
Abstract
Aim:
When performing acute onset dialysis after insertion of catheters for peritoneal dialysis, pain exists and tunnel infections may develop. This study investigated whether patients benefit from the use of a surgical girdle and specific dressing postoperatively to prevent pain and tunnel infections.
Materials and Methods:
In 85 consecutive patients, the development of tunnel infections was followed. The patients used a surgical girdle when they were in supine position from day 1 to day 3. The peritoneal dialysis catheter was fixed in a curvature avoiding stretch in the exit. A total of 53 patients participated in a retrospective questionnaire to evaluate abdominal pain within the first 3 days after surgery either with or without girdle. A visual analogue scale from 0 to 10 was used.
Results:
In 23 patients, data on pain both with and without the girdle could be recorded. Pain was relieved more when using the girdle versus no girdle (median day 1 3.0 vs 4.0, p < 0.001, n = 30, Wilcoxon paired). The development of tunnel infections during the latest 7-year period (exposure period 1487 months) showed a total of three episodes (one every 495 months) of which one caused a subsequent peritonitis, while the other two resolved after antibiotic therapy. Peritonitis episodes appeared at a mean of 37-month interval.
Conclusion:
The use a surgical girdle for 3 days postoperatively and a fixation of the peritoneal dialysis catheter in a curved loop relieves the pain and results in few tunnel infections and subsequent episodes of peritonitis.
Background
According to peritoneal dialysis (PD) guidelines, the start of dialysis is usually postponed for about 2 weeks after insertion of the dialysis catheter (break in period) to avoid leakage. 1 However, if uremia is detected late or develops fast, immediate start of dialysis is necessary. Such immediate start is performed at our unit after surgical insertion of a self-locating PD catheter in local anesthesia performing a three purse-string suture technique. 