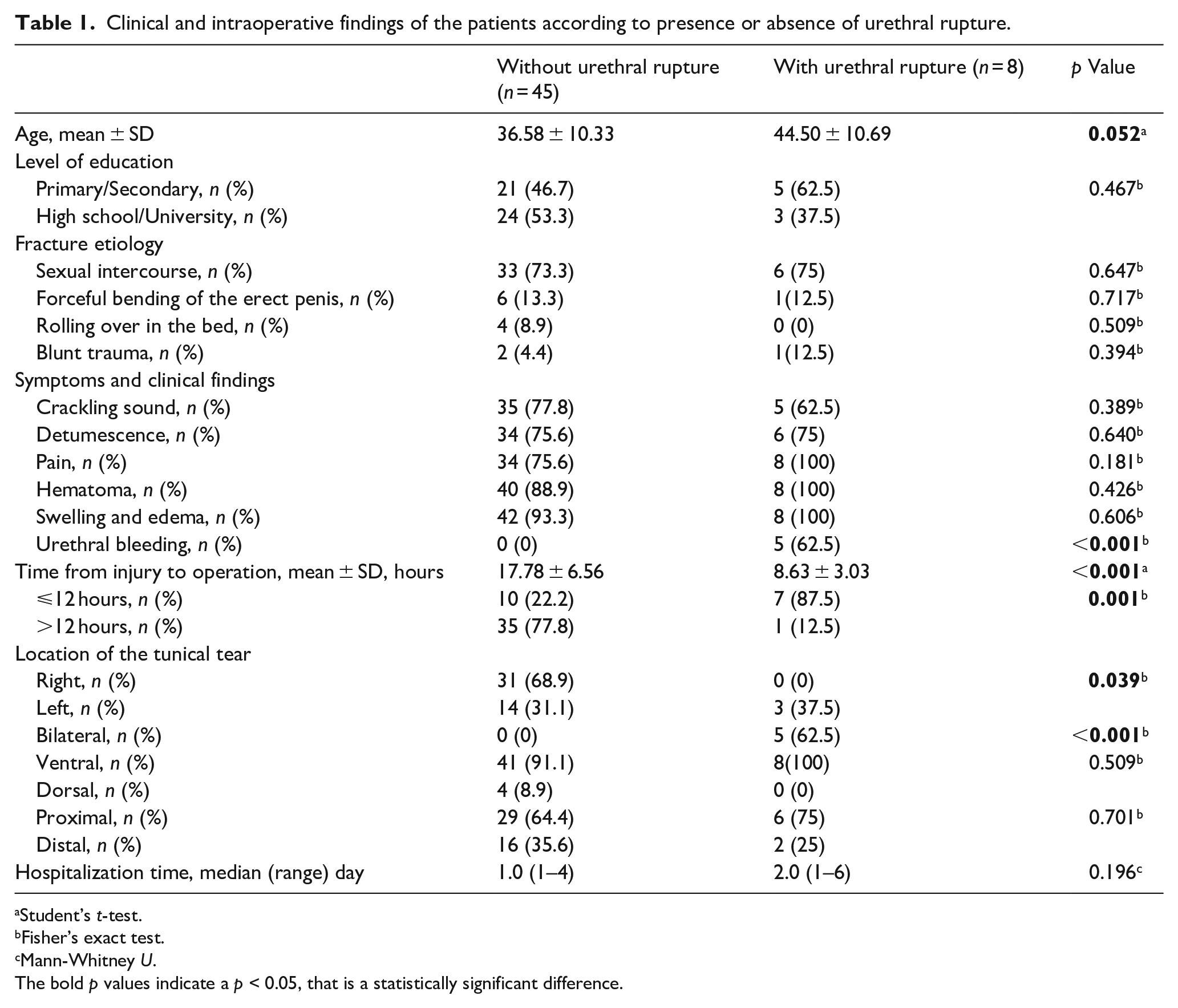
Fifty-three patients with penile fracture were included in the study. Of these, 8 (15.1%) required urethral rupture repair and the remainder (84.9%) did not. Clinical and intraoperative findings of the patients according to presence or absence of urethral rupture are given in Table 1. Before the fracture, all patients reported normal erectile function, and only two of them had risk factors for systemic vascular diseases, such as obesity (one patient) and hypertension (one patient). Moreover, none of the patients reported any drug use associated with managing lower urinary tract symptoms before the surgical repair.
