
Abstract
Background:
During the COVID-19 pandemic, the world experienced social distancing that resulted in changes in habits and lifestyle. Such changes can compromise healthy eating habits and the practice of physical activities, known risk factors for developing weight gain and obesity.
Objective:
The main objective of this study was to describe the change in eating habits, lifestyle, and cognition of the population of Rio Grande do Sul, a state in Southern Brazil, during social distancing due to COVID-19.
Methods:
The study was conducted from July 21 to August 10, 2020, through a structured online questionnaire that asked for sociodemographic information (age, gender, and education), anthropometric (reported weight and height), change in eating habits, lifestyle (sleep quality and physical activity), and cognition. Chi-square, McNemar tests, and univariate and multivariate analysis were used to evaluate the variables. Confidence intervals were calculated with a significance level of 5%.
Results:
Of a total of 1072 participants, 57.3% of respondents reported weight gain, and an increased percentage of people were classified as obese. Nearly half of the participants (46%) reported changes in their eating habits for the worse. Body mass index (BMI) was significantly associated with increased consumption of unhealthy foods. Our results identified high physical inactivity (46.9%) and obesity (19%) during social distancing. The changes in eating habits and lifestyle also increased the risk for decreased cognition.
Conclusions:
These findings highlighted that social distancing impacted eating habits and lifestyle, which increased obesity rates and might predispose to decreased cognition.
Introduction
The recent outbreak caused by the SARS-CoV-2 virus gave rise to the coronavirus disease (COVID-19) pandemic, which has emerged as a serious public health problem. 1 Since the emergence of this virus in December 2019 through February 2023, there have been more than 757 million confirmed cases of COVID-19 worldwide, including more than 6 million deaths reported to the World Health Organization (WHO). 2 From May 10, 2020, to April 27, 2021, the state of Rio Grande do Sul, situated in the South of Brazil, instituted a system of controlled social distancing to prevent and fight the pandemic. 3
The restrictions on normal daily activities imposed by the pandemic profoundly impacted lifestyle. 4,5 The increase in sedentary lifestyle and the adoption of an unbalanced diet increased obesity rates and predisposed to comorbidities, including cognitive impairment. 6,7 Furthermore, adipose tissue hypertrophy, which occurs in obesity, leads to increased production of pro-inflammatory cytokines and has been related to worse cognitive outcomes. 8,9 Also, unhealthy eating is a factor that negatively affects brain function, 10 but the impacts of lifestyle change caused by the pandemic on adult cognition are not yet known.
Previous studies conducted in different countries provided some data regarding changes in lifestyle during the initial period of the pandemic. A general trend toward adopting less healthy eating habits was shown. 5,11 However, some studies also found a healthier eating pattern. 12,13 In the Brazilian population, these findings are also controversial. 14,15 The socioeconomic differences between the analyzed regions might explain the divergent results. In view of that, it is clear the importance of identifying the factors related to lifestyle changes during social distancing in different populations. Based on these findings, it will be possible to compare the periods before and after the pandemic, as well as to outline public policies aiming to minimize the long-term impact of the pandemic on health. So far, there are no data on the adult population of Southern Brazil. Considering that the environment imposed during social distancing can influence the cognitive decline 7 and these changes can appear long before the onset of clinical signs, 16 it is important to investigate whether the lifestyle during the COVID-19 pandemic, including the eating habits and, consequently the body weight, could be associated with the cognitive status.
Given the above, the main objective of this study was to analyze and describe the changes in eating habits, lifestyle, and cognition during social distancing in the population of Rio Grande do Sul, Brazil.
Materials and Methods
Study Design and Participants
The present study was conducted by researchers from the Laboratory of Behavioral and Metabolic Physiology at the Federal University of Health Sciences of Porto Alegre (UFCSPA), using a web survey to obtain data on eating habits, lifestyle, and cognition of people in the Rio Grande do Sul during the COVID-19 pandemic. This web-based cross-sectional study was conducted using the Google Forms platform. People older than 18 years and residents of Rio Grande do Sul were included in the study.
The sample was calculated expecting a heterogeneous sample in terms of responses (proportion = 50%), with a tolerated error of 3% and confidence in estimates of 95%, resulting in 1068 participants. This calculation was performed using the PSS Health tool online version. 17 To this value, 20% was added to the sampling to avoid possible losses or duplication of responses. After reaching the estimated number of responses, the online questionnaire was closed. The survey began on July 21 and ended on August 10, 2020. At this time, the state of Rio Grande do Sul was experiencing a period of social distancing following a local governmental decree. 3
Survey Questionnaire
The questionnaire comprised 42 questions about lifestyle changes: eating habits, self-perception of sleep quality, physical activities, and cognition before and during the COVID-19 pandemic (Supplementary material S1). The survey was divulgated and distributed by email and private social networks (WhatsApp, Facebook, and Instagram) through an access link. The questionnaire was designed and structured in Google Forms and divided into four sections: (1) sociodemographic data (age, gender, education, city of residence); (2) anthropometrics information (reported weight and height); (3) lifestyle, food consumption, changes in eating habits, self-perception of sleep quality, and physical activities before and during isolation; and (4) cognitive aspects were investigated using questions from validated instruments, as described below, to investigate cognitive impairment before and during the pandemic.
