
Abstract
Objective:
To assess a novel combined laser suction handpiece (LSH) for performing PCNL in a clinical setting.
Methods:
The study comprised 40 consecutive PCNLs performed between May 2019 and February 2020. The first 20 procedures (Group A) were performed with conventional ultrasonic or pneumatic devices and the other 20 (Group B) were performed with the use of the new LSH. All patients were treated by tubeless supine PCNL. The groups were compared for demographics, clinical data, operative time, lithotrite effectiveness, stone clearance rate (SCR), and outcome.
Results:
Groups A and B were similar in age, and in stone size, complexity, and density (Hounsfield units) (p < 0.05). The average operative time was 99 and 78 min, SCR 143 and 200 mm3/min, hospital stay 1.6 and 1.1 days, and stone-free rate 90% and 95%, respectively. Despite a trend toward better results with the new LSH, none of these comparisons reached statistical significance. Ineffective lithotripsy with the initial device (ultrasonic) requiring conversion to another modality (ballistic) occurred in six (30%) procedures in Group A, while all procedures were effectively accomplished with the LSH in Group B (p = 0.02). There were two complications in Group A and none in Group B (p > 0.05).
Conclusions:
The LSH is as effective and safe as the traditional lithotrites for performing PCNLs. This new tool completes the capabilities of the holmium laser high-power machines, enabling them to serve as the sole platform for all endourological treatments.
Introduction
Despite its proven effectiveness developed along 44 years of implementation in the treatment of large and complex renal stones, percutaneous nephrolithotomy (PCNL) is still undergoing modeling and evolvement. 1 Endourologists continue to seek optimization of indications, position, access, tract size, instruments and ancillary devices, hospital stay, postoperative drainage, imaging, and follow-up. 2 Lithotrite modalities are also continuously transforming and undergoing technological changes, including hybridization and refinement of existing tools, as well as the introduction of new innovations. 3 In comparison to other lithotrites, the holmium laser is a multipurpose source of energy that can be used for the treatment of urinary stones, strictures, urothelial carcinoma, and prostatic enlargements. It has the unique ability of being delivered through flexible tiny fibers that fit both flexible and rigid scopes regardless of their size. Although the holmium laser’s utility has been described in mini-PCNLs, in which the working channel diameter restricts the use of other fragmentation devices, its uses with standard rigid nephroscopes (e.g. 18–26 FR) is not well-defined.4,5 As such, endourology units must be equipped with both ultrasonic and ballistic devices for PCNL in addition to the holmium laser for carrying out other endoscopic approaches. A novel laser suction handpiece (LSH) (Lumenis Ltd., Yokneam, Israel) was designed under the rationale that the endourological needs might be reduced to a single multipurpose source of energy. Its first application in the clinical setting was described 2 years ago in a case report by Ghani et al. 6 We recently adopted this tool in our own practice, and this study reports the results of the introduction of the LSH in routine performance of PCNLs and compares its effectiveness with other lithotrites.
Methods
The study was approved by the Institutional Review Board and the participating patients signed informed consent forms (TLV0233-20). It describes 40 consecutive PCNLs performed between May 2019 and February 2020. The data were retrospectively collected. The first 20 PCNLs (Group A) were performed primarily with a conventional ultrasonic lithotriptor (Olympus LUS-2) backed up by a ballistic (Swiss LithoClast®) device when needed. The other 20 PCNLs (Group B) were performed with the new LSH that had been introduced in our standard practice in October 2019. The two groups were compared for demographics, stone size and complexity, operating time, stone clearance rate [SCR, defined as stone volume divided by operating time (mm3/min)], conversion to another lithotrite modality, stone-free rate, hospital stay, complication rate, and stone-free status. All procedures were performed through a 24 Fr working sheath and by means of a rigid 21/18 FR nephroscope, concluding in a tubeless fashion, with the patient under general anesthesia and in a supine position. Flexible nephroscopy and nephrography were performed at the end of the procedure to ensure stone-free status. Further details about our PCNL technique are described elsewhere. 7
The LSH is composed of an 11.3 Fr external sheath attached to a handpiece with two buttons. One button activates the suction and can be set in permanent or manually activated modes. The other button serves to move the laser fiber in and out (Figure 1). In our current study, the LSH was connected by a tube to a built-in filter and an aspirating pump located on the Pulse™ Moses 120H holmium laser machine (Lumenis Ltd., Yokneam, Israel) (Figure 2). This connection offers the possibility of synchronizing the lasering with suction by pressing the activation pedal. The energy setting was 0.3 J/80 Hz for dusting and 0.8–1 J/20–30 Hz for fragmentation.
