
Abstract
Ventricular assist device (VAD) and cardiac transplant patients experience significant strain on their physical and mental wellbeing postoperatively. Mental health and substance use disorders (MHDs and SUDs) have substantial effects on the quality of life and compliance of transplant and VAD patients. In this study, we compare and characterize MHDs and SUDs between VAD and cardiac allograft patients and transplant list patients with and without VADs. This study compares the incidence of MHDs and SUDs between VAD and cardiac transplant patients. Cohorts were defined using ICD-10 codes in TriNetX, a large public database. Patient characteristics were matched by using propensity score matching. Incidence was analyzed using the log-rank test. Statistical significance was set at p < 0.05. Survival analysis showed a statistically significant impact of adjustment disorder, nicotine dependence, and mood disorder in VAD patients as compared to cardiac allograft recipients. Depression and opioid use disorder had a significantly higher incidence in post-transplant patients compared to their VAD counterparts. Survival analysis showed that PTSD and mood disorder had a statistically significant effect on the patients waiting on transplant wait list without VADs as compared to those with VADs. MHDs and SUDs have profound implications on quality of life, survival, and medication compliance. The incidence of MHDs and SUDs differed between VAD versus cardiac transplant patients as well as the patients on the transplant waitlist with and without VADs. Mental health resources should be tailored to address risk factors that may be unique to each group of patients.
Introduction
More than one in five Americans suffer from Mental health disorders (MHDs) with rates continuing to rise. 1 It is estimated that 60% of transplant patients are affected by anxiety and depression. 2 Cardiac allograft serves as a curative solution to end-stage heart failure. Ventricular assistance devices (VADs) may be used as a destination therapy or temporary solution until transplant is possible or as destination therapy to alleviate symptoms and as a bridge to recovery for myocardial function. Stress and uncertainty accompanying these treatments have a profound effect on mental and physical health of this patient population. Use of immunosuppressive regimens, including use of calcineurin inhibitors and steroids, may pose challenges to patients’ mental wellbeing. Immunosuppression regimens are only used in patients undergoing heart transplantation to prevent organ rejection . No immunosuppression is needed preoperatively for VAD patients or those patients waiting for a transplant A two center study of 175 patients identified stressors on the wait list. Some of the worst stressors were the necessity to undergo a heart transplant, diagnosis of end-stage heart disease, anxiety experienced by close family, worsening symptoms, waiting for a suitable donor, uncertainty, lack of energy, feeling constantly fatigued, poorer control over life’s activities, and the need to depend on others. Interestingly as the wait period lengthened the number of stressors affecting the patient increased .The novelty or familiarity of the factor seemed to influence the stressfulness ratings of many variables during the period of waiting for the transplant. 3 The culmination of these factors has been found to negatively affect medication compliance and increase hospitalizations in post-transplant patients.4,5 Studies have identified elevated rates of anxiety, depression, and lowered quality of life in post cardiac transplant patients, while the literature is inconsistent in VAD patients.6–9 The role of advanced surgical therapies for heart failure on the development of additional MHDs and SUDs remains understudied.
We previously conducted a comprehensive analysis of MHDs and SUDs in cardiac transplant, waitlist, and VAD patients compared to heart failure patients. Both transplant and VAD patients had elevated incidences of depression postoperatively. Transplant patients had increased incidences of adjustment disorder and opioid use disorder compared to heart failure patients. VAD patients had decreased incidences of panic disorder and anxiety disorder following intervention. 10 While depression was significant to VAD and transplant patients, additional findings were distinct to each group. This suggested that the unique experience of undergoing VAD insertion or cardiac transplant may increase risk of MHD or SUD development and affect patients in a differential manner. However it must be emphasized that the acuity of illness is essentially the same in a patient who gets a VAD or a transplant but the driving force that influences one or the other therapy are the patient characteristics and co-morbidities and past medical history that would impact the outcomes post VAD or transplant surgery. This study compares the incidence of MHDs and SUDs between VAD and cardiac transplant VAD as well as VAD and transplant wait list patients. These findings may allow for further investigations of coping strategies and guide implementation of additional mental health resources to highlight the differential effects of the two widely used surgical therapies in today’s medicine to treat end-stage heart failure.
Materials and methods
TriNetX is a large research database, gathering decoded information from electronic health records. The Global Collaborative Network is a subset of TriNetX database that was used for this project. It includes 104 healthcare organizations across 30 countries and includes both uninsured and insured patients. TriNetX ensures the deidentification of Protected Health Information (PHI) datasets through a formal process certified by qualified experts, and complies with Section §164.514(b)(1) of the HIPAA Privacy Rule. The study is exempted by the Institutional Review Board.
Data analysis was comprised of two stages: (1) delineating and balancing baseline characteristics of VAD and cardiac allograft as well as VAD and transplant list cohorts based on ICD-10 diagnoses and (2) performing incidence and survival analysis of balanced cohorts. Propensity score matching was used to compare baseline patient characteristics. Patients with outcomes that occurred prior to transplant or VAD insertion were excluded. Configuring the analysis involved establishing definitions for the index event, criteria for outcomes, and the specified time frame. The survival analysis was performed using the Kaplan Meir test . Estimation of probability of outcomes was done using daily time intervals . The patients who left the cohort during the period of the analysis were censored.