Before participants accessed the questionnaire, information about the study, such as objectives and the research ethics, was presented, followed by the consent form. The questionnaire was answered anonymously. Some questions were designed to determine whether participants increased, reduced, or maintained their habits during the pandemic. Other questions were related to the answers “before” and “during” the social distancing. It was also asked about the consumption of certain foods in the last 24 hours (such as fruits, vegetables, and water). In addition, the participants were asked if they perceived that their eating habits, physical activity, and body weight had changed since the beginning of social distancing.
The last research session consisted of 06 questions taken from the validated questionnaires Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE-SBr) 18 and Montreal Cognitive Assessment (MoCA). 19 These instruments are commonly used in clinical assessment of cognitive decline. Based on the scores of the cognition and memory tests, a cognitive score was created, defined as the sum of the 3 memory questions and the 3 cognition questions, scored as follows: 0 point for little change, 1 point for a little better, 2 points for much better, −1 point for a little worse, −2 points for much worse for the memory questions, and 1 point for correct and −1 point for incorrect each cognition question. The median value obtained from the whole sample was 3. Thus, low cognition was defined by scores below the median score (3 points). The analyzed outcomes were presence of obesity (body mass index [BMI] ≥30 kg/m2) and low cognition (worse cognition).
Ethical Aspects
The study was conducted following the Declaration of Helsinki (2000). 20 It was approved by the Research Ethics Committee of the Federal University of Health Sciences of Porto Alegre (approval number #4,166,026). Participants were informed about the study’s objectives and were asked to accept data sharing and privacy policies before participating.
Statistical Analysis
The Shapiro-Wilk test was performed to evaluate normal distribution of the data. Body weight and BMI before and during the pandemic were compared using paired 2-tailed Student t test and are described as mean ± standard deviation. The sample was described as absolute and relative frequencies. Chi-square was run for heterogeneity or linear trend, according to the nature of the variables. Frequency of physical activity was analyzed using McNemar test. In addition, 95% confidence intervals were calculated, and the level of significance considered was 5%.
