
Abstract
Background:
Despite the emergence of diverse programs in Mexico to address anemia and micronutrient deficiencies in disadvantaged groups, progress on reducing their prevalence has stagnated. In Mexico, anemia surveillance at the population level is conducted through the National Health and Nutrition Survey ENSANUT (for its acronym in Spanish).
Objective:
To overview the trends in anemia and iron deficiency (ID) from 1999 to 2018-19 in the Mexican population before COVID-19 pandemic.
Methods:
Data from five nationwide surveys in Mexico were used. Where available, data on anemia, ID, and ID anemia (IDA) were extracted from ENSANUTs 1999, 2006, 2012, 2016, and 2018-19 in participants from 1 to 99 years old. Blood sample collection methods were similar across surveys (1999-2018) where capillary drop blood was used to estimate Hb using a HemoCue and serum blood samples to measure ferritin and C-reactive protein concentration.
Results:
The trend in anemia prevalence shows a U-shape from 1999 to 2018-19 in <60 years old. In older adults (≥60 years), an increasing trend was observed. Anemia declined progressively from 1999 to 2012 but increased from 2016 to 2018-19 in comparison with 2012. In contrast, ID declined from 2006 to 2018-19, mainly in children, while IDA did not change over this period. In older adults, ID prevalence remained constant over time.
Conclusions:
The shifting trend in anemia prevalence across ENSANUTs 1999 through 2018-19 did not mimic the decreasing trend of ID over the same period of time. Other noncausal factors seem to play an important role in the variability of hemoglobin measurements.
Plain language title
Overview of Trends in the Prevalence of Anemia and Iron Deficiency in the Mexican Population From 1999 to 2018-19
Plain language summary
In Mexico, anemia surveillance has been monitored through the National Health and Nutrition Survey since 1999. Nonetheless, progress on reducing their prevalence seems to be stagnated despite the emergence of diverse social programs in Mexico to tackle micronutrient deficiencies in children and women. The main cause of anemia in children and women is iron deficiency (ID). Any progress in tackling ID should be reflected in anemia prevalence. To investigate the prevalence trend, we used information about anemia (based on hemoglobin concentration) and ID (based on serum ferritin levels) where available, from 5 nationwide surveys in Mexico among participants from 1 to 99 years old, to discuss some of the potential factors behind anemia and ID trends. From 1999 to 2018-19, we observed an ¨U” shape in the prevalence of anemia in all age groups <60 years old, contrasting with the prevalence of ID, which trend is in decline. No major changes in terms of social programs can explain the trend in anemia. In fact, other nutritional indicators seem to have improved in Mexican children. A major difference in the measurement of anemia and ID is that hemoglobin was measured in situ using drop of capillary blood in HemoCue, a portable photometer, while ferritin was measured in venous blood in the central laboratory. While many external factors might influence the hemoglobin measurement in the field setting, it seems that the technique of finger prick capillary introduces more errors to the measurement of hemoglobin than other techniques (e.g., pool capillary or venous blood using HemoCue). This difference, in turn, affects anemia diagnosis. Since the drop of capillary blood has been widely acceptable, we did not perform any validation of hemoglobin measurement in those past surveys, so we cannot role out the contribution of other factors that affected hemoglobin measurement. Future studies should use venous blood to improve anemia classification; otherwise, validation studies should be carried out to improve hemoglobin measurement when using capillary blood.
Introduction
Anemia is a global public health problem, of which iron deficiency (ID) is the main contributing factor across low- and middle-income countries (LMIC) worldwide. 1 Nutrition surveillance is essential to track the progress of the World Health Assembly goal of a 50% reduction in anemia in women of reproductive age by 2025. 2 This reduction can only occur through the implementation of programs designed to tackle the causes of anemia. In addition, it is critical to assure the quality of hemoglobin measurement to quantify changes attributable to these interventions.
In Mexico, anemia surveillance at the population level is conducted through the National Health and Nutrition Survey (in Spanish, ENSANUT). Despite the emergence of diverse programs in Mexico to address anemia and micronutrient deficiencies in disadvantaged groups, 3 -5 progress on reducing their prevalence has not been consistent. A study showed that the prevalence of anemia in the Mexican population declined steadily from 1999 to 2012 before experiencing an increase in 2016 and 2018-19. 6 The variability of Hb values informing anemia estimations through these surveys may be explained by diverse factors.