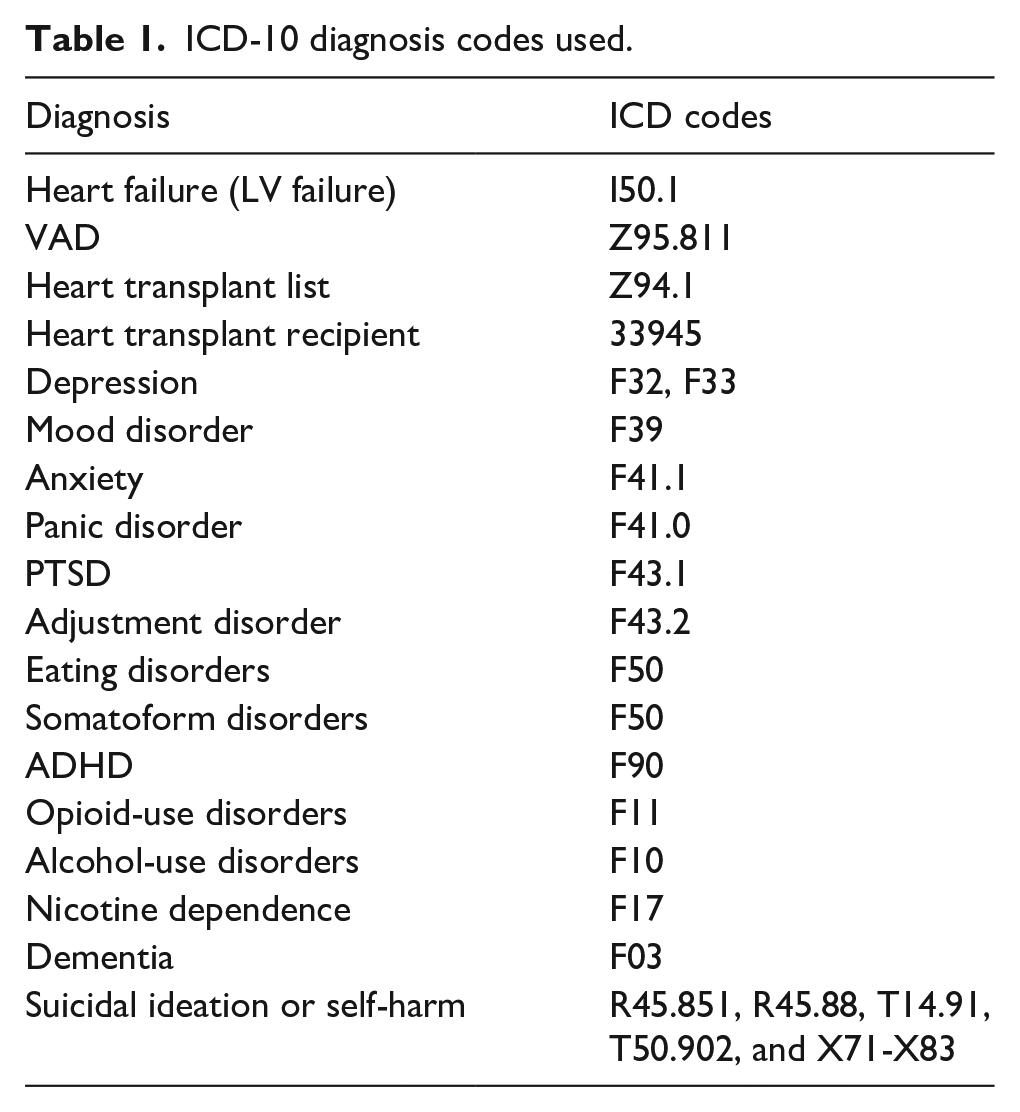
Table 1 presents the ICD-10 codes of outcomes studied in this investigation. The occurrence rates of MHDs and SUDs were compared among adult patients with VADs, and those who underwent cardiac transplant within 15 years from the index event. Index events occurring up to 20 years prior were included. An index event was defined as the moment a patient entered the cohort, defined as the date of transplant/VAD/entry to transplant list. Difference in incidence were examined using hazard ratios. Patients with pre-existing MHDs before the defined time window were excluded. Individuals aged between 0 and 100 were included. Propensity score matching was conducted through TriNetX (accessed on 7 June 2023) to address demographic and medical comorbidity imbalances. p-Values less than 0.05 were considered statistically significant.
ICD-10 diagnosis codes used.
Survival analysis was conducted using the Kaplan–Meier estimator. This estimated the probability of the outcome within specified time intervals. Censoring was applied to adjust for patients who exited the cohort during the analysis period. These patients were removed from the analysis after their last recorded event. The impact of VAD insertion and transplant were assessed using the Log-Rank test.
The frequency in which outcomes (MHDs and SUDs) occurred within the time frame (in this case, the postoperative period from transplant or VAD insertion) was assessed to determine incidence. The analysis included patients with zero instances. The incidence was calculated as the ratio of the number of new diagnoses observed during the analysis period to the total number of patients in the study cohort. The difference between VAD and transplant patients as well as VAD versus cardiac transplant list patients (without VAD) were assessed using the Hazard ratios and associated p-values.