Univariate and multivariate analyses were performed considering gender, age, education, physical activity, sleep change, and eating habits as the exposure variables, while obesity and cognition were the outcome variables. The associations of the variables with the obesity and low cognition outcomes were verified by Poisson regression analysis with robust adjustment of variance, where measures of relative risk (RR) effect size with 95% confidence interval (CI) were obtained in the univariate and multivariate stages. Analyses were performed using Statistical Package for the Social Sciences (SPSS) 25.0, Stata 16.1 and GraphPad Prism 8 were used for all statistical analyses.
Results
Participants
A total of 1217 participants completed the questionnaire, and after data validation, 1072 respondents aged between 18 and 83 years were included in the study. The female respondents represented 76.4% of the population. The level of education of the majority of the respondents was postgraduate (49.4%). General characteristics and anthropometrics of the population are reported in Table 1. Regarding the BMI, 48.4% of the participants reported normal weight at the time of the survey, but 49.6% of the sample were overweight or obese (BMI ≥ 25 kg/m2).
General and Anthropometric Characteristics of Participants During the COVID-19 Pandemic.a
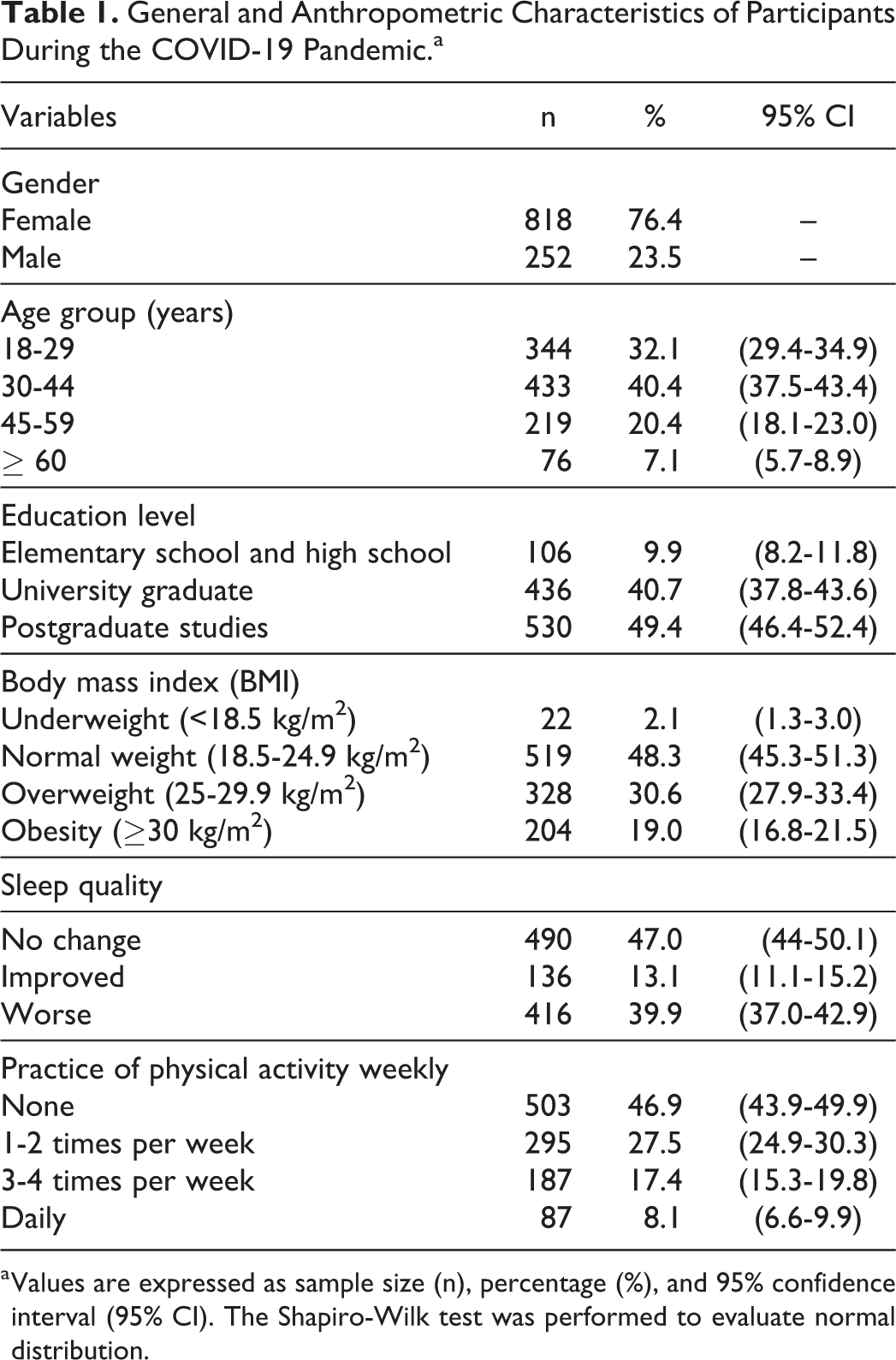
a Values are expressed as sample size (n), percentage (%), and 95% confidence interval (95% CI). The Shapiro-Wilk test was performed to evaluate normal distribution.
The sample’s average body weight significantly increased during social distancing (P < .0001, t = 12.65) from 70.1 ± 15.7 kg before distancing to 71.6 ± 16.3 kg during this period (Figure 1A), as well as the BMI of the participants (P = .0124, t = 2.502; Figure 1B). The BMI classification (Figure 1C) showed that 14.5% of the participants were obese before the social distancing, and the obesity percentage increased to 19% during the distancing.
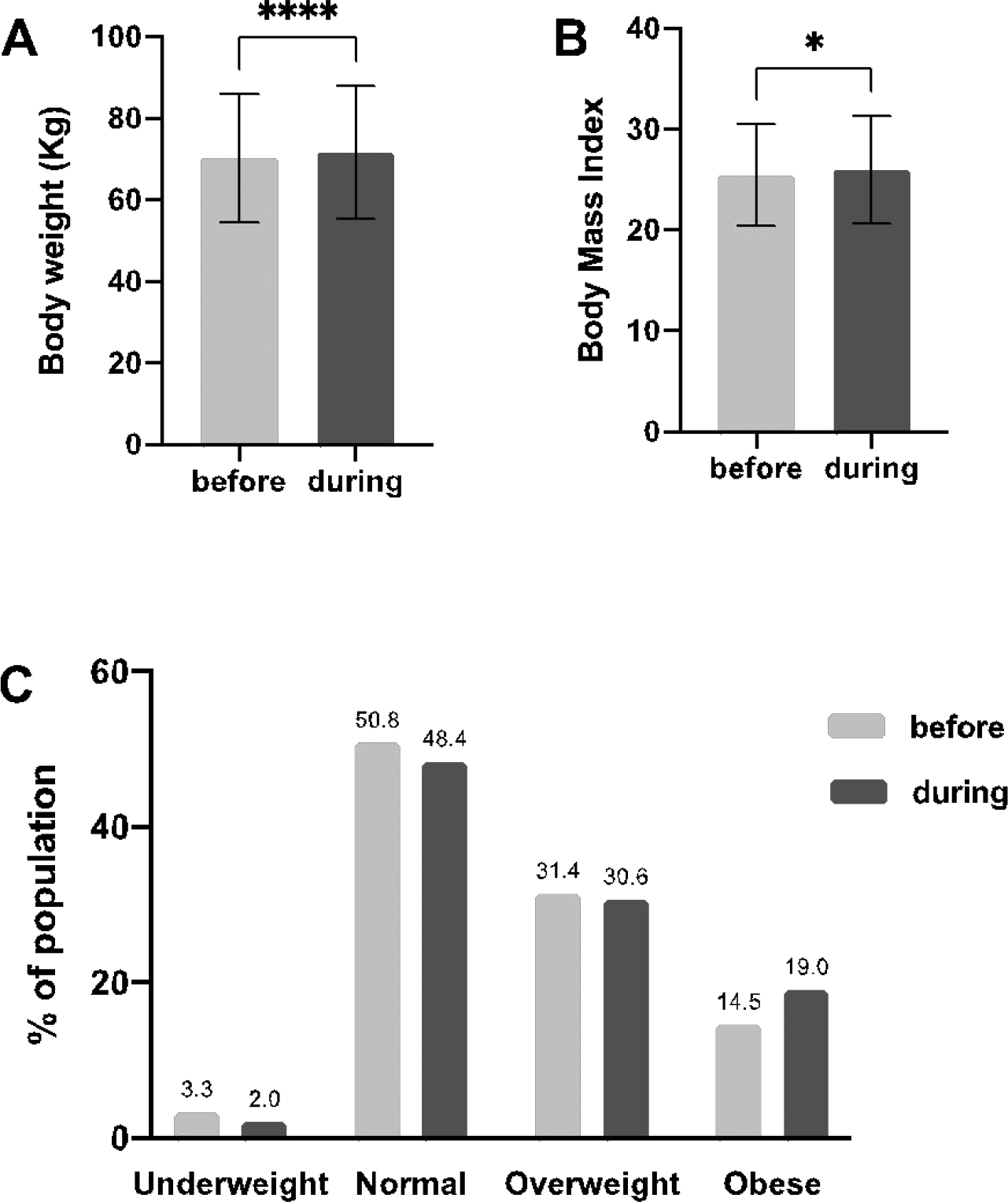
Body weight and body mass index (BMI) of the participants evaluated before and during social isolation. Average body weight (A), average BMI of the entire population (B), percentage change in the BMI classification (C). *P < .05;***P < .0001 (Student t test).
