
Abstract
Background:
Patients receiving left ventricular assist device (LVAD) implantation can experience significant psychological stress that negatively impacts quality of life and treatment outcomes. Assessment of LVAD stress is critical for providing targeted interventions and advancing the relevant literature. The goal of this study was to establish a new measure of LVAD-specific patient stress, the LVAD Stress Questionnaire (LSQ).
Methods:
The LSQ is an 18-item measure developed by researchers with extensive clinical experience providing psychological assessment and care for LVAD candidates and recipients. In this study, the LSQ was evaluated with a sample of 73 participants post-LVAD implant.
Results:
Results of factor analysis supported the use of an LSQ full-scale score, also yielding five subscales of distinct areas of stress. Cronbach’s alpha indicated that the full scale and subscales had reasonable to good internal consistency. The LSQ full scale score and four of the subscale scores were positively associated with depression and anxiety. Younger age, female gender, and being unpartnered were associated with higher LVAD stress based on one or more subscale scores.
Conclusions:
The LSQ is a useful tool that treatment teams can utilize to ascertain whether and in which area an LVAD causes stress, thereby informing interventions to maximize patient outcomes.
Introduction
Left ventricular assist devices (LVAD) are mechanical circulatory devices commonly indicated for management of advanced heart failure. They are employed either as a destination therapy or as a bridge to heart transplant. 1 Although they are lifesaving devices, patients may experience significant psychological distress associated with LVAD implantation. 2 The psychological impact of LVAD is a strong determinant of patients’ quality of life and treatment outcomes after LVAD implantation.3,4
Research suggests that an increase in stress is most common during the immediate post-implant phase with symptoms persisting up to 25 months post-implant. 5 Approximately 25% of LVAD patients experience chronic stress after hospital discharge. 6 Within the first year of Intensive Care Unit (ICU) admission, one in five patients post-LVAD implantation develop clinically significant post-traumatic stress disorder (PTSD), a stress and fear disorder that can emerge after experiencing or witnessing traumatic events. 4 Nevertheless, an increase in psychological distress can occur at any point during the LVAD implantation process, though the reasons for stress may vary at different phases. For many patients, stress related to the LVAD begins in the educational and preoperative phases. Prior to implantation, patients may report stress related to uncertainty of treatment outcomes. 7 During and after implantation, patients may report stress related to a range of concerns, including fears of complications and device malfunctions, disease progression, cardiac rehabilitation, maintaining medication adherence, and managing the driveline and device.2,3 Specifically, the exterior components of LVAD (e.g., driveline and batteries) provide constant awareness of the device, 3 which likely increases stress.
Device and patient specific factors can influence the stress associated with LVAD. Patients with earlier iterations of LVAD, specifically pulsatile devices, tend to feel agitated by the clicking noise stemming from the device and have higher rates of complications. 3 The experience of living with LVAD may differ by age, gender, and partner status. Younger age is associated with greater pain/discomfort and higher levels of anxiety and depression. 8 Older age is believed to be associated with an increased risk for cognitive difficulties 1 and mobility issues 8 post-implantation. This may also lead to increased stress, as poorer cognitive function can disrupt patients’ ability to comprehend and comply with their post-LVAD care 9 and reduce their functional capacities through negatively impacting sleep quality. 4 Regarding gender, women experience more psychological distress (i.e. anxiety and depression) and functional impairment post-LVAD implant relative to men. 8 Moreover, patients who are unpartnered may be at an increased risk of loneliness and therefore experience greater stress and depression. 10