This article presents an overview of anemia prevalence from 1999 to 2018-19, and ID and ID anemia prevalence from 2006 to 2018-19 in the Mexican population and we discuss some of the potential factors driving those trends. In order to allow comparability between surveys, we will focus our overview of trends prior to the COVID-19 pandemic, since this pandemic worsened some nutritional indicators in the Mexican population. 7
Material and Methods
The ENSANUTs are probabilistic surveys with multistage sample directed to households in urban and rural areas, representative of the national population, which were conducted periodically from 1999 through 2018-19 (https://ensanut.insp.mx). The ENSANUTs from 1999-2006 determined hemoglobin concentration using the second drop of capillary blood obtained by a one-bezel lancet using a portable HemoCue B-system (Angelholm, Sweden). In subsequent ENSANUTs (2012, 2016, and 2018-19), the HemoCue 201+ was used instead. Participants with available measurements of Hb, s-ferritin, and c-reactive protein (CRP) concentrations were selected from the database of ENSANUTs. The age groups were divided into 1 to 4 years of age (preschoolers), 5 to 11 years (scholars), 12 to 19 years (adolescents both sexes), women 20 to 49 years, and older adults both sexes (≥60 years).
All ENSANUT waves obtained venous blood samples in a subsample of the population (around 30%). Nonetheless, micronutrient status and particularly serum ferritin in children and adult women was only collected in 2006, 2012, and 2018-19. For older adults, serum ferritin data are available in 2012 and 2018-19. Venous blood was collected from the left arm in vacutainer free-mineral tubes. Blood samples were spun down in situ at 3000 g, then serum was separated and placed in cryovials in a liquid nitrogen container until delivery to the Nutrition Laboratory (INSP, Cuernavaca, Morelos, Mexico) for storage at −70°C until use. In 2006, ferritin and CRP were measured for children and women using Dade Boehringer, Inc kits in the equipment: BNproSpectrometer, Germany. For the 2012-2018 surveys, ferritin and CRP were measured through chemiluminescence in the automatic immunoanalyzer Architect CI8200 (Abbott diagnostics, Wiesbaden, Germany) using the material also provided by Abbot Co.
Iron deficiency was defined as serum ferritin <12 ng/dL in children <5 years old and <15 ng/dL in children ≥5 years old. 8 Ferritin values were preadjusted for inflammation according to methods used by Thurnham. 9 A CRP concentration of >5 mg/dL was defined as inflammation. Anemia was defined according to WHO criteria. 10 Hemoglobin data were adjusted by altitude in localities above 1000 m above sea level. 11
Information on other micronutrient status associated to anemia (deficiencies of vitamin A, B12, folate, and vitamin C) were only measured in children aged 1 to 4 years in some ENSANUT waves. Therefore, we decided to use ID data, since s-ferritin is the only one indicator measured in different age groups (children 1-11 years, adult women, and older adults) across ENSANUT waves, and because ID has been considered the main cause of anemia in Mexico, 12 as well as in LMIC. 13 Therefore, any change in ID should impact the anemia prevalence.
Statistics
Data were extracted from previous publications on anemia and micronutrient deficiencies in the Mexican population using the ENSANUT’s datasets. They were presented as prevalence or mean with 95% CI, adjusting for the complex design of the survey. STATA v17 was used to perform additional descriptive analysis using the SVY module for complex survey design.
Ethics
The protocol of the each ENSANUT wave has been approved by the Research, Ethics and Biosecurity Committees at the National Institute of Public Health, Mexico.
Results
Trends in the Prevalence of Anemia and Iron Deficiency
From 1999 to 2012, a significant drop in anemia prevalence was observed in all age groups within the sample, but afterward, a significant increase was observed in 2016 and again in 2018-19 (P < 0.05). In 2012, the prevalence of anemia was at its lowest across all population groups, but the overall prevalence increased in 2018 (Figure 1).