Eating Habits Changes During COVID-19 Social Distancing
In the survey, we asked if the consumption of certain types of foods changed during social distancing. The participants mentioned a high consumption of junk food, including sweets, industrialized food, and fried foods. Table 2 shows the association between the increase in food consumption according to age, gender, level of education, and BMI. According to age, there was a significant increase in the intake of fried foods and sugary drinks, with a higher percentage of change among participants aged 60 years or older. However, all age groups showed high consumption of all types of foods.
Increase in Food Consumption During the COVID-19 Pandemic Among Brazilian Adults According to Sociodemographic Characteristics and BMI.
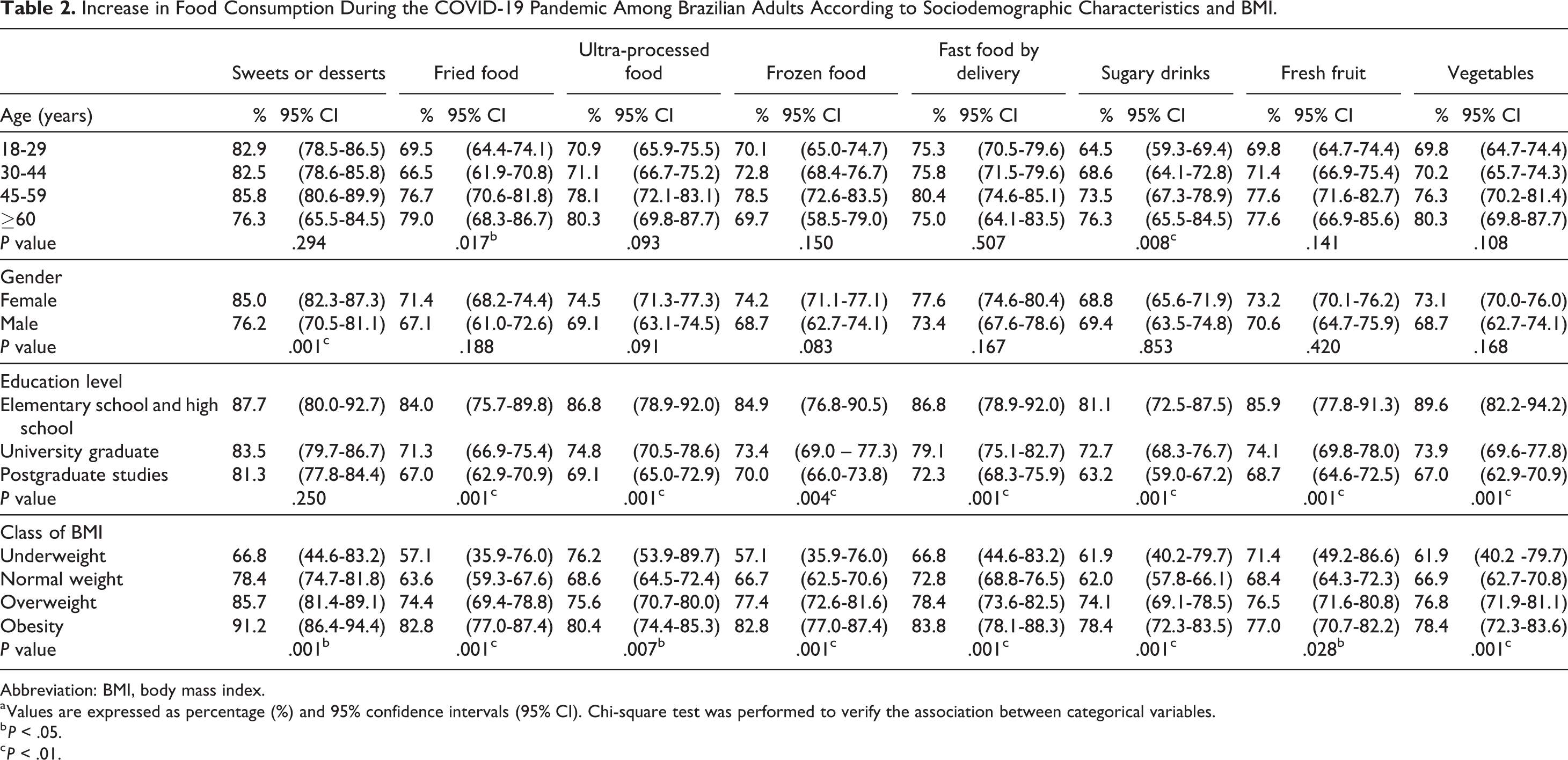
Abbreviation: BMI, body mass index.
a Values are expressed as percentage (%) and 95% confidence intervals (95% CI). Chi-square test was performed to verify the association between categorical variables.
b P < .05.
c P < .01.