Results
VAD versus cardiac transplant patients
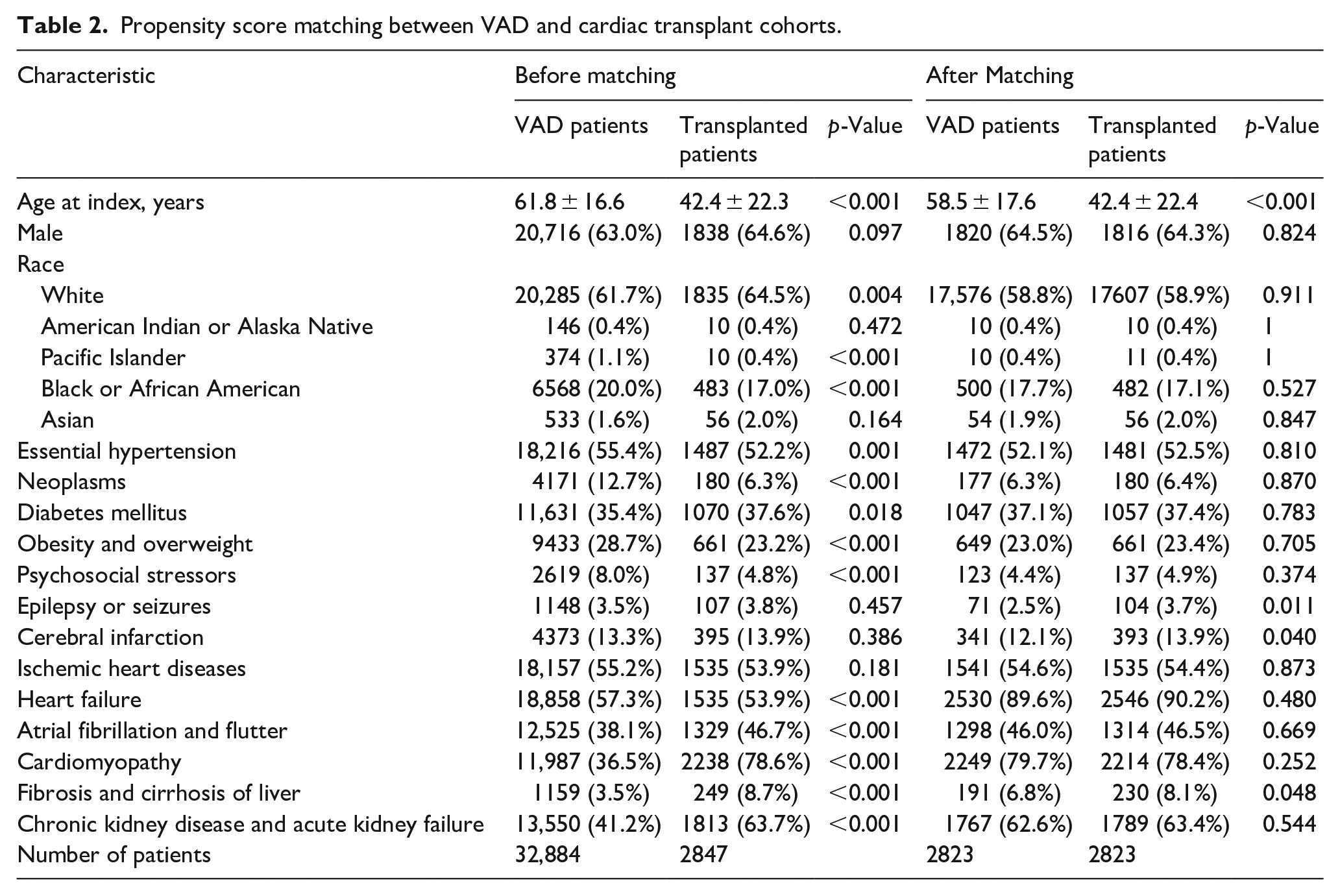
After propensity score matching, 2823 patients were identified in each cohort. The mean age at index was 58.5 ± 17.6 for VAD patients and 42.4 ± 22.4 for cardiac allograft patients. This was the only significant difference present between VAD and transplant patients. A comparison of baseline characteristics between the two cohorts are shown in Table 2. After propensity matching except for the mean age other baseline characteristics were not as highly significant between the two groups from the p-values noted in Table 2. Increase in the incidence of liver fibrosis in transplant patients was marginally significant with a p-value of 0.048. Cerebral infarction and consequent seizure activity was elevated in the transplant cohort with p-values of 0.04 and 0.011 respectively.
Propensity score matching between VAD and cardiac transplant cohorts.
