
Abstract
Background:
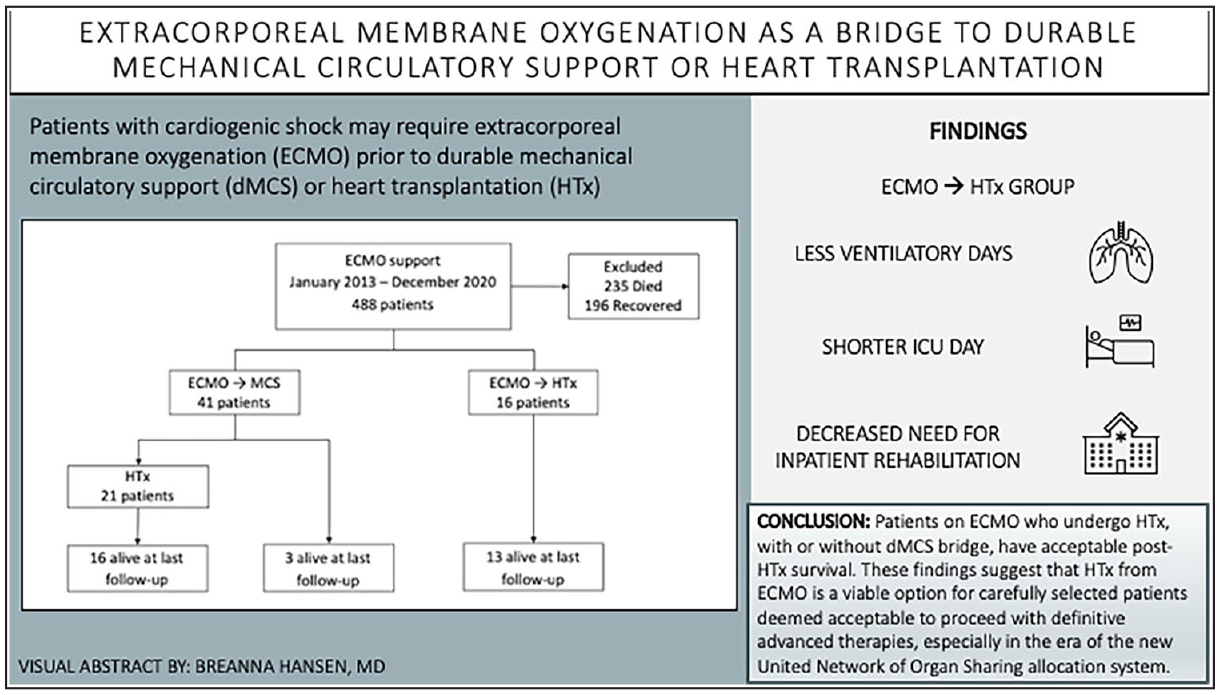
Patients with cardiogenic shock may require extracorporeal membrane oxygenation (ECMO) prior to durable mechanical circulatory support (dMCS) or heart transplantation (HTx).
Methods:
We investigated the clinical characteristics and outcomes of adult patients with ECMO support as bridge to dMCS or HTx between 1/1/13 and 12/31/20.
Results:
Of 57 patients who underwent bridging ECMO, 41 (72%) received dMCS (approximately half with biventricular support) and 16 (28%) underwent HTx, 13 (81%) after the 2018 UNOS allocation system change. ECMO → HTx patients had shorter ventilatory time (3.5 vs 7.5 days; p = 0.018), ICU stay (6 vs 18 days; p = 0.001), and less need for inpatient rehabilitation (18.8% vs 57.5%; p = 0.016). The 1-year survival post HTx was 81.3% in the ECMO → HTx group and 86.4% in the ECMO → dMCS group (p = 0.11). For those patients in the ECMO → dMCS group who did not undergo HTx, 1-year survival was significantly lower, 31.6% (p = 0.001).
Conclusion:
Patients on ECMO who undergo HTx, with or without dMCS bridge, have acceptable post-HTx survival. These findings suggest that HTx from ECMO is a viable option for carefully selected patients deemed acceptable to proceed with definitive advanced therapies, especially in the era of the new UNOS allocation system.
Keywords
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.