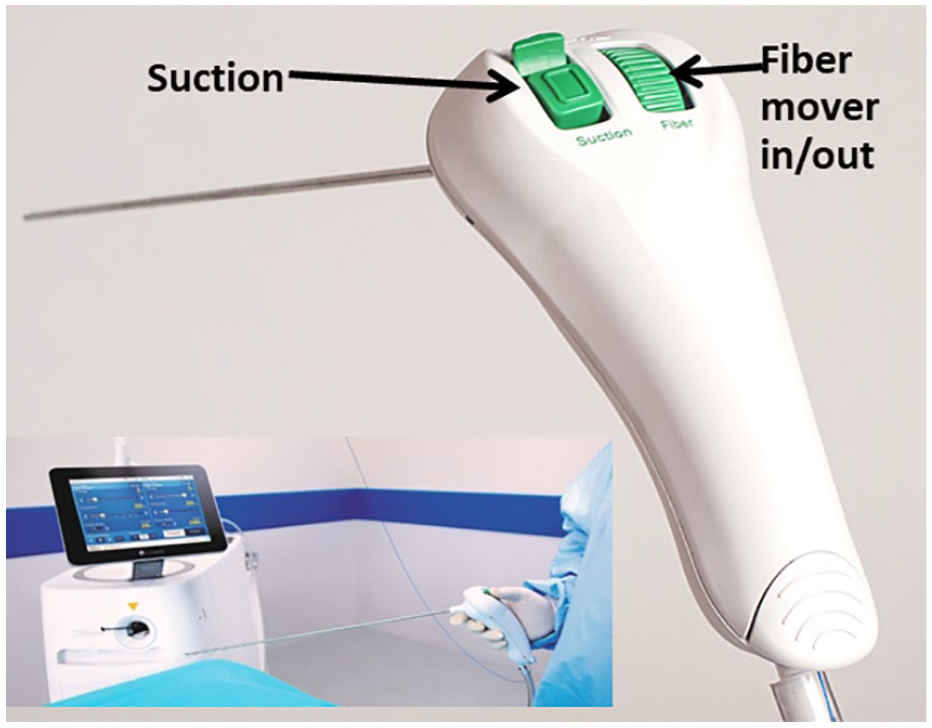
The Lumenis laser suction handpiece composed of a 11.3 Fr external sheath and a handle with two buttons activated by the surgeon’s thumb.
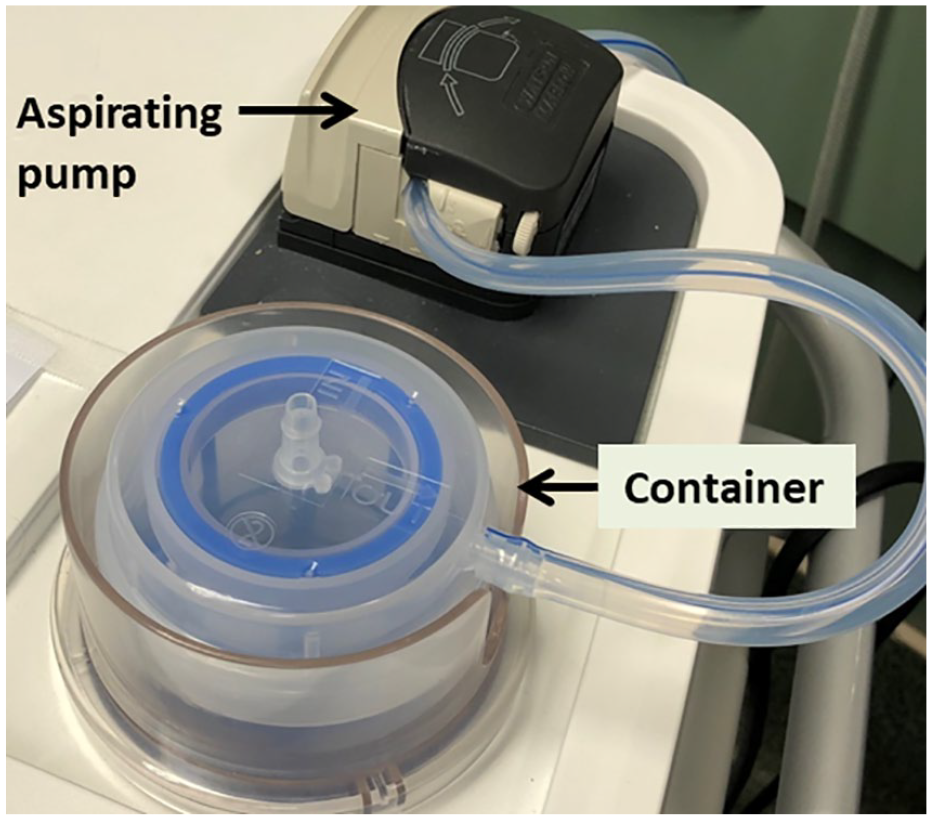
The built-in Lumenis filter and aspirating pump device of the Pulse® Moses 120H holmium laser machine.