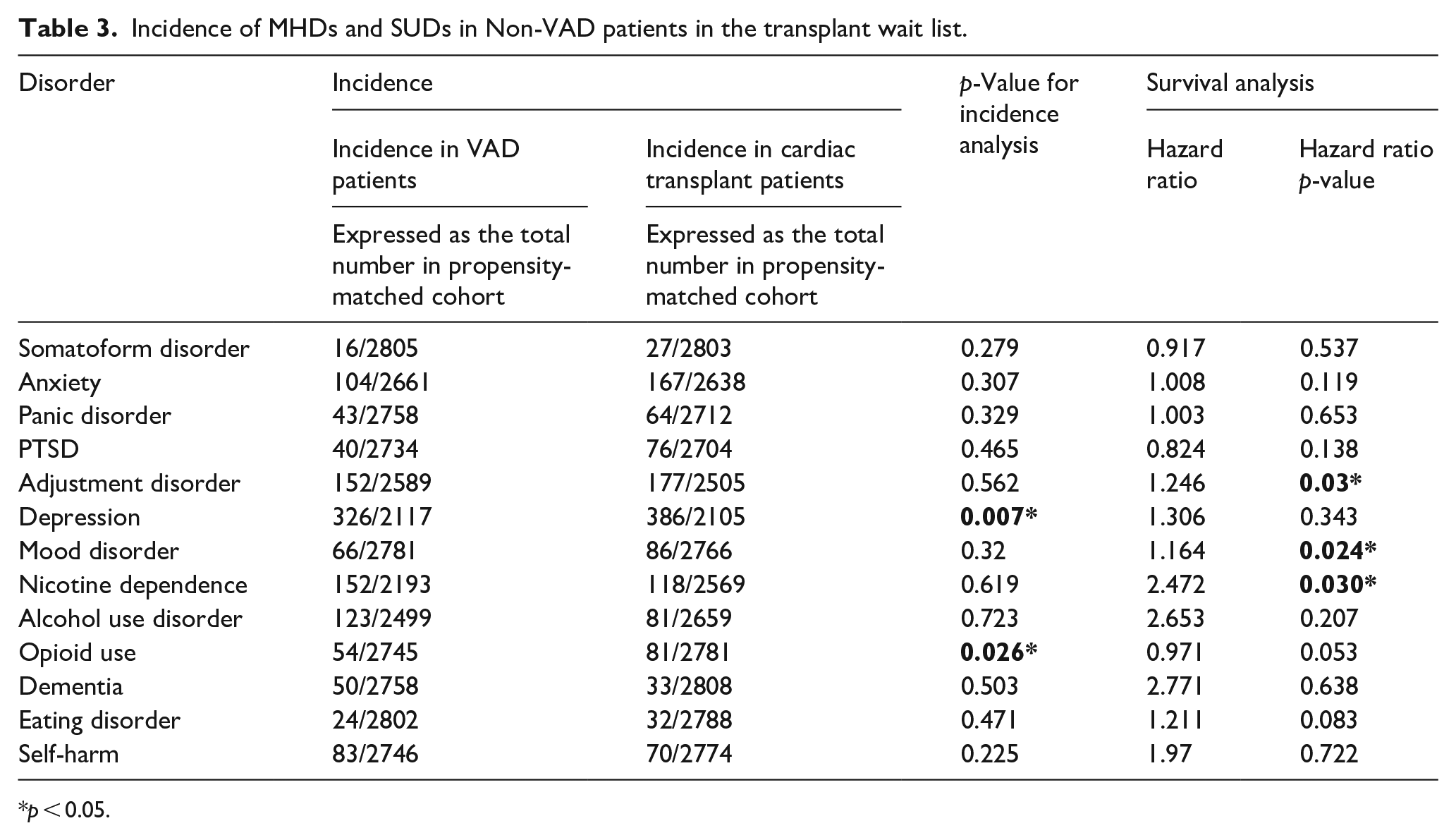
Depression and opioid use disorder had a significantly higher incidence in transplant patients as compared to those on a VAD but did not impact survival as shown in Table 3. However adjustment and mood disorders as well as nicotine dependence significantly affected survival as shown in Table 3. Figure 1(a, b, and c) show significant hazard ratios (HR) of 1.3, p = 0.03, 2.3, p = 0.03, and 1.3, p = 0.024 for adjustment disorder, nicotine dependence, and mood disorder respectively.
Incidence of MHDs and SUDs in Non-VAD patients in the transplant wait list.
p < 0.05.