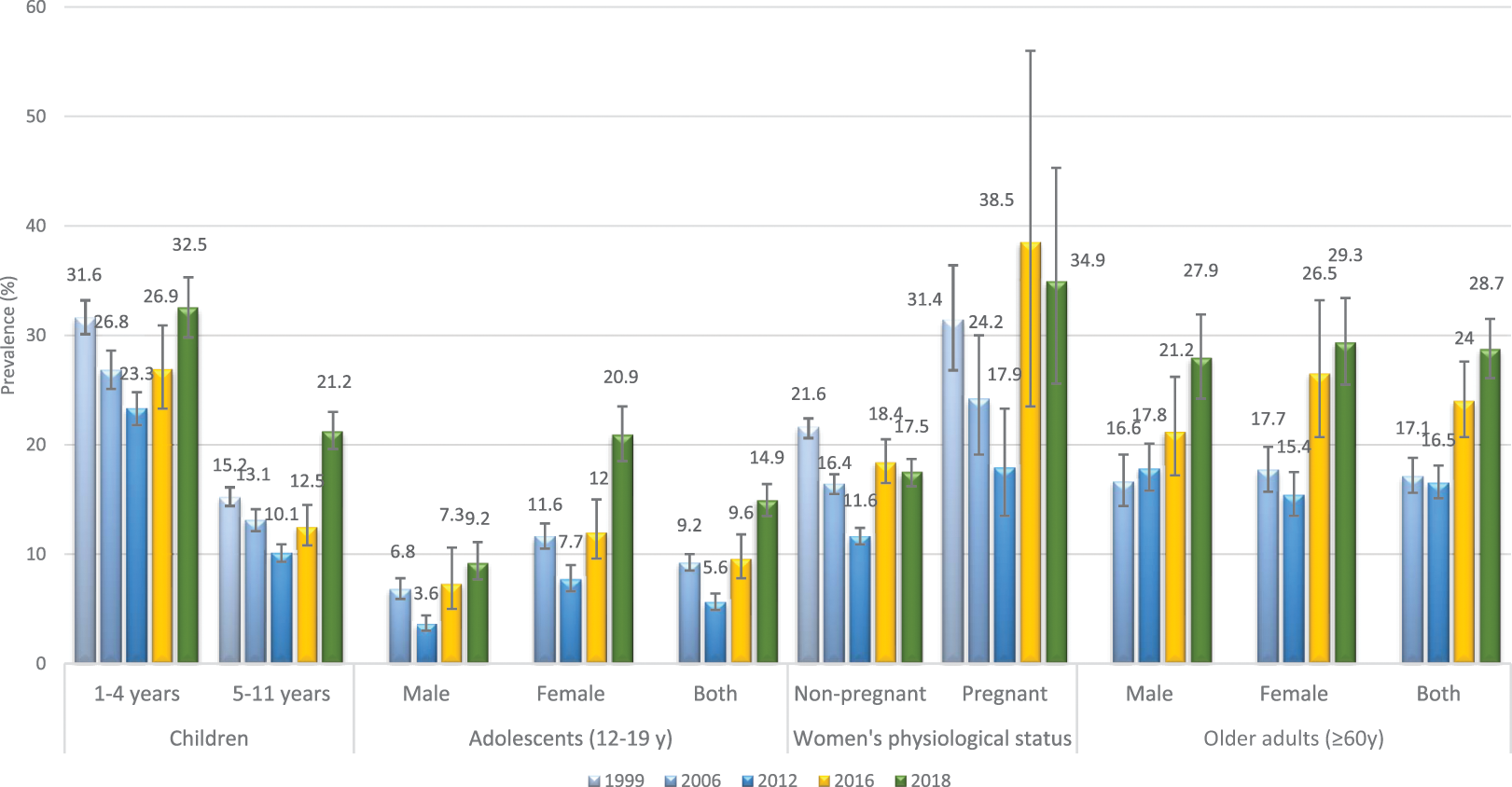
Trends in the prevalence of anemia in the Mexican population across the National Health and Nutrition Surveys, ENSANUTs 1999-2018-19.
The prevalence of ID in 2006, 2012, and 2018 was in decline in children from 2006 to 2018-19, in women from 2012 to 2018-19 but not in older adults which remained without change over 2012 to 2018-19. Iron deficiency anemia showed a significant drop among children aged 6 to 11 years, while in others age groups it did not change (Figure 2).