In addition, the lifestyle interference brought by LVAD 1 may increase or maintain patients’ stress in daily life. Social isolation plays a prominent role in patients’ experience of anxiety and depression post-implant. 5 Because many live a more withdrawn and cautious life after the installation of the device, it may be difficult for them to continue engaging in activities that used to bring them joy or find new pleasurable activities. Furthermore, research has shown that LVAD may reduce satisfaction of sexual intimacy among patients and their partners. 1 Potential disturbances during sexual intimacy, including the functional impairments resulted from LVAD driveline or battery pockets as well as body image concerns, can lead to emotional distancing between patients and their partners.11,12
Taken together, LVAD-related stress has been found to be associated with a variety of patient concerns throughout the implantation process, patient demographic factors, and life-interference in day-to-day living. To inform opportunities for improving patients’ psychological wellbeing thereby enhancing treatment outcomes, it is essential to assess the intensity of and reasons for LVAD-related stress. However, relevant measures are extremely limited. To our knowledge, there is one measure of LVAD specific stress, the LVAD Stressor Scale. 13 This scale was developed based on data collected using a preoperative version of the Heart Transplant Stressor Scale. 13 From items of transplant-related factors, rated on a scale of ‘not all stressful (0)’ to ‘very stressful (3),’ the research team consolidated six stressors: physical, family, work/financial, hospital, psychological, and self -care. 13 To the best of our knowledge, LVAD Stressor Scale has not been widely disseminated; it has only been utilized in seven research studies since its development in 1994, with the most recent use occurring in 2011. 14 Given that it was directly adapted from a measure of heart transplant stressors, instead of LVAD specific stressors (e.g., driveline maintenance), the LVAD Stressor Scale has limited functional precision.
Accordingly, the purpose of this study was to develop a new, brief, patient-reported measure of LVAD stress—the LVAD Stress Questionnaire (LSQ) and to evaluate this measure with a sample of LVAD recipients. Clinically, this measure may inform more targeted assessments of patients’ readiness for receiving a LVAD and their adjustment to it. The development of this measure will allow future empirical studies to advance understanding of the stress specific to LVAD and its impacts on quality of life and health outcomes, and to maximize treatment interventions.
Methods
Patients who received LVAD implantation were recruited during appointments at a large academic medical center between May 2014 and July 2024. Patients were provided with information on the study and the opportunity to consent to or decline participation. Once informed consent was obtained, patients completed questionnaires eliciting demographic and health information. Of key interest for this study, patients completed the LSQ. Patients also completed measures of general psychological distress, including Generalized Anxiety Disorder-7 (GAD-7) and Center for Epidemiology Studies Depression Scale (CESD). This study was approved by the university institutional review board.
A total of 73 participants post-LVAD implant consented to participation and completed the study. Based on the demographic questionnaire, the sample was predominantly male (79% male, n = 58), with a mean age of 62 years (SD = 12.8, min = 20 years, max = 83 years). Participants were mostly White (64%, n = 47) or Black (30%, n = 22). Most participants were partnered/married (64% n = 47); 9 (12%) were single, 3 (4%) were separated, 8 (11%) were divorced, and 5 (7%) were widowed. Participants were 4 to 489 weeks post-LVAD implant (M = 114, SD = 103.1) at the time they completed study measures. Among the sample, 58 (79%) of patients received LVAD as destination therapy and 15 (21%) received LVAD as bridge to transplant.
LVAD Stress Questionnaire
The LSQ is an 18-item questionnaire assessing LVAD-specific stressors and concerns. This measure was developed by a group of researchers with extensive clinical experience providing psychological assessment and care for LVAD candidates and recipients, including the senior author (EB) who has worked in this field for over 30 years. Two of the co-authors (EB and DE) developed an initial list of 18 LVAD stressors based on clinical experience. This list was subsequently reviewed and determined as relevant and comprehensive by an experienced LVAD nurse coordinator (AB) at the medical center, supporting the content validity of the LSQ. In the LSQ, the 18 items cover a variety of aspects of living with LVAD (e.g. changing the battery, alarms, keeping equipment clean, body image concerns, and showering). They are rated on a 5-point Likert Scale (1 = “Not at all Stressful,” 2 = “A little Stressful,” 3 = “Moderately Stressful,” 4 = “Very Stressful,” and 5 = “Extremely Stressful”).