Clinical and intraoperative findings of the patients according to presence or absence of urethral rupture.
Student’s t-test.
Fisher’s exact test.
Mann-Whitney U.
The bold p values indicate a p < 0.05, that is a statistically significant difference.
Patients with urethral rupture tended to be older, but this was at borderline significance (44.50 ± 10.69 vs 36.58 ± 10.33 years, p = 0.052). There was no significant difference in education levels or fracture etiology. Urethral bleeding was present only in patients with urethral rupture, as expected (62.5% vs 0%, p < 0.001). Except for this finding, the clinical presentation of patients with and without urethral rupture was similar in terms of the crackling sound, detumescence, pain, hematoma or swelling and edema. The time from injury until surgery was significantly shorter in patients with urethral rupture compared to those without urethral rupture (8.63 ± 3.03 vs 17.78 ± 6.56 h, p < 0.001) and the proportion undergoing operation ⩽12 h after injury was also significantly higher in patients with urethral rupture (p = 0.001). No urethral rupture patients had a tunical tear only on the right side of the penis and bilateral rupture was invariably present in patients with urethral rupture. Tears were ventral and proximal in both groups with similar rates (p = 0.51 and p = 0.70). Duration of hospital stay was longer in the urethral rupture group, but this was not significant (p = 0.2).