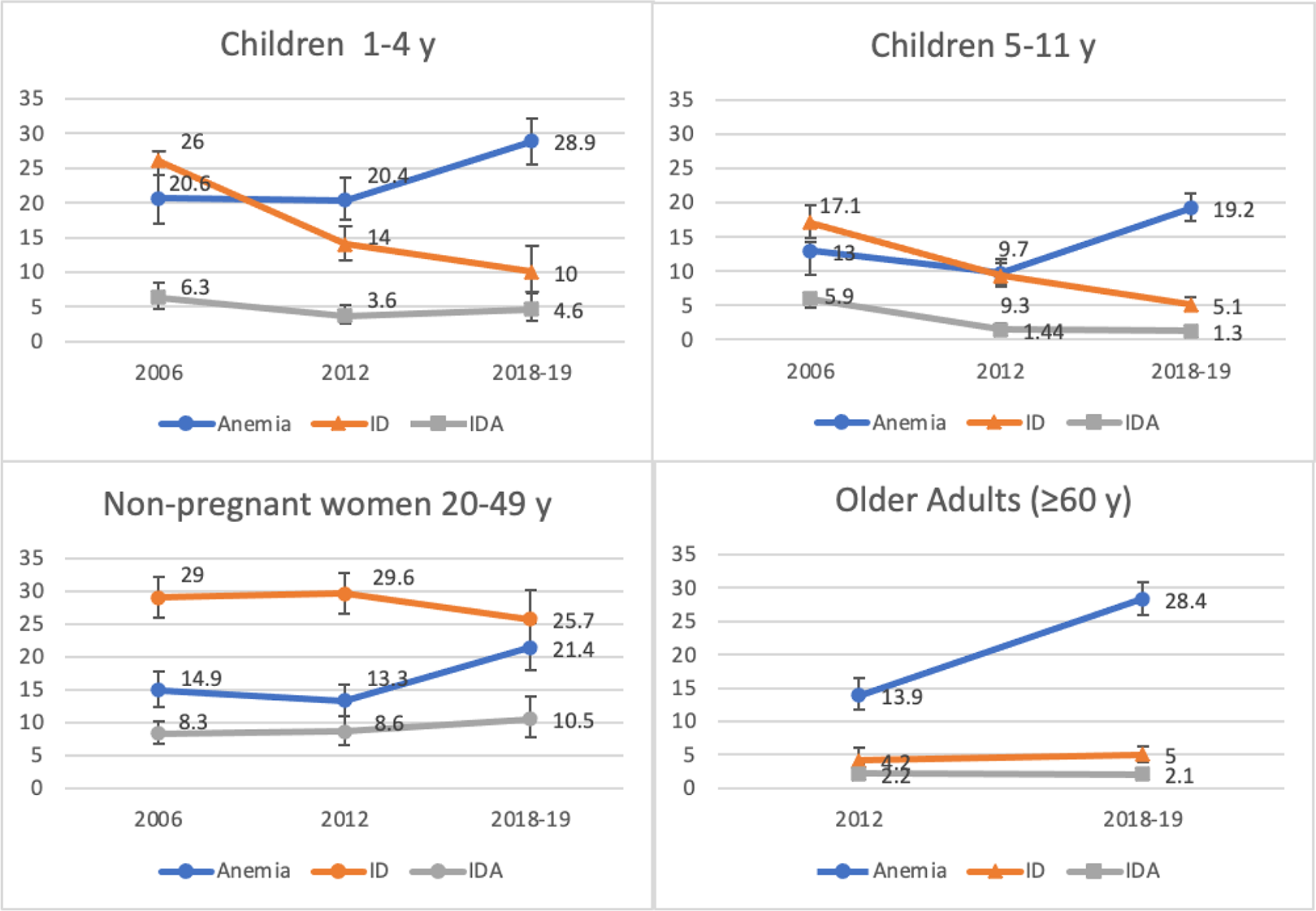
Trends in the prevalence of anemia, iron deficiency, and iron deficiency anemia in the subsample of population with serum sample on file. ENSANUTs 2006, 2012, and 2018-19.
In children 1 to 4 years of age, the prevalence of inflammation did not change significantly affecting around 11.0% of them. In children 5 to 11, the prevalence was around 9.0% in the 3 surveys (2006, 2012, and 2018-19) (Figure 3).