Statistical analyses
Kaiser-Meyer-Olkin Measure (KMO) of Sampling Adequacy and Bartlett’s Test of Sphericity were employed to determine appropriateness of factor analysis. After establishing appropriateness, a Principal Components Analysis (PCA) was conducted to identify the underlying factor structure of 18 items and to assess the utility of the measure as a full scale. Specifically, to establish distinct components of the scale, the initial analysis specified extraction of components with an Eigenvalue of 1. A varimax rotation was used to simplify the identified components, minimizing the variance within component while identifying the specific variance of each component. Individual items were organized into subscales based on the identified components. A secondary PCA was run, specifying extraction of only one factor, to determine the appropriateness of using a full-scale score. Additionally, Cronbach’s alpha was used to examine the internal consistency of the full-scale measure as well as the identified subscales.
In an exploratory manner, independent samples t-tests were used to compare LSQ scores between different demographic groups. Correlational analyses were conducted to describe the relationships between LSQ scores and age and general distress (i.e., anxiety and depression).
Results
Factor structure and internal consistency
The KMO of Sampling Adequacy was .781, indicating that the strength of the relationships among LSQ items was high enough to suggest an underlying factor structure. Bartlett’s Test of Sphericity was also significant (χ2 (153) = 638.795, p < .001), indicating