There was a significant increase in the consumption of sweets and desserts, in both genders, with the highest percentage of change in women (85%). The change was greater in females, except for sugary drinks. We did not observe a significant change in the intake of fresh fruits and vegetables and homemade food consumption between gender or age groups. There was a significant change in all foods investigated according to education level, except for sweets and desserts. In addition, it was found that a lower level of education was associated with a higher percentage of change in the consumption of fried foods, processed foods, frozen foods, fast food via delivery, sugary drinks, fresh fruits, vegetables, and homemade food. According to the BMI classification, overall consumption increased in all groups. The highest percentage of increase was shown in people with obesity. As for food consumption of fresh fruits and vegetables the day before, the results show low consumption of fruits during social distancing; only 16.6% of people ate the portion recommended by the WHO during COVID-19. 21 Regarding the consumption of vegetables, 51.4% responded to eating 2 or more portions a day during COVID-19 (Supplementary Table S2).
We also performed univariate analysis to evaluate which factors were associated with obesity (Table 3). The factors associated with the risk of developing obesity were sedentary lifestyle (P = .011), worsening sleep quality (P = .034), change in sweets consumption (reduction P = .006; increase P = .001), change in fried food consumption (reduction P = .016; increase P < .001), increase in ultra-processed foods consumption (P = .002), increase in fast food via delivery (P = .003), increase sugary drinks consumption (P < .001), and increased vegetables consumption (P = .029). When we performed the multivariate regression analysis with adjusted residuals, we found that factors such as physical inactivity (P = .019), increased fried foods consumption (P = .013), and change in sweets consumption (P = .039) remained risk factors associated with obesity during the COVID-19 pandemic. In addition, young people (18–29 years old) had the lowest risk of developing obesity (P = .010).
Factors Associated With Obesity During the COVID-19 Pandemic.
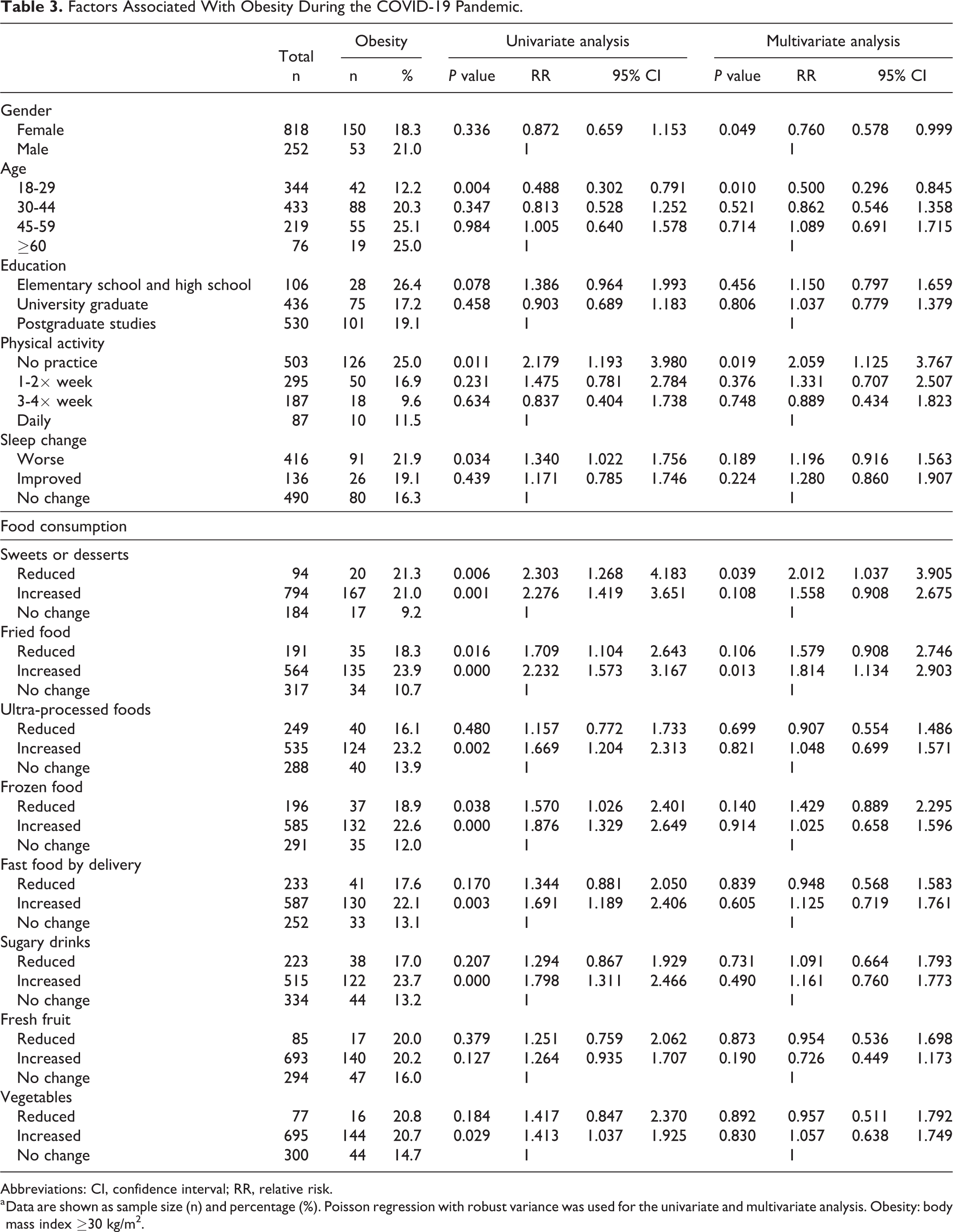
Abbreviations: CI, confidence interval; RR, relative risk.
a Data are shown as sample size (n) and percentage (%). Poisson regression with robust variance was used for the univariate and multivariate analysis. Obesity: body mass index ≥30 kg/m2.