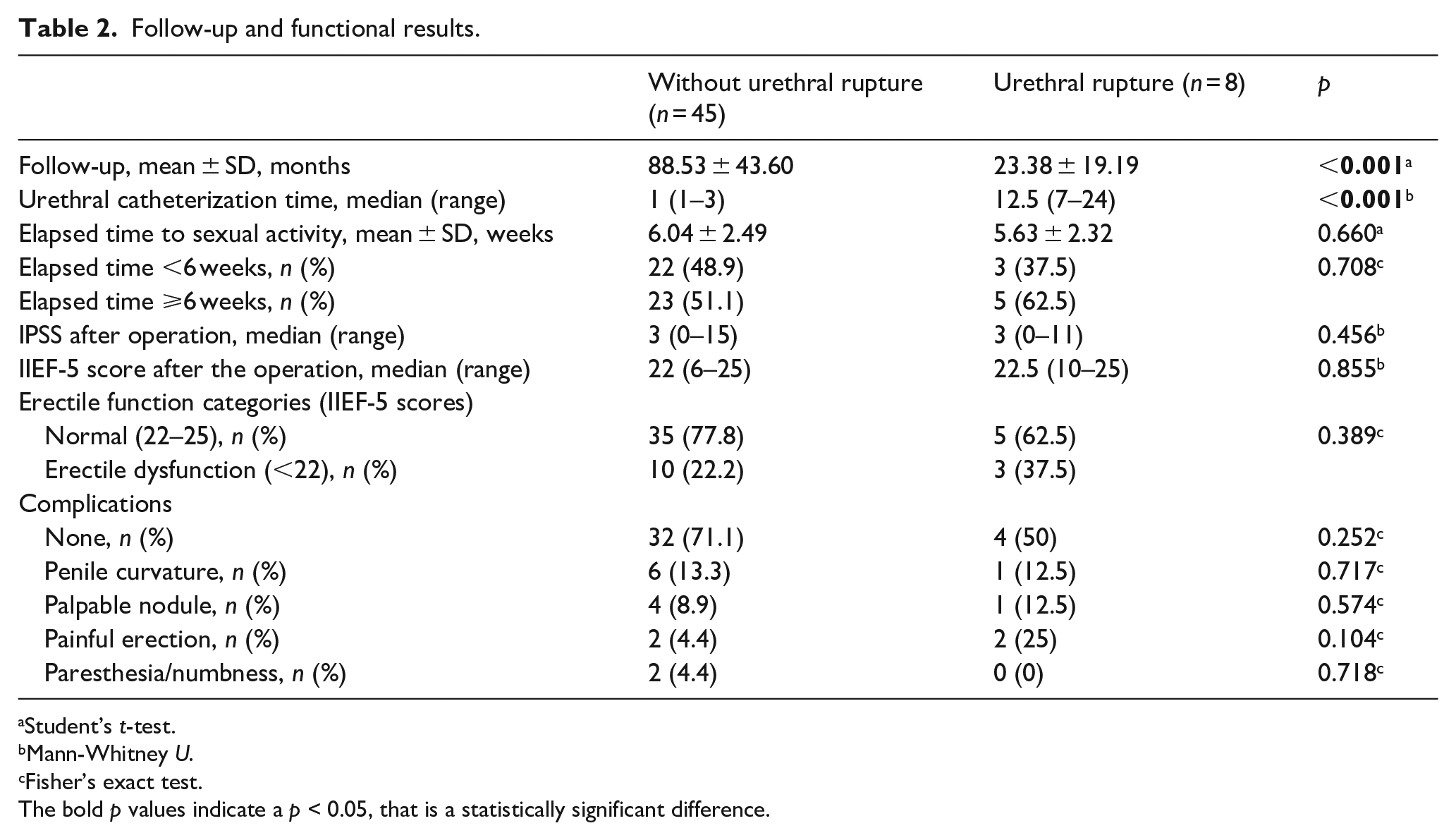
Mean follow-up time was around 2 years in the urethral rupture patients. However, this was significantly shorter than patients who did not have urethral rupture (p < 0.001). Elapsed time to resumption of sexual activity was similar in both groups (p = 0.66). There was no significant difference in IPSS and IIEF-5 scores, the presence of erectile dysfunction and complication rates (p = 0.47, p = 0.86, p = 0.39, and p = 0.25, respectively). The detailed results are presented in Table 2.
Follow-up and functional results.
Student’s t-test.
Mann-Whitney U.
Fisher’s exact test.
The bold p values indicate a p < 0.05, that is a statistically significant difference.
Age, etiology, lesion descriptions, and follow-up data of eight patients with urethral rupture are given in Table 3. Four patients had a complete urethral rupture with bilateral tunical tear and three of them were of sexual intercourse etiology. Two patients developed mild and one patient moderate erectile dysfunction. No urethral stenosis was detected.
Age, etiology, lesion descriptions, and follow-up data of eight patients with urethral rupture.
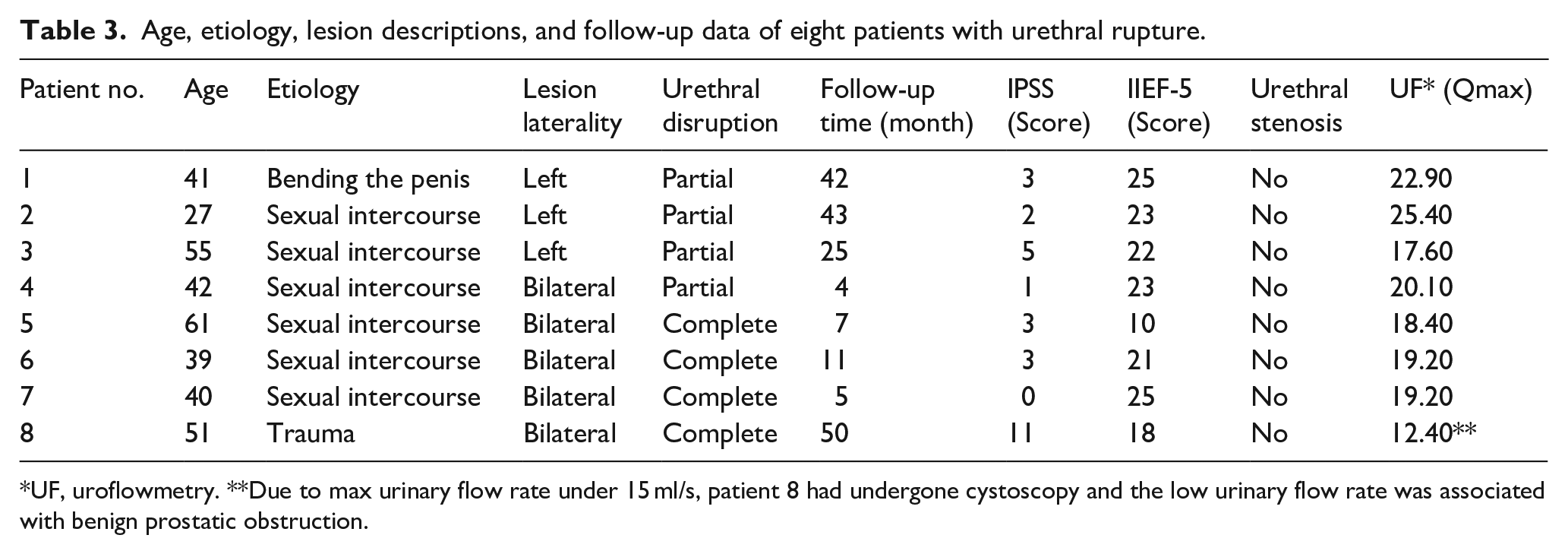
UF, uroflowmetry. **Due to max urinary flow rate under 15 ml/s, patient 8 had undergone cystoscopy and the low urinary flow rate was associated with benign prostatic obstruction.
Discussion
Concomitant urethral rupture is detected in approximately 15% of patients with penile fracture. Therefore, during penile fracture evaluation and treatment, the identification and repair, if necessary, of a concomitant urethral rupture are mandatory. Age, urethral bleeding, high- energy trauma, and bilateral involvement of corpus cavernosum are possible risk factors for concomitant urethral rupture.
Pariser et al. retrospectively evaluated 3883 penile fracture patients repaired surgically between 2003 and 2011 in the National Inpatient Sample database. 9 Their clinical data included age, race, comorbidity, insurance, hospital factors, timing of trauma (day of the week and season), hematuria, and preoperative urinary symptoms. They attempted to identify predictors of urethral evaluation and risk factors for urethral injury and found that older age conveyed a 1.84-fold increased risk of concomitant urethral rupture. 9 To our knowledge, there is no other study in the literature comparing penile fracture patients based on the presence or absence of urethral rupture. Thus, we believe the present study to be the first to compare perioperative findings, functional outcomes, and complications depending on the presence of concomitant urethral rupture. In the present study, urethral rupture patients also tended to be older (44.5 vs 36.5 years), but it is likely that the relatively small number of patients prevented this reaching significance.