appropriateness for factor analysis. Results of the PCA with varimax rotation yielded five components: (1) driveline, (2) controller and battery, (3) fears related to the device, (4) lifestyle interference, and (5) maintenance of device. The dimensionality of the scale further supported the content validity of the scale. According to Cronbach’s alphas, all subscales based on the identified components showed reasonable to good internal consistency. See Table 1 for the five identified subscales and their Cronbach’s alphas, as well as rotated factor loadings of individual items on corresponding subscales and the full scale.
LSQ factor loadings and internal consistency.
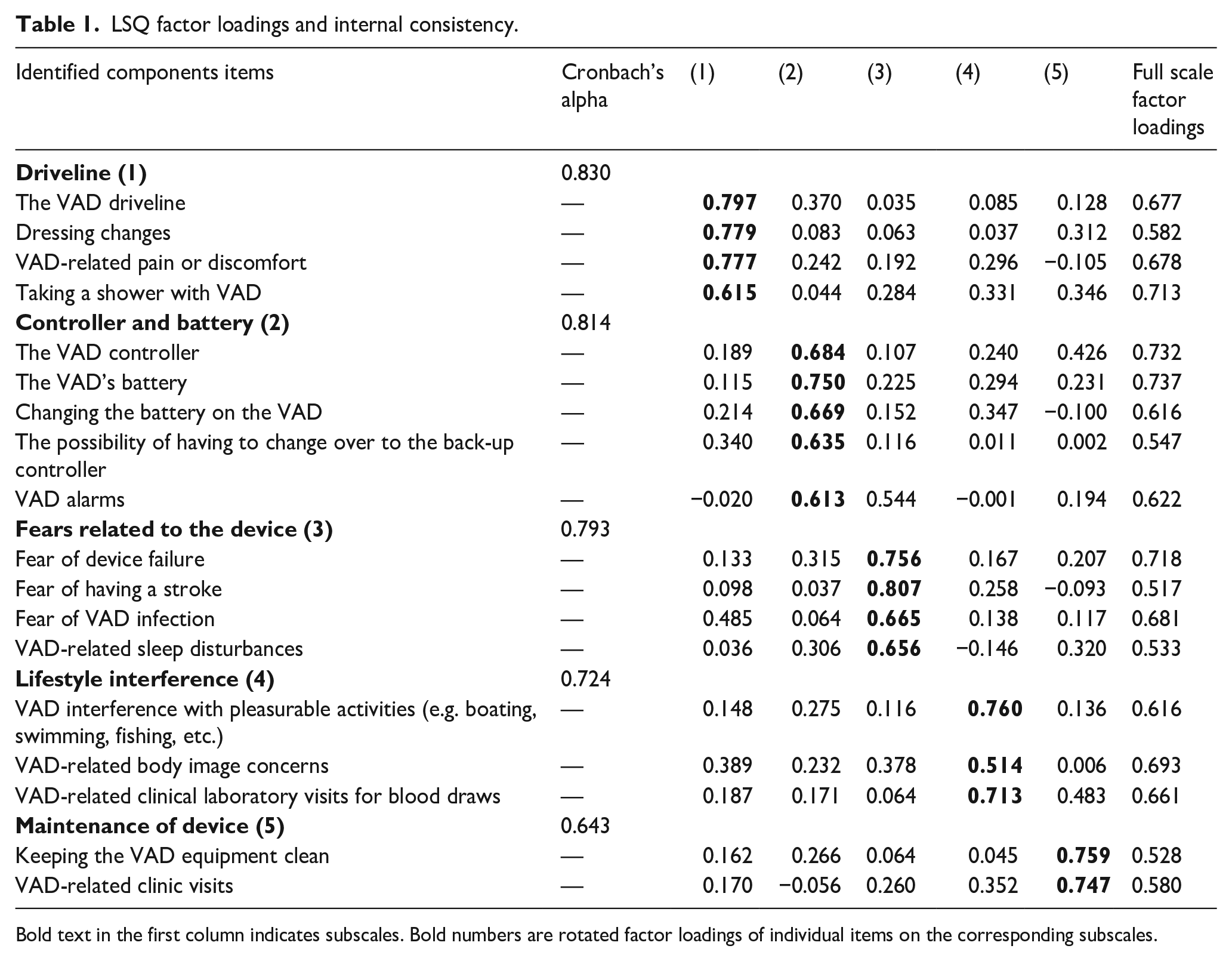
Bold text in the first column indicates subscales. Bold numbers are rotated factor loadings of individual items on the corresponding subscales.
LSQ and other variables
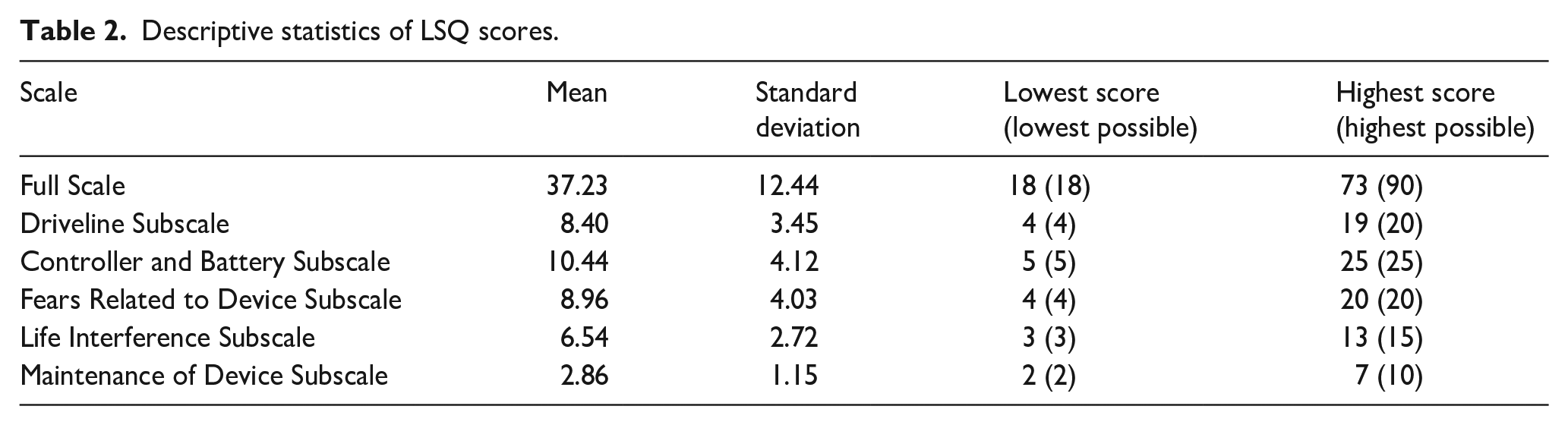
Descriptive statistics of full-scale and subscale scores of the LSQ are presented in Table 2. According to independent samples t-tests (see Table 3), women and unpartnered participants reported significantly higher scores on the Fears Related Device subscale. Furthermore, correlational analyses (see Table 4) indicated that younger participants reported higher full-scale scores and higher scores on the Driveline, Fears Related to Device, and Life Interference subscales. Moreover, both higher generalized anxiety and depression scores were associated with higher full-scale scores as well as higher Driveline, Controller and Battery, Fears Related to Device, and Life Interference subscale scores.