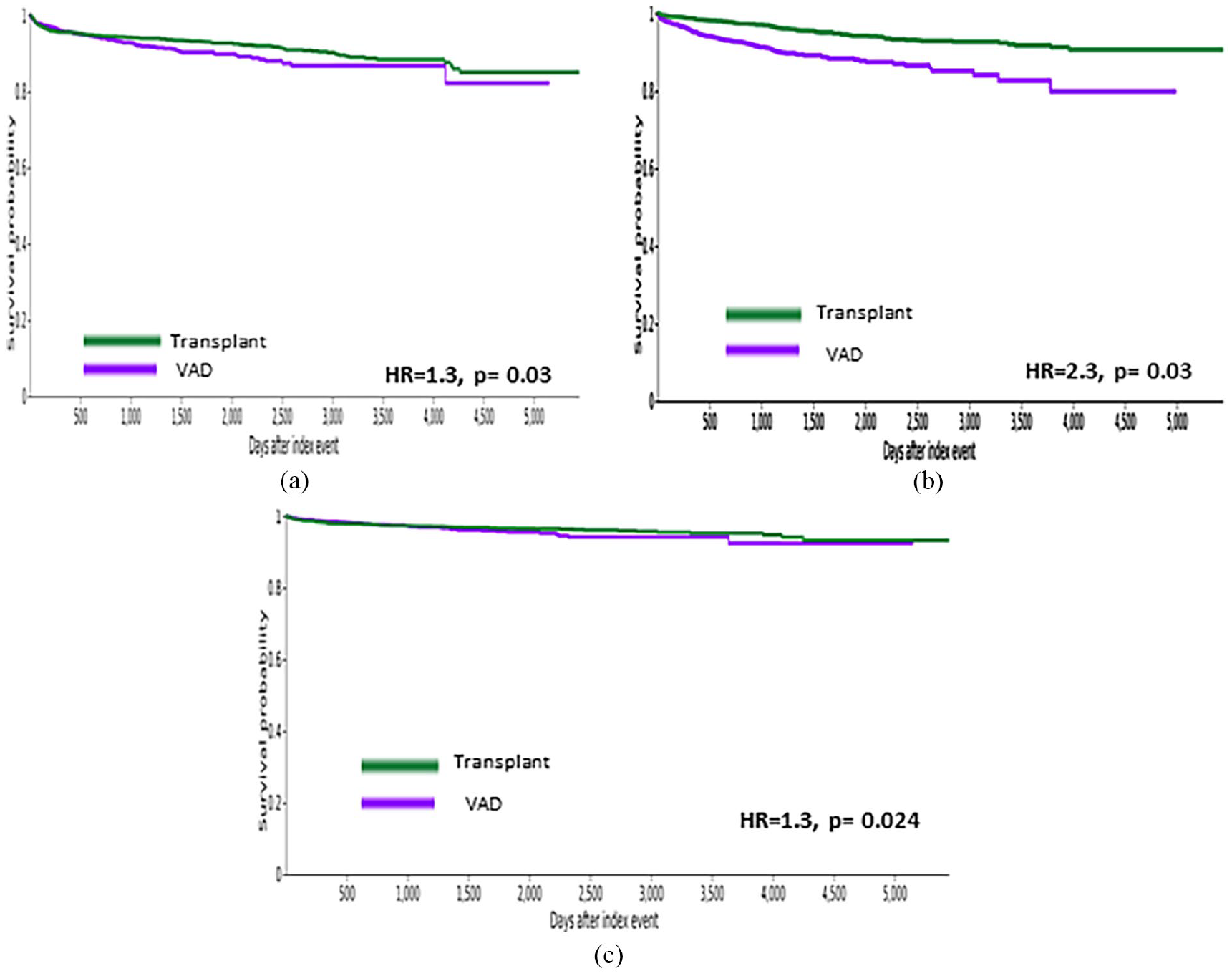
Survival curves for VAD versus cardiac allograft patients: (a) adjustment disorder, (b) nicotine dependence, and (c) mood disorder.
VADs versus non-VAD patients on the transplant list
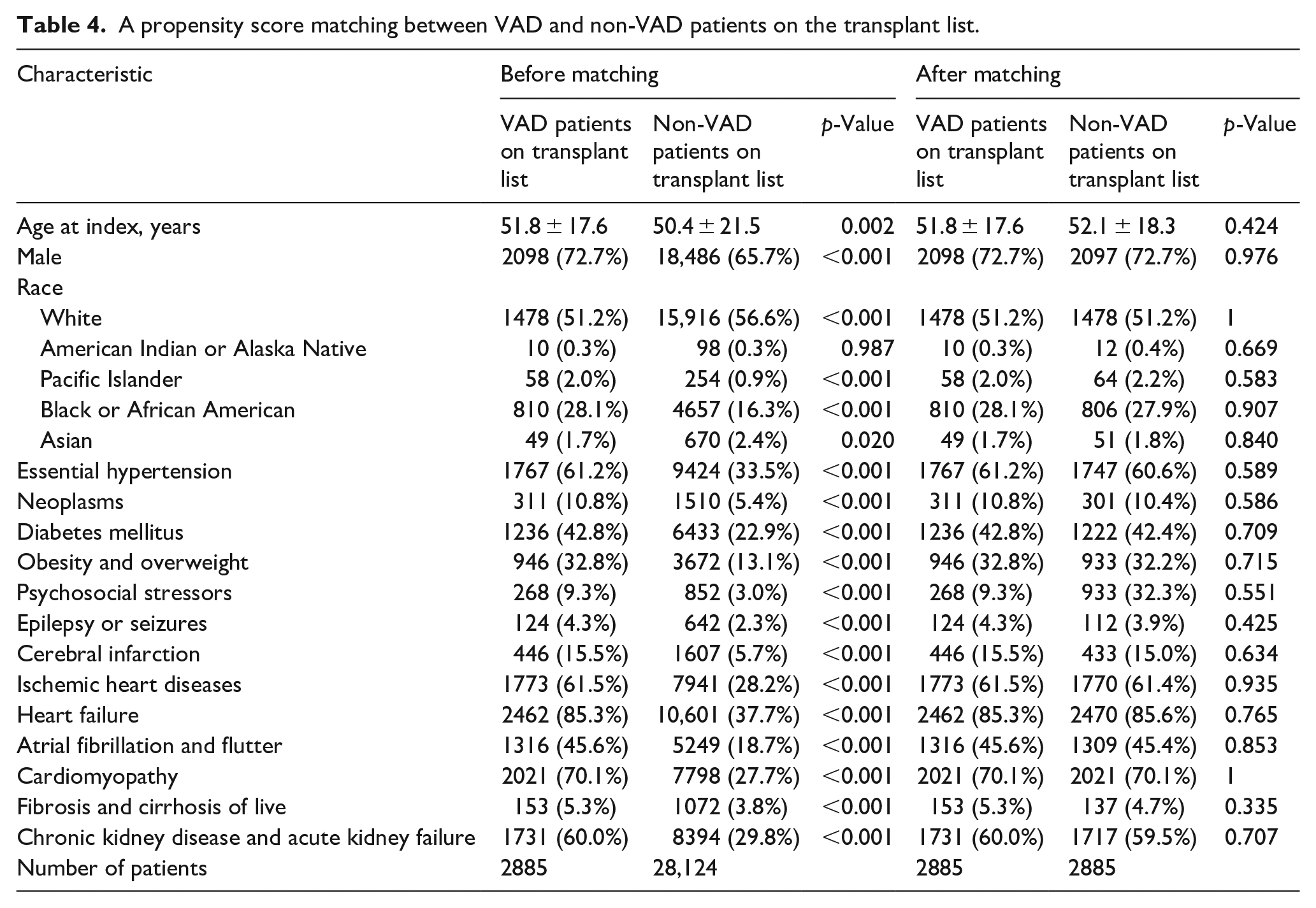
After propensity score matching, 2885 patients were identified in each cohort. The mean age at index was 51.8 ± 17.6 for VAD patients and 52.1 ± 18.3 for non-VAD patients on the transplant list patients. Baseline characteristics were not significantly different in the two cohorts. A comparison of baseline characteristics between the two cohorts are shown in Table 4.