2 To prevent from postoperative peritonitis, according to data from a controlled study, cefuroxime 1.5 g is given IV prior to the operation and 250 mg/L in the first PD-bag containing 1 L, postoperatively. 3 Such approach is also beneficial to avoid several admissions, such as for long-distance patients. The fill volume is initially limited to 1–1.5 L the first day. Postoperatively patients feel local pain in the operation wound but also by tension, 4 distension, and hematoma that may appear in the wound. To counteract such distension, we started to use a surgical girdle (Figure 1(a)–(c)) during parts of the first 3 days, such as when the patient was out of bed or had tendency to hematoma. In addition, we changed the bandage and placed the external part of the PD catheter into a loop so that stretching the catheter would not distend the exit site area (Figure 2). Analysis of clinical data was supported by approval of the local ethical committee (No. 2012-181-31M). We report here how we use such girdle and the outcome data regarding pain and tunnel infections.
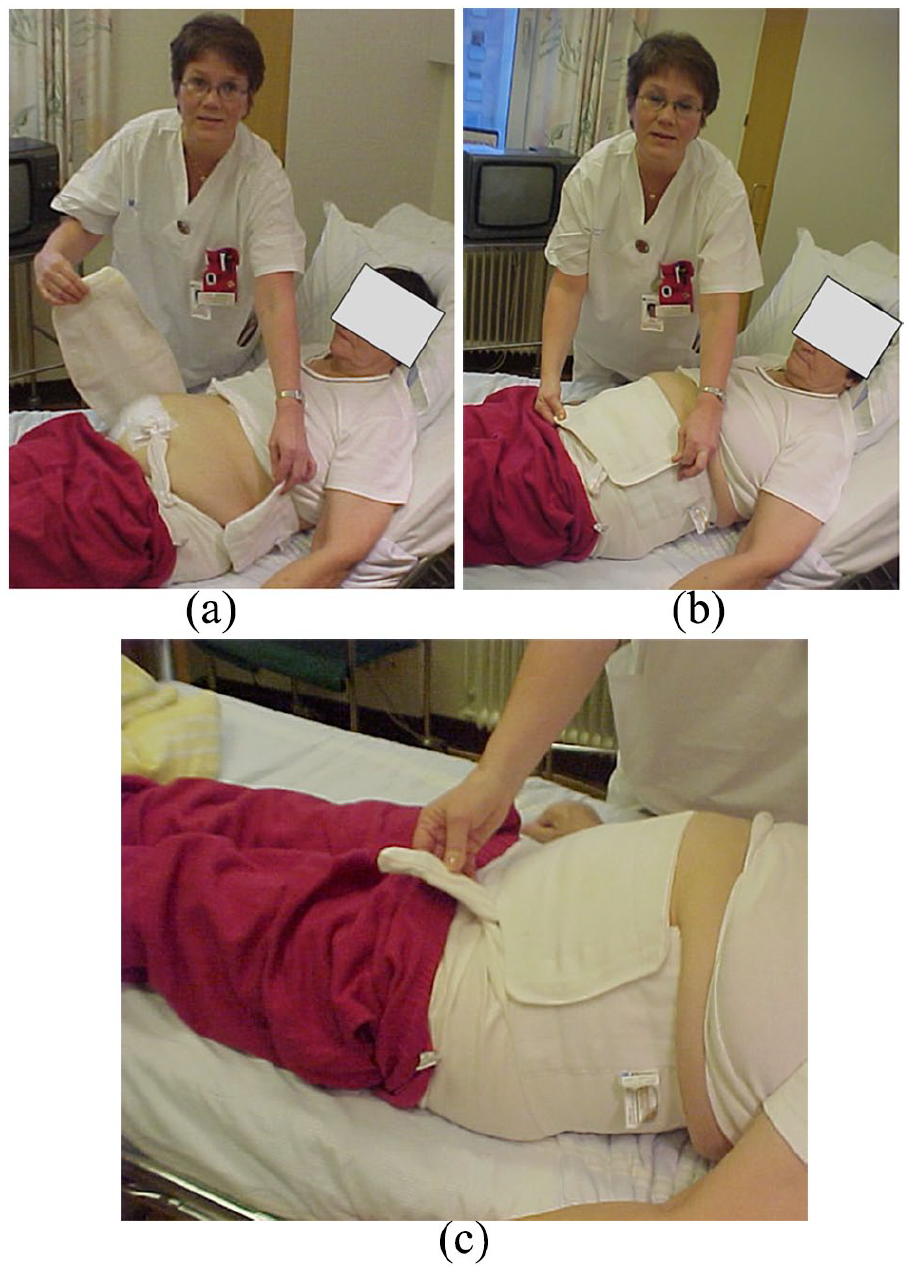
(a) Place the girdle behind the back and distend it. The girdle is preferably fixed around the patient when in a supine position. (b) The girdle thereafter is fixed at the front of the patient. (c) The external part of the peritoneal dialysis catheter is allowed to exit the girdle (not to compress it onto the skin). Fixation of the girdle includes the surgical wound as well as the exit site of the dialysis catheter. The girdle is tightened to only give a slight feeling of compression in supine position, to counteract the intra-abdominal pressure from the fluid instilled in the abdomen. If the pressure is high, this might counteract the ultrafiltration pressure achieved by the PD glucose. The aim is that the patients should feel comfortable and not oppressed.