Student’s t-test or the Mann-Whitney U test were employed for distribution depending upon normality. Levene’s test was applied for equality of variances, and the t-test for equality of means. Significance was considered at p < 0.05. The data were processed by SPSS (IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp.).
Results
The demographics and stone size, complexity, and density were similar for both study groups (p > 0.05) (Table 1). The overall average density of stones exceeded 1,100 Hounsfield units (HU), indicative of their hardness. There were no significant differences between the groups in terms of operating time, SCR, hospital stay, and complication rate (Table 2). Group A was characterized by inefficient ultrasonic lithotripsy in six (30%) cases, necessitating completion of the procedure with conversion to ballistic fragmentation and removal of fragments by either a vacuum cleaning effect or stone graspers and baskets. All cases in group B were successfully completed with the LSH as the sole lithotrite device.
Comparison of demographics and stone characteristics.
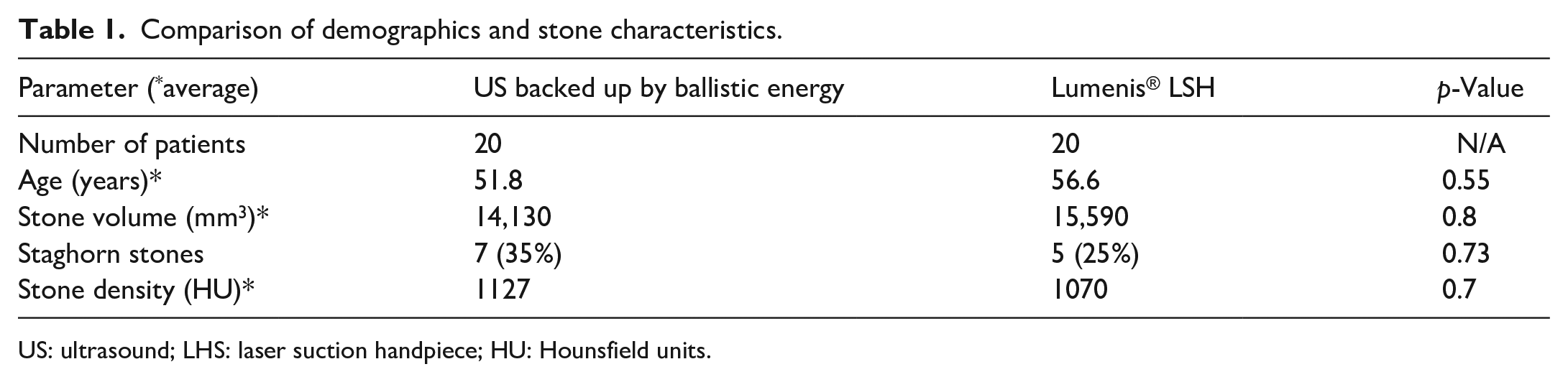
US: ultrasound; LHS: laser suction handpiece; HU: Hounsfield units.
Outcome of conventional lithotripsy compared to the use of the laser suction handpiece.