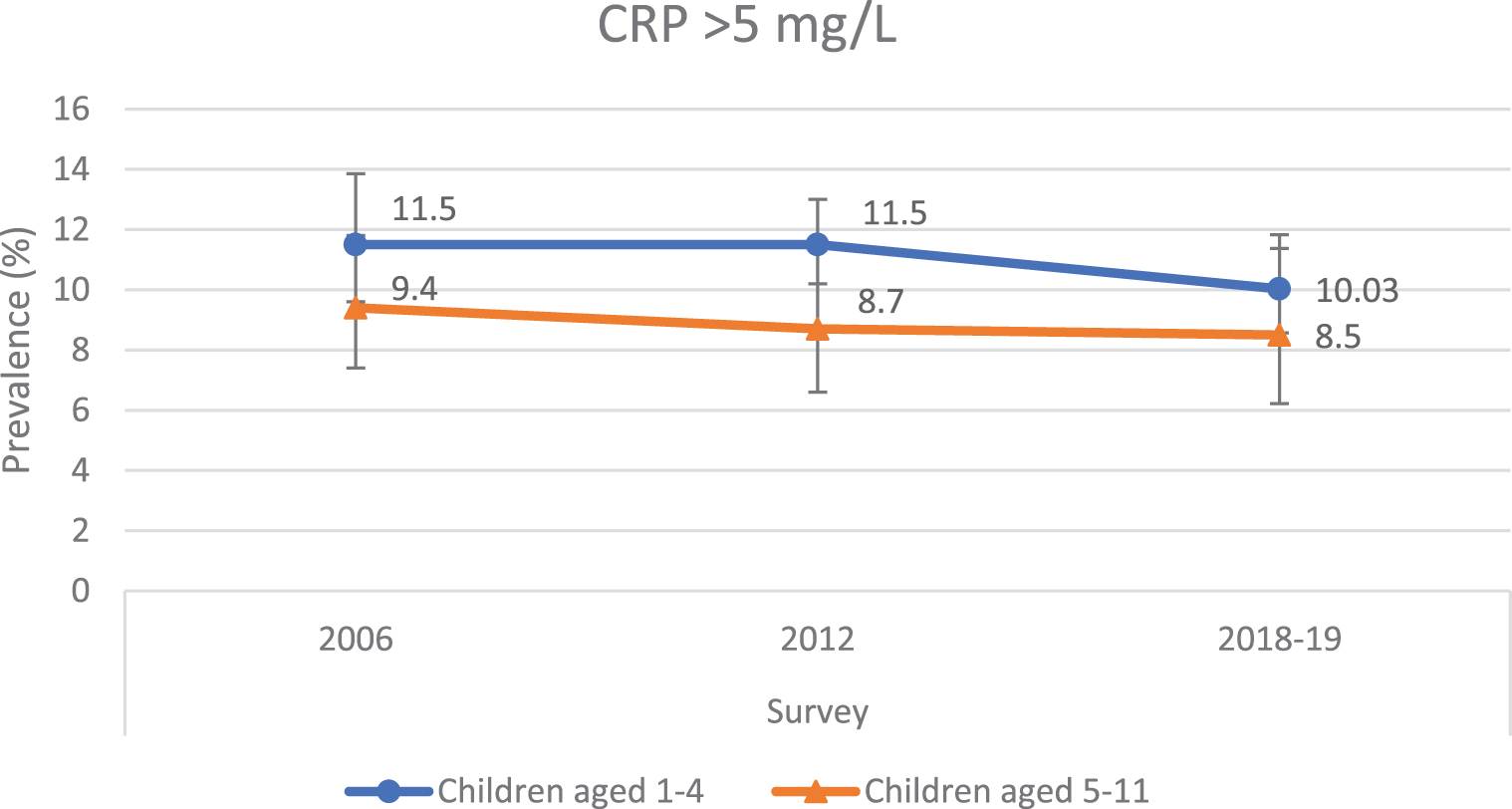
Trends in the prevalence of inflammation in Mexican children, ENSANUTs 2006, 2012 and 2018-19.
Distribution of Hb Concentration in Children Aged 1 to 4
When comparing the distribution of Hb mean concentration across ENSANUT waves of 2006, 2012, and 2018-19 in children, no differences were observed between the 2006 and 2012 waves (12.01 and 12.06 g/dL), while compared to both previous years, the 2018 wave showed a difference between means on average 0.4 g/dL lower. In the 2006 and 2018-19 waves, the prevalence of mild anemia was 14.8% and 17.2%, for moderate anemia 5.5% and 11.6%, and for severe anemia <0.2%, respectively
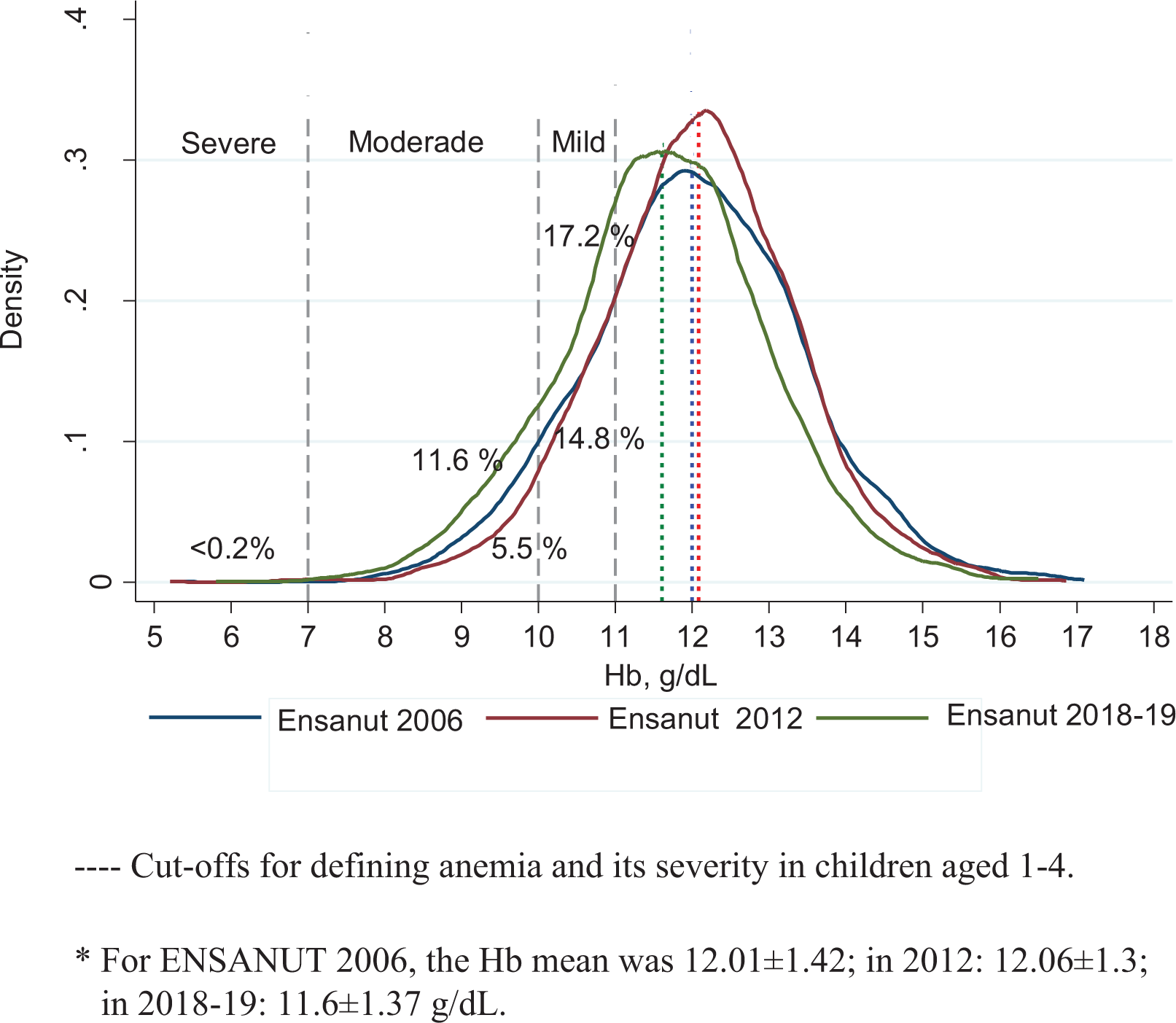
Distribution of hemoglobin values in children aged 1 to 4 in the ENSANUTs 2006, 2012, and 2018-19. For ENSANUT 2006, the Hb mean was 12.01 ± 1.42; in 2012: 12.06 ± 1.3; in 2018-19: 11.6 ± 1.37 g/dL.–– Cut-offs for defining anemia and its severity in children aged 1 to 4.
Discussion
The prevalence of anemia from 1999 to 2018-19 shows a U-shape across all age groups <60 years of the Mexican population. In older adults (≥60 years), data are available from 2006 and shows an increase in 2018-19. Since 2012, an increasing trend in anemia prevalence can be observed, which contrasts with the descending trend in ID in younger (<60 years) population. Since the methodology for Hb and ID measurement has remained unchanged since 2012, causal and noncausal factors other than ID may be contributing to Hb variability.
Causal factors for anemia at the population level may vary in magnitude by age-group. For instance, in LMIC, anemia in children and women of childbearing age has been associated with ID and micronutrient deficiencies, 1,13 while in adults from high-income countries, the same condition has been associated with inflammation and subjacent disease. 13 The patterns of these conditions may have been shifting in Mexico alongside the well-documented epidemiological and nutritional transition. 14
Deficiencies of micronutrients including vitamin B12, folate, retinol, and vitamin D affect erythropoiesis through various mechanisms. 1 These deficiencies may be the result of poor intake from the food source or higher biological demand in the presence of infection or disease. Nevertheless, the prevalence of such deficiencies in Mexican children and women is in decline when compared to the data from 2006 15 to 2018-19. 16 In children, folate and B12 deficiency dropped from 3.6% to 0%, and from 7.3% to 5.1%, over the period 2006-2018-19, respectively; while vitamin A depletion dropped from 15.7% 17 to 4.7% over the period 2012-2018-19. These reductions may be associated with multiple factors, such as increased access to fortified foods, higher intake of nutrient-dense foods, or a natural tendency over time.