A propensity score matching between VAD and non-VAD patients on the transplant list.
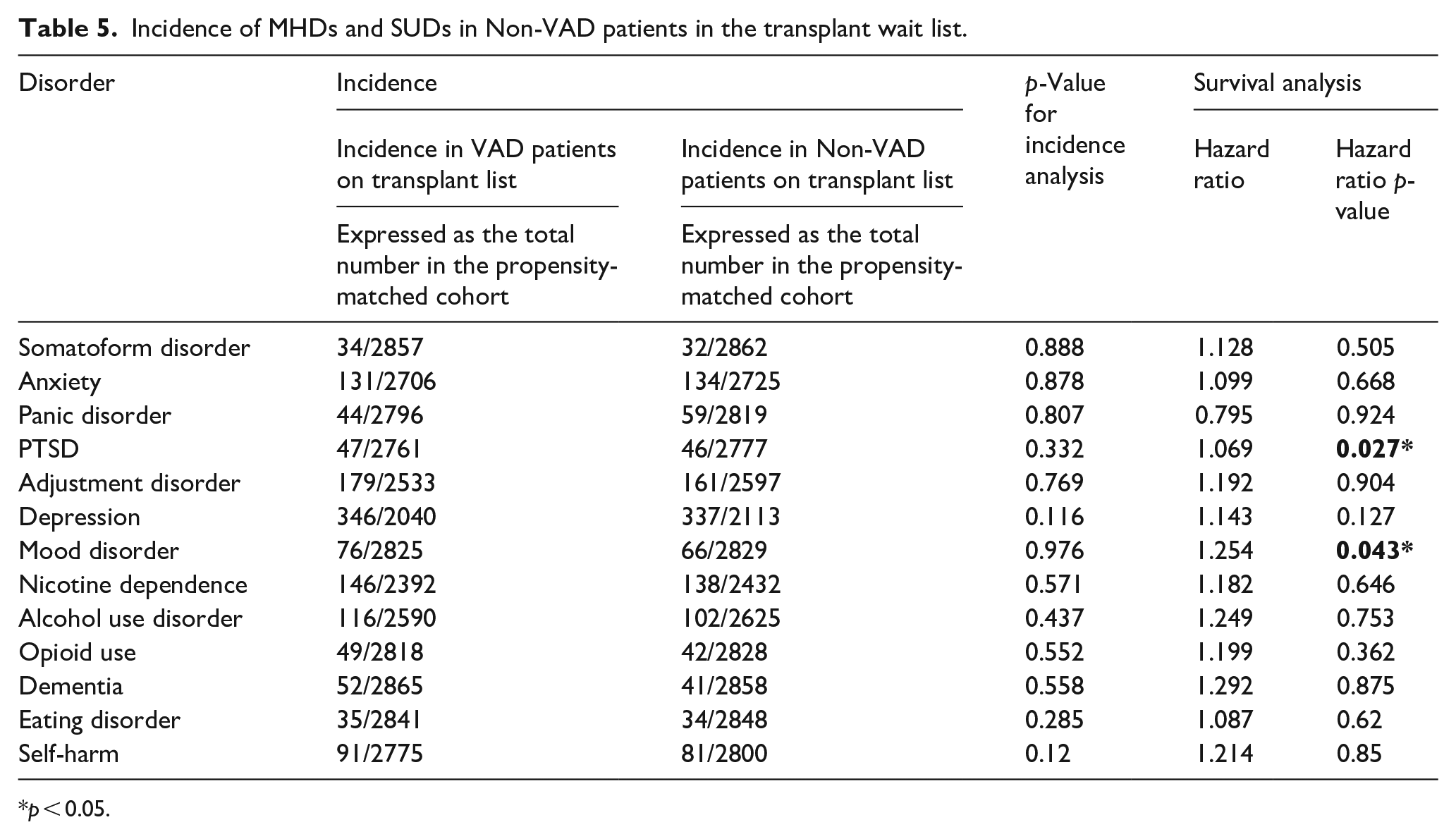
The incidence of MHDs and SUDs analyzed were not significant in this study as shown in Table 5. Survival analysis showed a statistically significant impact of a VAD as compared to non-VAD patients on the transplant list with respect to PTSD and mood disorder (Table 5, Figure 2). Figure 2(a) and (b) show a significant HR of 1.3 with a p-value of 0.03 and 0.04 respectively for both PTSD and mood disorder in the non-VAD patients on the transplant list.