Descriptive statistics of LSQ scores.
LSQ scores by gender and partner status.
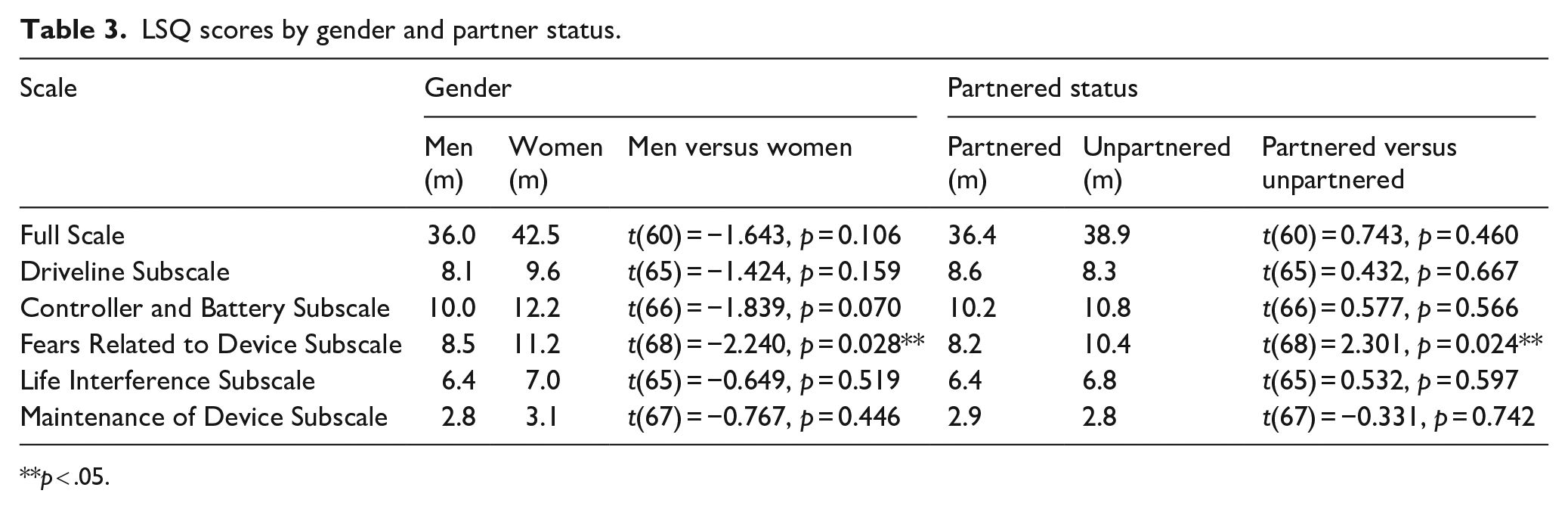
**p < .05.
Correlations between LSQ scores and age, anxiety, and depression.