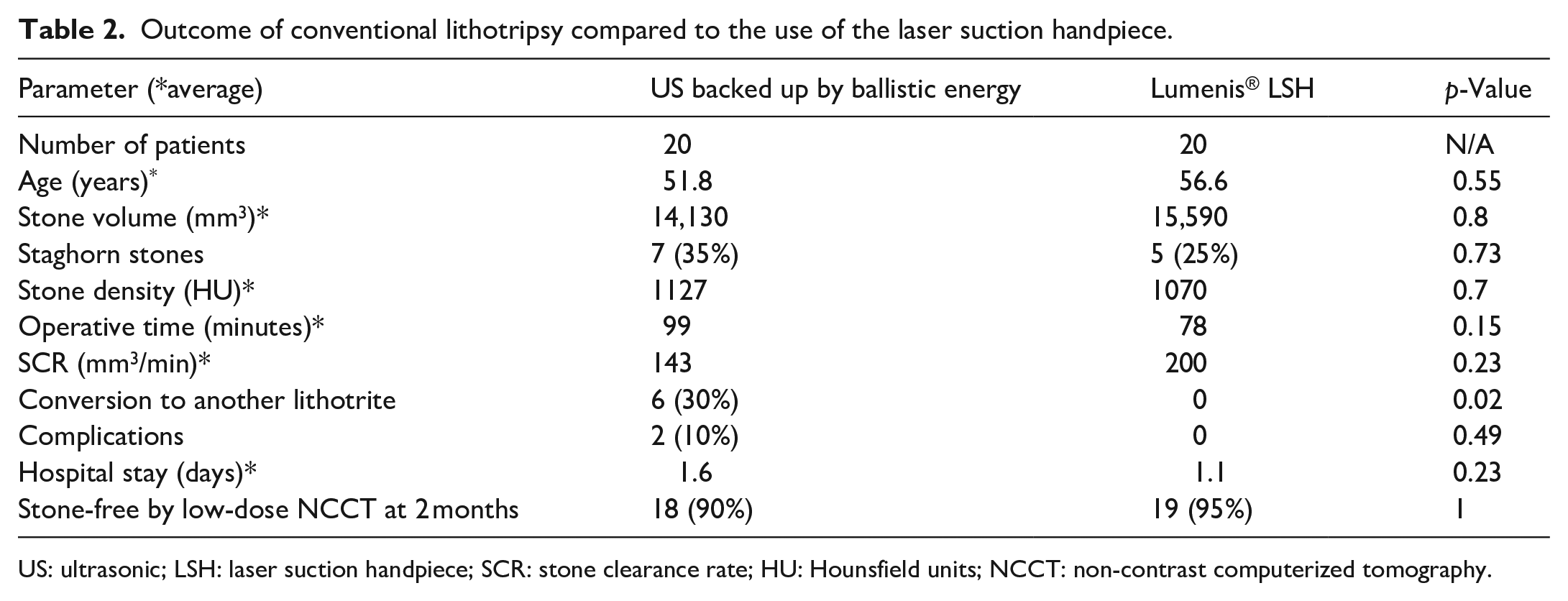
US: ultrasonic; LSH: laser suction handpiece; SCR: stone clearance rate; HU: Hounsfield units; NCCT: non-contrast computerized tomography.
There were two complications in Group A, both infectious, contributing to a relative but non-significant prolongation of hospital stay. The stone-free rate was assessed by low-dose non-contrast computerized tomography 2 months after the procedure, and it was 90% (18/20) for Group A and 95% (19/20) for Groups B (p > 0.05). One patient in each group had residual stones re-treated with flexible ureteroscopy, and one patient in group B with a 4 mm residual fragment was left for observation.
All of the operations were performed by the fellow in endourology and the endourology residents under the supervision of a senior endourologist. The impression of the surgeons and the supervisor was that the device was easily adapted and posed no remarkable difficulties.
Discussion
The present generation of endourologists is witnessing a progressive evolution toward the predominance of endoscopic approaches. 8 This shift is characterized by increasing rates of ureteroscopies on the account of shock wave lithotripsy (SWL), while the rate of PCNL remains constant. This stability of PCNL probably derives from its indications related to large size, high complexity, hard stone composition, and stones unsuccessfully treated by either ureteroscopy or SWL. As a result of these trends, the endourology setting is marked not only by miniaturization and improvement of visualization, but also by innovative developments in intracorporeal lithotripsy devices. 3 Hybridization of existing modalities has provided a substantial contribution to their effectiveness. One of the most significant achievements was the combination of ultrasonic and ballistic devices that offered a synergic effect of the superior ability of the ballistic component of fragmentation with the ability of the ultrasonic modality to simultaneously dust and evacuate small fragments (e.g. Swiss LithoClast® Ultra).9,10 This was followed by combining a dual ultrasonic probe that provided two different ultrasonic pulse rates and intermittent mechanical impacts on the stone, while aspirating the fragments through the inner hollow of the probe (e.g. Cyberwand—Olympus). Beside these devices, holmium laser machines became an indispensable tool that was used mainly for ureteroscopic and mini-PCNL procedures, as well as for treating symptomatic prostatic enlargement, strictures, and upper tract urothelial cancer.4,11–14
Standard PCNL for the treatment of large and infected stones is still being carried out through 18–26 FR nephroscopes with 4–4.5 mm working channels, with the intention not only to dust or fragment the stones but also to actively remove the residual material. These needs cannot be accomplished with a laser fiber, even if it is wide (500–1000 nm) and used in combination with a stabilizing catheter to reduce fiber trepidations related to the pulsed photo-acoustic mechanism of the holmium laser. It appears that a well-equipped, high-volume endourological center needs at least two energy sources, one ultrasonic and/or ballistic, and the other laser to cover the entire spectrum of treatments. However, adaption of the laser platform might suffice to accommodate all endourological treatments.