Physical Activity During Social Distancing
Regarding the practice of physical activities, 70.4% of the participants reported performing some level of physical activity (from 1 to 7 days a week) before the pandemic. However, this percentage decreased to 53.1% during social distancing. In addition, the percentage of people who did not practice physical activities before the pandemic increased from 29.6% to 46.9% during the pandemic. These results showed reduced physical activity during social distancing imposed by COVID-19. Data on the weekly frequency of physical activity before and during the pandemic are shown in Table 4.
Frequency of Physical Activity Before and During the Social Distancing Imposed by COVID-19 Pandemic.a
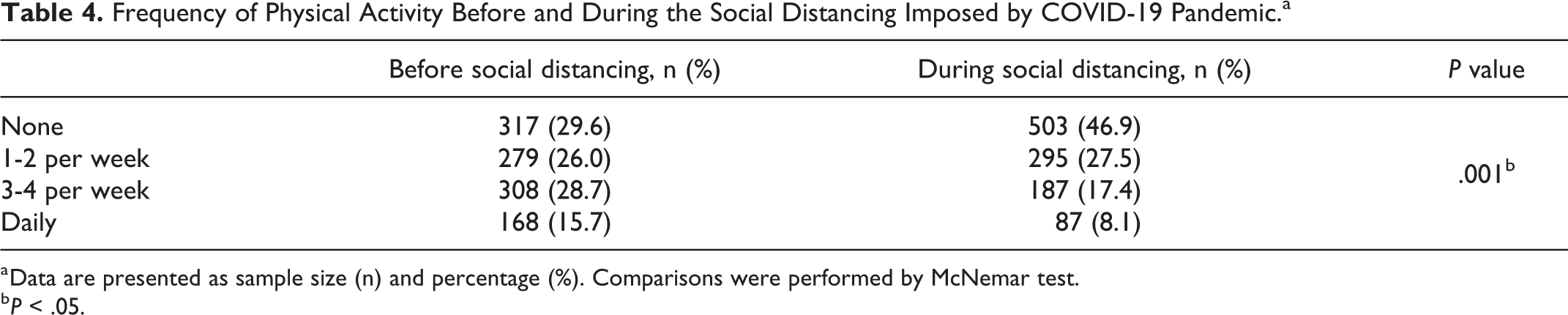
a Data are presented as sample size (n) and percentage (%). Comparisons were performed by McNemar test.
b P < .05.
Cognition
A cognitive score was calculated based on the answers to the memory and cognition questions. As described in “Methods” section, people with a score below 3 were considered to have a low cognitive score. Then, we investigated the risk factors associated with the low cognitive score (Table 5). Univariate analysis showed that women (P < .001), undergraduate educational level (compared to postgraduate, P = .021), low weight (compared to normal weight, P = .048), sedentary lifestyle (P = .005), poor sleep quality (P < .001), reduction in fast food (P = .036), fruit (P = .002), and vegetables (P = .031) consumption were risk factors for worsened cognition. The adjusted multivariate analysis showed that factors such as female gender (P < .001), not practicing physical activity and doing it 3 to 4 times (compared to doing it daily, P = .024), poor sleep quality (P < .001), increased consumption of frozen foods (P < .028), and reduced consumption of fast food remained risk factors for a low cognitive score.