Social programs targeting disadvantaged groups have also been pivotal to tackling these deficiencies. The consumption of fortified foods (LICONSA milk) or supplements with micronutrients that provide one RDA of iron and other micronutrients were associated with a reduction in zinc deficiency, ID, and anemia for beneficiaries of one or both of the social programs LICONSA and PROSPERA. 3,4 PROSPERA was active from 2006 to mid-2018, while the LICONSA milk program is ongoing; therefore, such programs may not have contributed to the increase in anemia prevalence observed in 2018.
In 2008, the financial crisis in Mexico could have worsened the food security situation, which was estimated to affect the 21.7% of the population who lacked access to food. 18 Afterward, food insecurity (FI; moderate and severe) in Mexico dropped from 27.5% to 22.9% over the period 2012-2018-19. If FI were an important contributing factor to anemia, then the crisis recovery would have led to the decrease—not increase—in anemia. Therefore, it is hard to explain the increasing trend in anemia observed in the data. 19 Moreover, data shows that rates of ID are decreasing in all population groups, with ID being the main contributor to anemia due to its role in the synthesis of Hb in the liver and bone marrow.
Although anemia has a multifactorial etiology, non-nutritional causes of anemia at a population level have not been adequately addressed in Mexican surveys. We hypothesized that non-nutritional potential causes would have a low contribution to anemia at the population level; for example, hemoglobinopathies, thalassemia, certain rare autosomal recessive disorders involved in iron homeostasis, parasites, hookworms, and chronic diseases (cancer or autoimmune disorders that lead to functional ID). 1 Although these potential causes have not been measured at the population level, it would be unusual for the trend of these causes to change greatly over 6 years (2012-2018-19).
Functional ID secondary to inflammation can cause iron-refractory anemia. Obesity has shown to be a trigger of the inflammatory pathway affecting iron distribution. 20 Nonetheless, the magnitude of higher CRP concentrations (>5 mg/dL) in Mexican children that could eventually affect iron absorption did not change over the period analyzed. No information of other sensitive biomarkers of inflammation is available as Alpha glycoprotein 1 acid. In fact, past surveys have associated overweight and obesity with lower odds of developing anemia in children and adults 16 ; however, such findings should be interpreted with caution given the lack of sensitive biomarkers and prospective studies needed to understand the role of obesity in anemia incidence. Overweight and obesity have increased in the past years 21 and low-grade chronic inflammation can affect iron absorption and, hence, anemia due to inflammation. 20 It is possible that we are witnessing a shift in the causes of anemia from micronutrient deficiencies to inflammation. Nevertheless, more sensitive indicators of iron homeostasis regulators during inflammation (hepcidin) would help elucidate the diagnoses and address this hypothesis. 22
Noncausal factors linked to anemia could be explained by different reasons. Diverse factors in the preanalytical, analytical, and postanalytical stage can affect Hb measurement, including equipment, material, participant sample, environmental factors, blood sampling techniques, and skill level of study personnel. If not controlled, all these factors may affect the variability of Hb values. 23
Portable photometers are widely acceptable for use in LMIC field settings for logistic and economic reasons. 8 In the 1999 and 2006 ENSANUTs, the B-HemoCue system was used for measurement while from 2012 to 2018-19 the HemoCue 201+ was used. The HemoCue 201+ has been demonstrated as reliable and reproducible. 24 Nevertheless, the lowest prevalence of anemia across all age groups was observed in 2012 using the HemoCue 201+, while the highest prevalence of anemia was observed in 2018 using the same device. So, the use of this device cannot fully explain the Hb variability observed, unless the device was not properly calibrated and verified. It seems that other factors apart from the HemoCue model affected Hb variability. Humidity and temperature can affect the stability of HemoCue cuvettes and electronic performance of the device. 23 We do not know the magnitude of their impact (if any) on Hb variation in past surveys. However, the timing of data collection between surveys was similar (from July to April), particularly in 2006, 2012, and 2018-19. In 2015, the ENIM (a national survey in Mexican children and women) shown a prevalence of anemia of 14.1% in children aged <5 years using HemoCue 201+ and finger-prick blood samples, 25 which contrast with the results found in the ENSANUT 2016.
Another possible explanation for the U-trend is whether or not the samples were biased toward populations at a higher risk of anemia. If the sampling were biased toward populations with an increased risk of anemia, then other nutritional indicators and characteristics associated with this condition would exhibit a similar pattern to anemia, such as malnutrition, micronutrient deficiencies, and FI. This did not occur and these indicators did not reveal a significant increasing trend: stunting (13.6% in 2012 and 14.2% in 2018, P > .05) and wasting (1.6% in 2012 and 1.4% in 2018-19, P > .05) remained constant 26 ; micronutrient deficiencies showed a decrease in vitamin B12, vitamin A, iron, and zinc 16 ; and the proportion of households with moderate to severe FI dropped from 28.2% to 22.7% (P < .001) in the same period. 19 Therefore, it is unlikely that the samples were biased.