Urethral bleeding is pathognomonic for the presence of concomitant urethral injury. Thus, concomitant urethral rupture should be evaluated in cases with microscopic or macroscopic hematuria. 10 In the literature, urethral bleeding or hematuria was found in the majority of patients who underwent urethral repair (Raheem et al. 100%, Derouiche et al. 100%, Kasarareni et al. 91.7%, Barros et al. 76.9%, el-Ibraheim et al. 92.8%).2,5 –8 Pariser et al. found that hematuria was associated with a 17-fold increased risk of urethral injury. 9 In our study, urethral bleeding was present only in patients with concomitant urethral rupture. However, lack of urethral bleeding does not necessarily exclude the presence of a urethral injury. Amer et al. showed that urethral bleeding was detected in 5.6% of cases, whereas confirmed urethral injury was present in 6.1% of patients in a meta-analysis of penile fracture. 12
Sexually-derived penile fractures are caused by higher energy trauma when compared to self-manipulation. The major etiologic factor is sexual intercourse in penile fracture patients with concomitant urethral rupture. In contrast, concomitant urethral rupture was reported infrequently in studies where the major etiologic cause was self-manipulation. Zargooshi reported 352 penile fracture cases. 4 The main etiologic cause was the taqaandan click, a penile fracture caused by forced bending of the penis for the abrupt termination of an erection during masturbation in 269 cases (76.4%). They found only five cases (1.4%) with concomitant urethral rupture. 4 Similarly, in the study of El Atat et al. self-manipulation constituted 60% (180/300) of the etiologic causes of penile fractures. 13 They found concomitant urethral rupture in only five cases (1.6%). 13 However, the rate of concomitant urethral rupture was 15%–24% in studies when the main etiologic cause was sexual intercourse.2,3,5 Penile fracture with bilateral corporal laceration also indicates high-energy trauma and there are only two case reports of bilateral corporal involvement without concomitant urethral rupture.14,15 Neither of these cases had an etiology of sexual intercourse with one caused by self- manipulation 14 and the other by blunt trauma. 15 Amit et al. reported eight concomitant urethral rupture cases with one bilateral involvement with complete urethral disruption. 3 Barros et al. reported nine bilateral involvements in their 13 concomitant urethral rupture cases, while four cases had complete urethral disruption. 2 Kasaraneni et al. reported one bilateral corporal involvement in 12 concomitant urethral rupture cases. 5 In our cohort, the etiology of injury was sexual intercourse in the majority of patients and the concomitant urethral rupture rate was 15.1%. Notably, in our study, all patients with bilateral damage (5/53) had urethral rupture.
We found that the delay between trauma and the operation was much shorter in patients with concomitant urethral rupture. Patients may be more concerned about urethral bleeding and this may accelerate admission to the emergency department. Delayed surgery is not recommended in the presence of concomitant urethral rupture.12,16
Follow-up time of penile fracture with concomitant urethral rupture was sufficiently long (about 2 years) to obtain reliable information about long-term effects. However, follow-up was significantly shorter than in patients without urethral rupture. This is surprising and the reason for this situation was that we encountered these patients more recently. It is interesting that we encountered more urethral rupture recently compared to previous years. There was no evidence of undiagnosed urethral rupture during penile fracture repair in the patient records of earlier cases, operation notes, or outpatient follow-up. There were no hospital admissions or any complications found which could be attributed to undiagnosed urethral rupture in any of our patients. We think the change in sexual behavior probably caused this situation due to increasing socio-economic developments in our developing country, especially in recent years.
For the first time we have reported long-term functional outcomes and complications of penile fracture, including comparison of functional outcomes and complications in patients with and without urethral rupture. There was no significant difference in terms of IPSS or IIEF-5 scores, presence of erectile dysfunction, presence of any complication, or presence of specific complications which included penile curvature, palpable nodule, painful erection, or paresthesia/numbness. Raheem et al. showed normal sexual activity with complete recovery of erectile function in 11 of 12 concomitant urethral rupture patients with complete urethral disruption. 8 Amit et al. reported that all patients were able to void with a good urine flow and had an erection with adequate rigidity, although one patient complained of painful erection and two patients complained of penile curvature in their eight concomitant urethral rupture patients. 3 Derouiche et al. did not find any erectile dysfunction, penile curvature, or painful erection in their 10 patients. 6 Kasaraneni et al. reported that all patients voided well, and none had erectile dysfunction, while one patient had penile curvature in their 12 concomitant urethral rupture patients. 5
This study had some important limitations, including its retrospective design and the relatively small number of patients with concomitant urethral rupture.
Conclusions
Older age is a possible risk factor for concomitant urethral rupture in patients with penile fracture. Concomitant urethral rupture was detected in all patients with urethral bleeding and bilateral corpus cavernosum involvement. The presence of urethral rupture was associated with shorter delay from trauma to surgery. Concomitant urethral rupture repair did not adversely affect long-term sexual and urinary functional outcomes and did not increase penile complication rates.
Footnotes
Acknowledgements
The authors are grateful to Mr. Jeremy Jones of the Academic Writing Department of Kocaeli University, Izmit, Turkey, for his assistance in editing the English used and for his help and advice concerning the contents of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.