Factors Associated With Low Cognition During the COVID-19 Pandemic.a
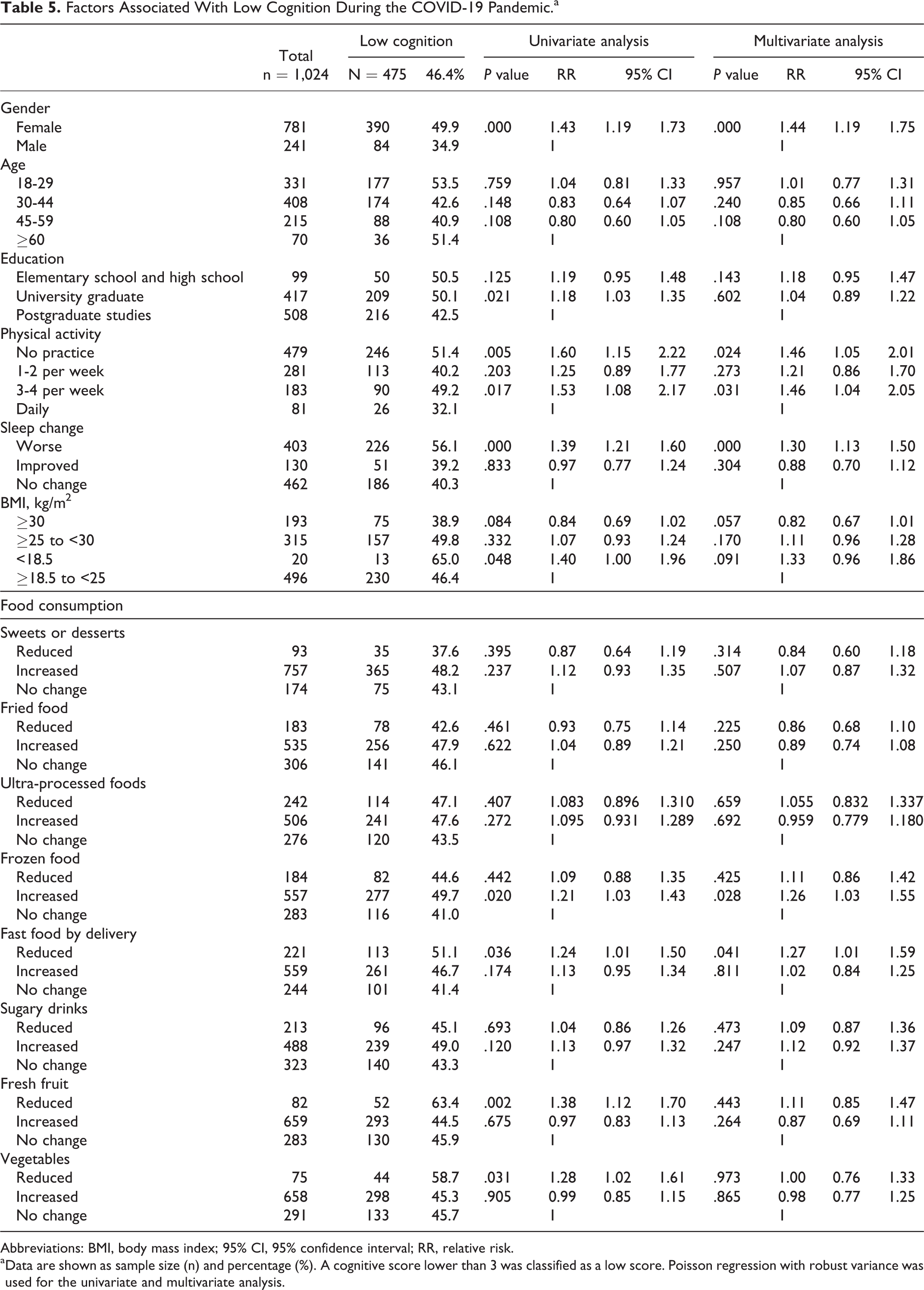
Abbreviations: BMI, body mass index; 95% CI, 95% confidence interval; RR, relative risk.
a Data are shown as sample size (n) and percentage (%). A cognitive score lower than 3 was classified as a low score. Poisson regression with robust variance was used for the univariate and multivariate analysis.
Discussion
This study was the first to investigate adults’ eating habits, lifestyle, and cognition from Rio Grande do Sul, the Southern state of Brazil, during social distancing due to COVID-19. The social distancing rules imposed by the local government reduced the spread of the disease. However, these restrictions caused changes in the lifestyle of the studied population. In the present study, most of the sample were young adults (40.4%), mainly women (76.4%). The greater participation of women has already been evidenced in other studies on lifestyle during the COVID-19 pandemic. 5,22
Our research also explored the perception of change in body weight. Here, we showed a significant increase in average body weight during social distancing compared to prepandemic weight. Consistently, this weight gain is reflected in an increase in average BMI. Similar results were found in Spain and Italy, where 52.7% and 48.6% of the participants reported increased body weight, respectively. 5,13 These findings demonstrated that during the initial period of social distancing, there was a body weight gain in different populations. The present study highlighted the increase in obesity from 14% to 19% of the population. The increase in obesity during the COVID-19 pandemic was also shown elsewhere. 23
Social distancing due to the COVID-19 pandemic has led to significant changes in food consumption. In the present study, most participants (46%) responded that their diet had worsened. On the other hand, in an Italian study, 46% of the participants answered that they had not changed their eating habits during the initial period of the pandemic. 5 In the same period, a study carried out in Spain showed that healthier eating habits were adopted. 21 Our study showed that females had the highest percentage of change in food consumption, except for sugary drinks. Differences between the sexes in the behavior regarding food choices, especially for sugary foods, have already been described previously. 24 Here, women showed an increase in the consumption of sweets and desserts, similar to the findings of another study. 22 We showed that almost one-third of participants (29.8%) reported eating sweets or desserts daily. The daily consumption of sweets might be related to the increase in stress and anxiety resulting from social distancing since the intake of carbohydrates is related to well-being and emotional comfort. 25 However, it is widely known that excessive intake of sweets increases the risk of developing overweight and obesity, among other diseases. 26 According to the WHO, the recommendation is that less than 5% of the total caloric intake of adults should come from free sugars. Also, it is recommended to replace sweets and added sugars with fresh fruit. 27
In Brazil, previous studies have shown conflicting results regarding consuming fruits and vegetables during the pandemic. 14,15 These divergences might indicate that the changes in eating habits depend on the socioeconomic status of the studied population. Decreased consumption of fruits and vegetables is worrying since these foods provide the necessary micronutrients to the body, strengthening the immune system; therefore, it is a protective factor for preventing chronic diseases. In addition, fruits usually consumed by the Brazilian population, such as bananas, avocados, and pineapples, and vegetables and tubers such as cauliflower, broccoli, potatoes, beets, and peas are rich in nutrients such as tryptophan, which is a precursor of serotonin, which in turn is involved in the regulation of satiety and energy intake. 28 On the other hand, low micronutrient intake negatively affects the immune response. Therefore, a varied and balanced nutritional pattern, with adequate intake of vitamins and minerals, such as vitamins C, D, E, and β-carotene and zinc, is especially important during a pandemic. 29
Our study showed an increase in overweight during social distancing due to the pandemic. Recent data estimate that around 2.1 billion people are overweight or obese in the world. 30 Although obesity is a multifactorial disease, the COVID-19 pandemic has increased its prevalence, as shown by our study and others. 13,23 These results reflect the obesogenic environment created during the pandemic: the excessive consumption of ultra-processed, accessible, tasty, and energy-rich foods, combined with an increased sedentary lifestyle.