Incidence of MHDs and SUDs in Non-VAD patients in the transplant wait list.
p < 0.05.
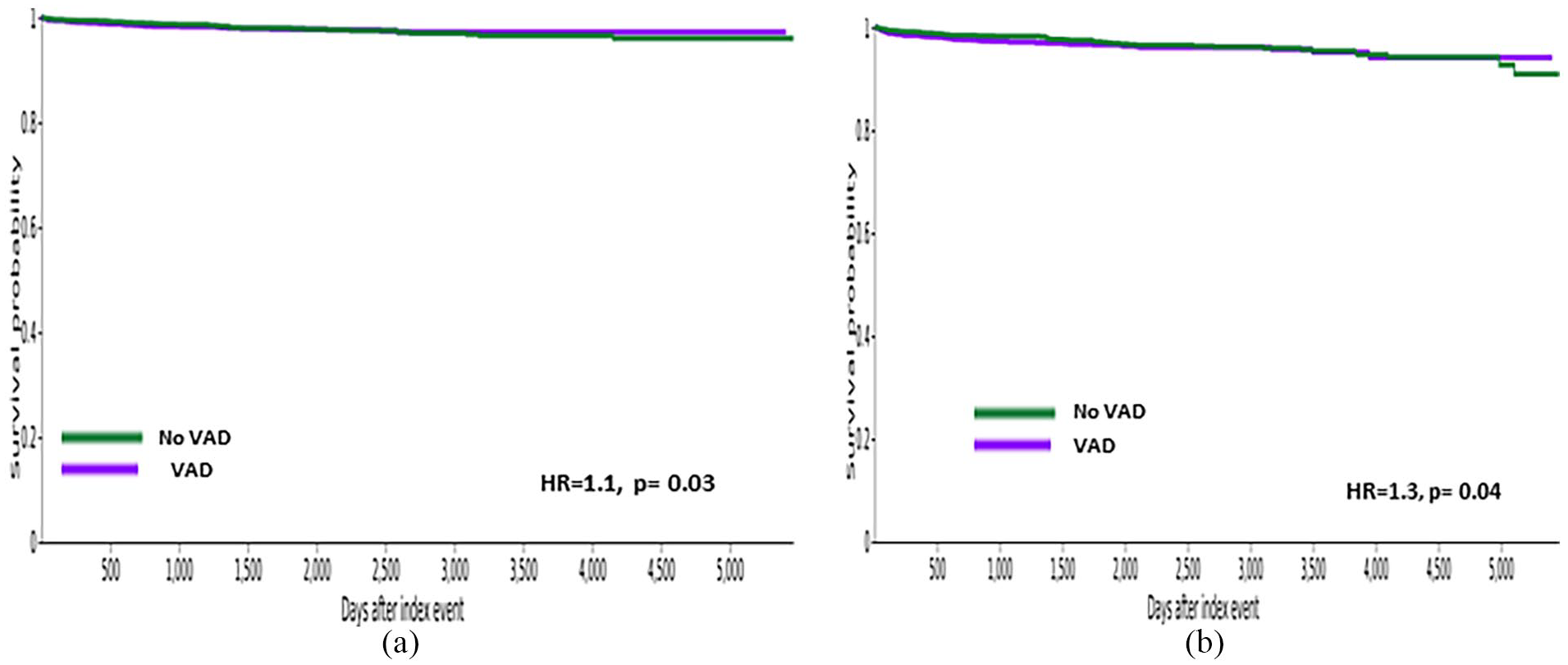
Survival curves for Transplant Wait list patients with and without VAD: (a) PTSD and (b) mood disorder.