Previously, we discussed the factors associated with anemia in the Mexican population, 6,16 finding no associations with socioeconomic or demographic factors; among the variables studied, only ID was minimally associated to anemia in children. Random error in Hb concentration measurement may link to anemia misclassification, which tends to nullify any association of the covariates. In the surveys, Hb was measured through capillary drop blood while iron status, CRP, and other micronutrients were measured through serum (venous blood). Notably, ferritin measurement was done using two different types of equipment (BNproSprc with reagents from Dade Boehringer in 2006, and an Architect CI8200 in 2012-18) in the same laboratory; data were verified and calibrated accordingly.
Most population-based surveys from LMICs use point-of-care devices (portable photometers) to measure Hb and to estimate the prevalence of anemia at the population level using capillary blood. 27 It is well recognized that Hb measurement with venous blood using hemocounters is the gold standard, nonetheless in the field, it is not feasible to maintain in the cold chain (5°C) the whole venous blood sample to transport it to a central laboratory due to long distances, economic and logistic challenges, therefore we use HemoCue. The use of capillary blood samples can render higher anemia misclassification than when using venous blood samples with HemoCue devices. 27 In Mexico, measurement of Hb has been in situ using HemoCue devices and the single capillary drop blood method, which may render a greater variability along with aleatory error.
In a recent study, 28 we documented high random variation of measured Hb values when using capillary blood drop samples taken by personnel with high-performance skills. 28 When using capillary drop blood and the HemoCue 201+, in comparison to venous blood, measurement error was higher in children (17.7%) than in women and older adults, which reflects the challenge in obtaining good quality capillary drop blood samples in this age-group. Measurement error can largely impact those with a mean Hb value near the cutoff value defining anemia, 29 as is the case for children. The lower mean Hb concentration, including its variability, was associated with the higher rate of anemia prevalence observed in 2018-19.
With these considerations, there is a possibility that the estimated anemia prevalence and trend were driven primarily by measurement errors in Hb concentration and other unobserved causes of anemia. The skill of personnel in taking capillary drop blood samples can result in greater variation and higher anemia estimates than when using pooled capillary or venous blood. 30 Along with non-studied causes, measurement error in collecting capillary drop blood may have played a role in the prevalence of anemia measured across surveys. Nevertheless, past surveys did not include validation studies which could have addressed the potential variability in the hemoglobin concentration. Recently, we estimated the prevalence of anemia in Mexico using venous blood in HemoCue 201+ 31 and found that all age groups showed a lower prevalence of anemia using venous blood in comparison with these past surveys that used drops of capillary blood. This finding supports our hypothesis that some measurement error might have affected the estimation of anemia using drops of capillary blood. The series of finger prick measurements performed in the 5 ENSANUT waves were cross-sectional, thus no causality can be claimed.
Further studies should pay more attention to accounting for all the factors potentially associated to variability of Hb concentration and micronutrient deficiencies, and if possible, validate related data to assure precision and quality. This would allow for better anemia estimates and, in addition, better nutritional surveillance that will support targeted health policies to tackle undernutrition: particularly micronutrient deficiencies.
Conclusions
The shifting trend in anemia prevalence across ENSANUT waves from 1999 through 2018-19 did not match the decreasing trend in more sensitive indicators such as ID across the same period of time. Deficiencies of micronutrients associated with hemopoiesis also decreased, and concentrations of the indicator of inflammation CRP did not change significantly; nonetheless, other reliable indicators of inflammation help us to understand whether other causes of anemia are occurring. Other noncausal factors seem to play an important role in the variability of hemoglobin measurements. Future studies should considerer a validation component designed to explain the variability of hemoglobin and its impact on anemia estimates in the study sample.
Footnotes
Authors’ Note
This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study participants were approved by the Ethics in Research Committee at the National Institute of Public Health of Mexico. Written informed consent was obtained from all subjects in each survey.
Author Contributions
Conceptualization, VDlC-G; methodology, VDlC-G, TS-L; formal analysis, VDlC-G; writing—original draft preparation, VDlC-G; writing—review and editing, TS-L, SV; funding acquisition, TS-L. All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This study was funded by the Mexican Ministry of Health. The funder had no role in the design, analysis, or drafting of this article.