An important point raised by our study is that we showed that this environment imposed by the pandemic had a negative impact on body weight, BMI, eating habits, and physical activity level. Together, these factors influence cognition. 31 In addition, we showed that factors such as worsening sleep quality, increased consumption of frozen industrialized foods, and not practicing physical exercise increase the risk of a low cognitive score. Although it is already established in the literature that these factors can influence cognitive decline in different age groups, 7 to the best of our knowledge, this is the first study to demonstrate that these factors increase the risk of decreasing cognitive performance in the context of the COVID-19 pandemic. Given that factors such as worse eating habits, poor sleep quality, and a sedentary lifestyle have intensified during the pandemic, further studies are important to investigate the long-term consequences on cognition. The relationship between obesity and cognitive decline is based on the exacerbated inflammatory status of the adipose tissue, which generates a systemic dysfunction. The brain is also susceptible to such dysfunction, as demonstrated by the neuroinflammation caused by obesity, which triggers cognitive impairment. 9
Another consequence of social distancing was a decrease in physical exercise. The high rate of physical inactivity found here was in line with other studies in different countries. 32,33 We also showed that the decrease in the weekly frequency of physical exercise is a risk factor for both obesity and impaired cognition, highlighting the negative impact of physical inactivity on health. It is widely known that physical inactivity is also a risk factor for chronic noncommunicable diseases such as coronary heart disease, type 2 diabetes, and cancer. 34 This scenario emphasizes the importance of our study in supporting Brazilian public health policies aiming to diminish sedentarism as a way to improve health.
Nevertheless, the findings presented here should be interpreted within their limitations, as it is a cross-sectional study with a representative but a random sample. Any observed associations may not represent a cause-and-effect relationship in the general population. It is important to recognize that self-reported responses may be subject to reporting bias. However, self-reported weight and height are already validated for the Brazilian population. 35 Another study limitation is that the questionnaire is not a validated instrument. However, in the context of a pandemic, online research was a viable, simple, and fast approach to exploring the Southern Brazilian population’s eating habits, lifestyle, and cognition. Despite these limitations, future studies would benefit from investigating strategies to minimize the consequences reported here.
Conclusion
The present study showed that social distancing imposed by the COVID-19 pandemic caused a harmful effect on eating habits and lifestyle, which was associated with weight gain and increased risk of impairing cognition. These findings can contribute to formulating policies in response to the consequences of the pandemic on the health of the Southern Brazilian population.
Supplemental Material
Supplemental Material, sj-pdf-1-fnb-10.1177_03795721231172369 - Weight Gain, Lifestyle, and Cognition During the COVID-19 Pandemic in Southern Brazil
Supplemental Material, sj-pdf-1-fnb-10.1177_03795721231172369 for Weight Gain, Lifestyle, and Cognition During the COVID-19 Pandemic in Southern Brazil by Liziane da Silva de Vargas, Jeferson Jantsch, Ana Paula Muterle Varela, Gilson Pires Dorneles, Roberta de Vargas Zanini, Alessandra Peres and Renata Padilha Guedes in Food and Nutrition Bulletin
Supplemental Material
Supplemental Material, sj-pdf-2-fnb-10.1177_03795721231172369 - Weight Gain, Lifestyle, and Cognition During the COVID-19 Pandemic in Southern Brazil
Supplemental Material, sj-pdf-2-fnb-10.1177_03795721231172369 for Weight Gain, Lifestyle, and Cognition During the COVID-19 Pandemic in Southern Brazil by Liziane da Silva de Vargas, Jeferson Jantsch, Ana Paula Muterle Varela, Gilson Pires Dorneles, Roberta de Vargas Zanini, Alessandra Peres and Renata Padilha Guedes in Food and Nutrition Bulletin
Footnotes
Acknowledgments
The authors thank the Support Center for Research of UFCSPA and Cristiane Bündchen for assisting us with the statistical analysis.
Authors’ Contributions
LV conceptualized the study, collected and analyzed the data, and wrote the manuscript. JJ analyzed the data and critically reviewed the manuscript. APV critically reviewed the manuscript. GD and RZ validated and analyzed the data. AP critically reviewed the manuscript and supervised the study. RG provided resources, designed the graph, critically reviewed the manuscript, and supervised the study. The authors read and approved the final manuscript.
Data Availability Statement
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
This study was approved by the Human Research Ethics Committee of the Federal University of Health Sciences of Porto Alegre (CAAE protocol no. 33892720.7.0000.5345).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.