Cuellar and Averch 15 were the first to explore a device similar to an ultrasonic lithotrite with a 365-nm laser fiber that passed through the hollow of the probe and connected to manually controlled suction. They reported feasibility and effectiveness in 29 patients by using a fragmentation setting at an average of 1.3 J/11 Hz. This artisanal tool did not gain popularity, but three manufacturers developed refined products based on its principles. LithAssist (Cook Medical) was the first commercially available device with an ergonomic design to allow easy combination of laser and suction during standard PCNL. 16 This 11.6 FR probe with an activating handle was compared in vitro in a model using artificial soft and hard stones to the Swiss Lithoclast Ultra (Boston Scientific). The LithAssist performed better with hard stones but it was outdone by Lithoclast in soft stones. Karl Storz later released the LASER Suction Tube®, which was a simple reusable metallic tube with a side connection to negative pressure, and Lumenis® presented the LSH as a single-use 11.3 Fr device. All three were compared in an animal model that revealed similar capabilities in stone framentation. 17 The first clinical application in humans was recently demonstrated by Ghani et al. 6 in a video case report of a PCNL performed for a struvite 1000 HU staghorn stone successfully treated in a dust setting in a procedure that took 110 min.
Our study took this one step forward by applying this technology in routine clinical practice. The LSH performed as well as the ultrasonic and ballistic lithotrites, without the need to be backed up by another source of energy and with a trend toward shorter operating time and better effectiveness, although not reaching a level of significance. It is possible that the failure encountered with the LUS 2 machine is attributable to its being an older ultrasonic device and that the new generation of ultrasonic lithotrites, such as ShockPulse-SE (Olympus) or Swiss LithoClast® Trilogy lithotripter, would have succeeded. In any event, the LSH extended the horizons by supporting the concept that the holmium laser may serve as the single energy source for all endourological applications. In our opinion, the combination of the LSH with the built-in aspiration and collecting device on the Pulse™ Moses 120H holmium laser machine that is automatically synchronized with the activation of the laser in high-power modes makes it an ideal system for dusting, fragmentation, and aspiration of residual stones. Our study restrained to assessment of clinical implementation. The cost effectiveness implications of using this system remain to be analyzed in further comparison studies.
We are aware of the inevitable limitations related to the retrospective design of this study, the small comparison groups, and the lack of another comparison group of patients treated with a combined ballistic and ultrasonic machines. However, we believe that the similarity among the two study groups in terms of by-entry clinical data as well as the highly satisfactory performance of the LSH alone provide enough support for this study to stand-alone and to confirm its utility in clinical use.
Conclusion
The Lumenis® LSH is as effective and safe as the traditional lithotrites for performing PCNL. It can be used at high-power settings and in various modes, including the MOSES technology, in order to avoid retropulsion. This new tool completes the capabilities of the holmium laser high-power machines, thereby enabling it to serve as the sole source of energy for all endourological approaches.
Footnotes
Author contribution
Noam Bar-Yaakov: Acquisition of data, drafting manuscript, assisting surgery. Haim Hertzberg: IRB application, acquisition of data, statistics. Ron Marom: Assisting surgery, patient follow-up, instrumental coordination. Jemal Jikia: Surgery, data interpretation, drafting manuscript. Avi Beri: Critical revision of manuscript. Roy Mano: Critical revision of study design. Ofer Yossepowitch: Supervision. Mario Sofer: Study design, surgery, data interpretation, team coordinator, editing, and revision.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Institutional Review Board (IRB) (Tel Aviv Sourasky Medical Center, Tel Aviv, Israel, TLV0233-20) approval was obtained for this study. Written patient informed consent was obtained before undergoing the procedures.