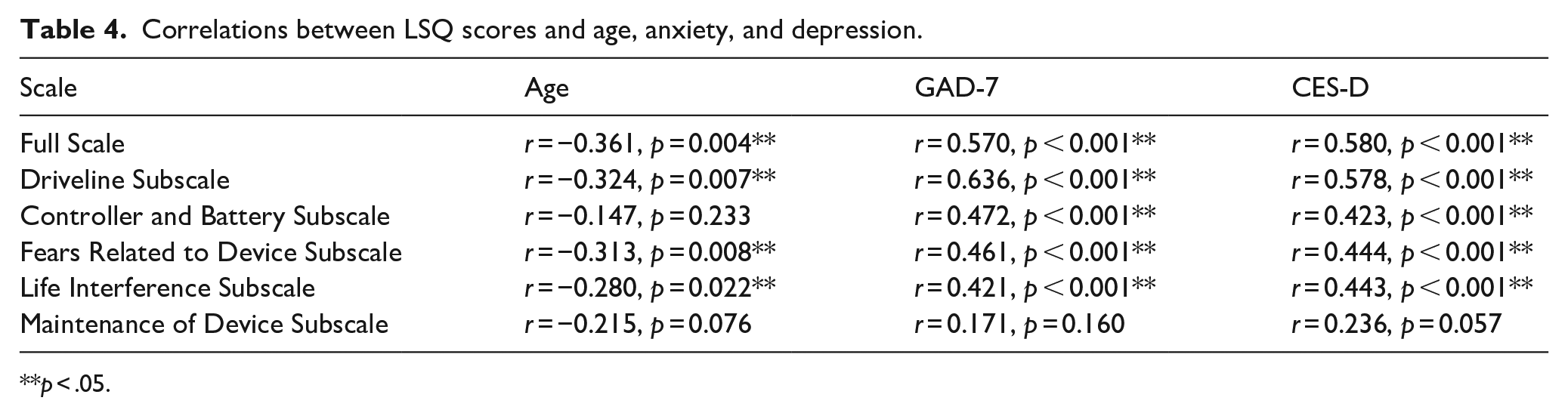
**p < .05.
Discussion
In the current study, a new, patient-reported measure of LVAD stress—the LSQ was developed by a group of content experts. LSQ provides one summary score as well as five subscale scores of stress in the areas of (1) driveline, (2) controller and battery, (3) fears related to the device, (4) lifestyle interference, and (5) maintenance of device. Adequate internal consistency was found for the full-scale and subscales of LSQ. Based on LSQ scores collected from the current sample, higher scores of LSQ full-scale and four of the five subscales (stress in all areas except for maintenance of device) were positively associated with higher ratings of depression and anxiety. Furthermore, higher scores of LSQ full-scale score and three of the five subscales (stress related to driveline, fears related to device, and life interference) were associated with younger age. It was also found that being female and being unpartnered were associated with greater stress specifically related to LVAD device.
Clinical implications
Learning to manage and live with an LVAD can be extraordinarily stressful for some recipients. Greater psychological distress related to LVAD has been found to be associated with less optimal outcomes. 6 The LSQ provides an assessment of LVAD stress in five different domains. Asking LVAD recipients to complete the LSQ may help LVAD treatment team members identify which recipients are stressed. It can also provide an indication of how stressed LVAD recipients are and delineate which area(s) they are stressed about. Treatment teams can then provide additional education targeting those specific areas or refer patients to psychotherapy to address LVAD stress. Additionally, the LSQ can be re-administered to evaluate the effectiveness of educational and psychological interventions in decreasing LVAD-related stress.
Limitations and future directions
The main limitation of the present study is the small sample, which may have limited the generalizability of study findings. Future research should replicate psychometric analysis of LSQ in large-scale studies. In order to better understand the role of LVAD specific stress in patient health, future research may benefit from assessing patients’ perception of stress and the impact of stress on specific outcomes, such as treatment adherence, healthcare utilization, and survival.
Summary
Measuring the level of psychological stress associated with an LVAD is critical to success post-LVAD. The LSQ is a useful tool the LVAD treatment team can utilize to ascertain whether and how LVAD causes stress/distress among patients and to identify opportunities for intervention to maximize patient outcomes.
Footnotes
Data availability
Participants did not provide consent for their data to be shared publicly, therefore the study data is not available for request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical consideration
The study was approved by the UNC IRB (protocol #13-2554).
Consent to participate
Participants provided written informed consent for study participation.
Consent for publication
Not applicable.