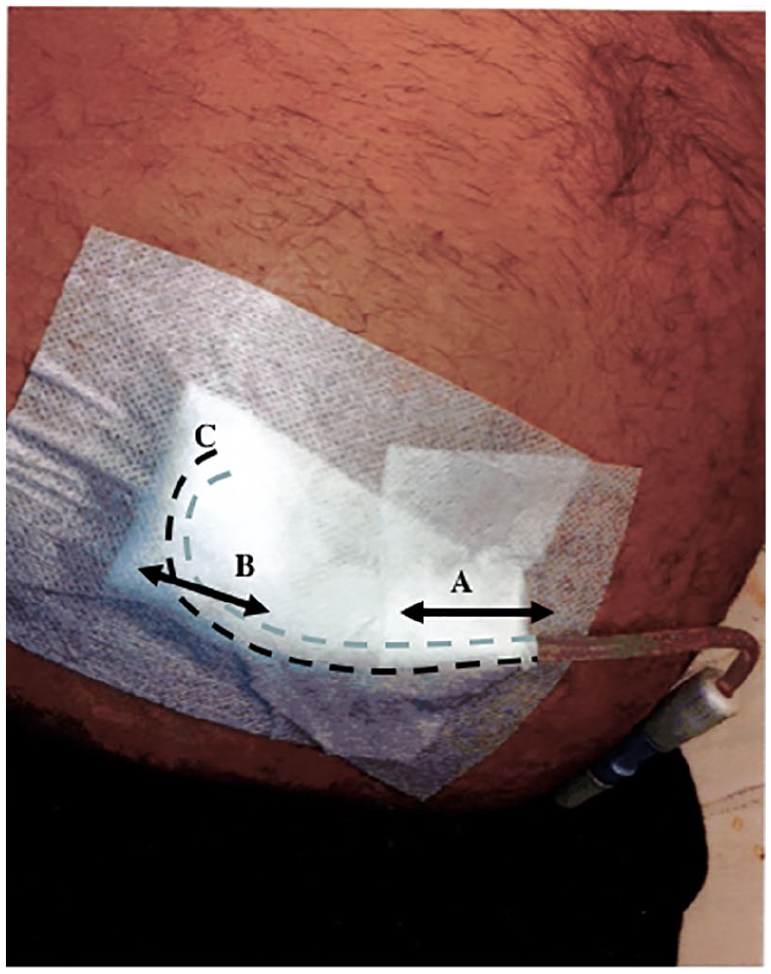
The catheter is fixed in a curved loop under the dressing (see hatched line) to avoid distension at the exit site if the catheter is stretched (direction A). The movements will transform to area B where only a change of the curvature appears while the exit at C is not altered. This location is used throughout the PD period. The exit site is flushed by chlorhexidine containing ethanol (70%) two to three times/week and each time after a shower before a new bandage is placed.
Methods and results
Regarding leakage and other complications, we refer to previously published data. 2 The first day, 1.5 L fluid is instilled (1 L if the patient feels oppressed) and conventional PD is started. Patient training will start thereafter. The patients are recommended mainly to stay in supine position for 24 h. Some patients will be out of bed before that—however, they will be told to use the girdle. During the following days, the fill-volumes are increased up to 2 or 2.5 L/dwell.
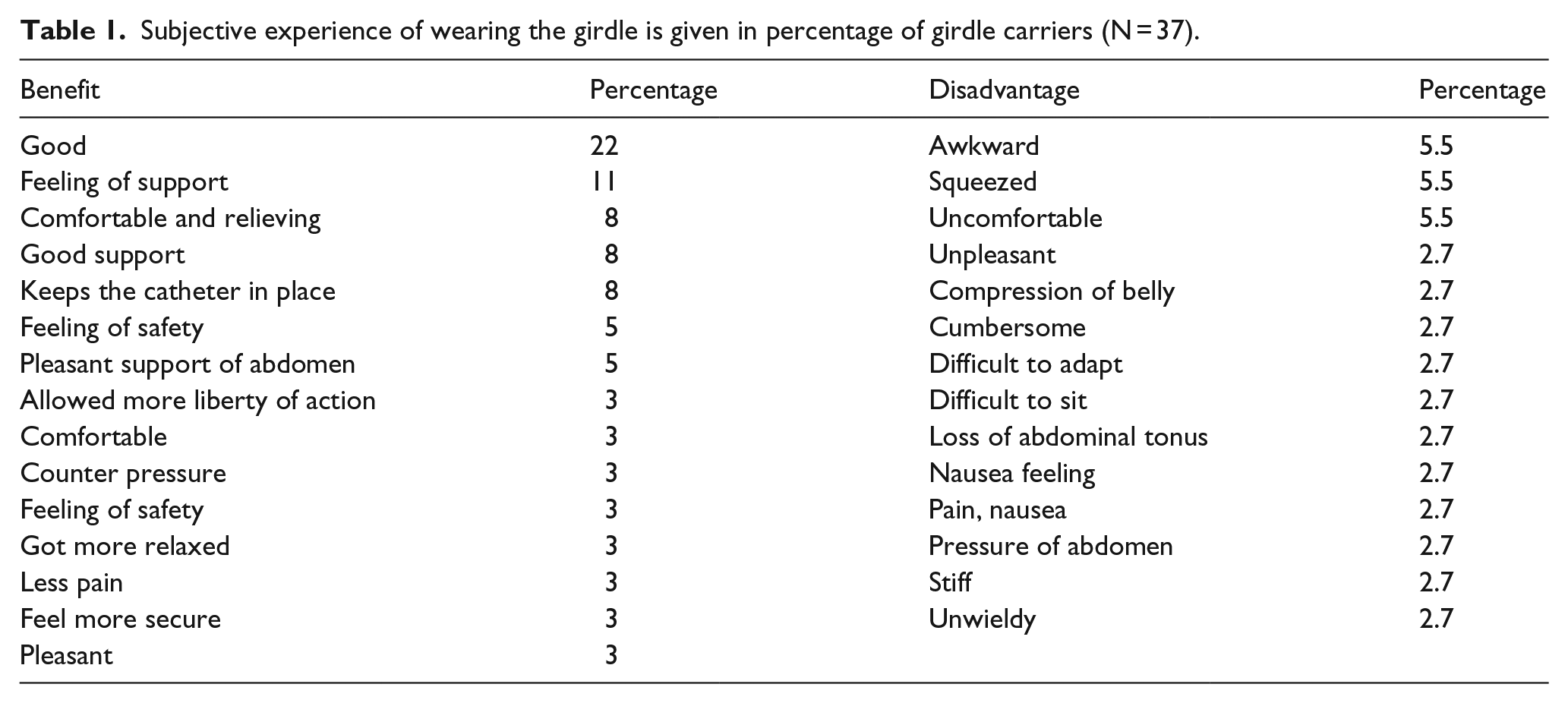
As a quality assessment study, data of a total of 85 consecutive PD patients were analyzed regarding outcome during the latest 7 years. Of these, 57 were asked to make a retrospective estimate of abdominal pain using a visual analogue scale (no pain = 0 up to severe pain = 10). Five of them did not participate in the questionnaire. Mean and median age was 55 years (range = 28–79 years). Reasons for renal failure were glomerulonephritis (32%), diabetes mellitus (26%), hereditary diseases (14%), nephrosclerosis (12%), interstitial nephritis (7%), and other diagnoses (9%). Of these, 34 experienced an advantage of the girdle (64%), while 17% experienced the girdle as unpleasant and 19% had no opinion. Of those who refused to use a girdle (n = 15), the girdle was too large, uncomfortable, and unpleasant. The experience of the girdle-carriers is given in Table 1. The experience of pain was less when using a girdle versus no girdle
Subjective experience of wearing the girdle is given in percentage of girdle carriers (N = 37).