Discussion
This study offers a comprehensive comparison of MHDs and SUDs in cardiac transplant and VAD patients. These results support existing findings that transplant patients suffer from increased rates of depression relative to VAD patients. Our previous study found that the incidence of depression was elevated in both VAD and transplant patients as compared to heart failure patients. 10 This is likely due to medical complications, lifestyle changes, and emotional volatility surrounding the post-transplant/post-VAD implantation period . In post-transplant patients treatment with steroids and other immunosuppressive agents also influence emotional health and well-being.4,11,12 This result conflicts with one study which found that heart transplant patients suffered from decreased rates of depression and anxiety compared to VAD or those undergoing aortic valve replacement. 13 Other studies found an initial improvement in depression in VAD patients immediately following surgery, but found that the patient reported outcomes for VAD patients were lower than those of transplant patients.7,14 One of these studies identified development of depression over multiple years whereas the others focused on the weeks to months following operation. These conflicting results warrant further study into the onset and duration of depression in VAD and transplant patients. While both VAD and transplant patients are at risk for depression, transplant patients may be disproportionately affected.
Cardiac transplant patients had an increased incidence of opioid use disorder relative to VAD patients. Use of opioids and benzodiazepines to manage acute pain following surgery contributes to the development of opioid dependence.4,15 The risk of opioid use disorder after transplant is estimated between 1.1% and 10%.4,16 Patients who underwent cardiac surgery with opioid use disorder were found to have multiple readmissions after surgery but rarely receive addiction management. 16 Interestingly, it was found that opioid use in VAD patients was associated with worse hemodynamics, with higher central venous pressures and pulmonary capillary wedge pressures. 17 Enhanced recovery after surgery (ERAS) programs for VAD surgery have been shown to decrease discharge on opioids as well as discharge to rehabilitation centers. 18 Increased use of such programs for cardiac transplant may be useful in attempting to mitigate opioid prescription after transplant.
Survival analysis showed a statistically significant impact of a VAD relative to transplant on adjustment disorder. Adjustment disorder refers to a dysregulation of emotions usually within three months of an identifiable stressor. These results suggest that the immediate months following VAD implantation may be more challenging to adjust to compared to transplant. While transplant patients must adjust to new immunosuppressive and lifestyle regimens, VAD patients must also learn to manage their change in life style with a new device within the body and a driveline that needs extreme care and caution. Additionally the VAD patients have limitations on certain activities such as swimming and other aquatic activities.
Though the acuity of patients undergoing VAD implantation and cardiac transplant are the same some preliminary studies do show that stress in the post-operative period can include demoralization and depression in heart transplant patients but in the VAD patients implanted as a bridge to transplant or as destination (till end of life) show no difference in sleep quality and markers of inflammation such as cortisol patterns or C-reactive protein levels in ether group.19-21
VAD and transplant patients have similar support systems depending on the acuity of the patient but studies are lacking how this could influence adjustment disorder. It is likely that different therapies may confer different psychological stresses and hence may need more intense support in VADs versus heart transplant. 22
Further studies are needed to differentiate psychological stresses in the different surgical therapies for end stage heart failure patients.
Nicotine dependence was found to negatively affect survival in VAD patients relative to transplant patients. Smokers who were also VAD patients found to have a higher proportion of pump thrombosis and driveline infections than nonsmokers. 23 Smoking cessation is a requirement prior to cardiac transplant. However, some patients return to smoking after surgery. Studies have found that return to smoking in transplant patients negatively affects survival by accelerating the process of graft vasculopathy and malignancy. 24 While smoking is deleterious for both populations, our result suggests that nicotine use may be a more significant risk factor for VAD than transplant patients.
This study paves the pathway to further investigate differences in the mental health issues seen in patients supported on a VAD versus those who have received a cardiac transplant as the two treatment modalities may confer a different set of challenges on the patients.
Limitations
This study is limited by its retrospective nature and lack of granularity of a large public database. It was also not possible to control for comorbidities of SUDs and MHDs. The use of ICD codes also limits our understanding of patients’ full clinical picture. Additionally, the use of a large, billing database is prone to some misidentification. Other limitations include screening for MHD and SUD is not as consistent as it should be and it is possible that some patients registering with new MHD and SUD may have had them before the index event, but were undiagnosed. Another aspect of this study is that transplant patients may be particularly motivated to appear well-mannered on screenings before their transplant due to concerns about eligibility to be on the transplant list and placement, which could obscure an accurate estimate of pre-existing MHD. Further studies should use prospective trials and focus on the efficacy of current counseling and psychiatric interventions to identify deficiencies in the management of these patient populations.
Conclusions
This is the first study to compare MHDs and SUDs in VAD patients versus cardiac transplant patients. Cardiac transplant and VAD patients experience significant strain on their mental and physical well-being throughout their treatment. These findings suggest that the risk of MHDs and SUDs after cardiac transplant and VAD may be unique to each patient population. Future mental health interventions should be designed with a focus on the MHDs and SUDs distinct for VAD versus transplant patients. Our results serve as foundations for further understanding of the patient experience before and after VAD implant and cardiac transplantations as well as for the development of much-needed future psychiatric treatment initiatives. This will help us tailor therapies for patients receiving different surgical therapies for end-stage heart failure and therefore improve outcomes via personalized medicine.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.