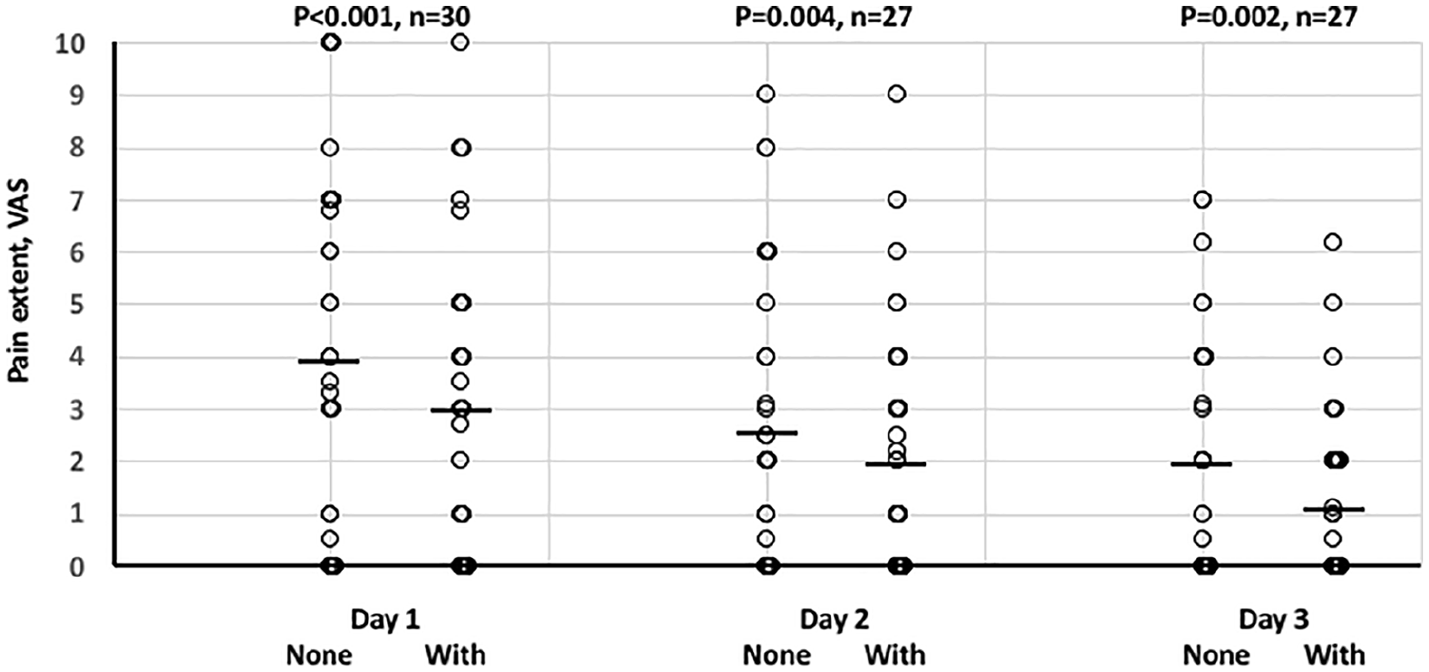
Patient experienced postoperative pain graded by visual analogue scale (“no pain” = 0 to “severe pain” = 10, VAS). Scatter plot of data is shown. Wilcoxon non-parametric paired analysis was performed. Median (-), p values, and number of pairs within each day (n) either experienced without the girdle (None) and with the girdle (With).
Peritonitis episodes appeared at a mean of 37-month interval.
Discussion
This insertion technique referred to allow early start of dialysis in both chronic and acute PD. This is an advantage to enable more patients into the PD program. Another option in numerous of acutely started dialysis would be to insert a central dialysis catheter and initiate hemodialysis. The risk for early or late leakage using this technique is low. By shortening the time in supine position after surgery, the risk for leakage increases. However, by adding a surgical girdle, this gives relief of pain and less wound pressure otherwise present due to distension in the operation wound. The girdle is easy to fix and gives a comfort also in supine position if distension in the operation wound gives more extensive pain. Our experience is that the girdle gives a firm pressure to the operation area, restricts dislocation of the dialysis catheter, and may prevent hematoma in the wound and thereby facilitate wound healing at the exit and tunnel site and results in subsequent less postoperative wound infections. A limitation is that numerous patients did not accept the girdle since it was too large and felt uncomfortable. A softer and adaptive compression might be worth to develop. The use of a loop of the extracorporeal PD catheter avoids local stretching and seems to help avoid exit site and subsequent TIs.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financially supported by Njurföreningarna i Norrland.