
Abstract
Background:
Fortification of rice with slaked lime is an acceptable and inexpensive way to combat calcium (Ca) deficiency. However, bioavailability of calcium after intake of slaked lime fortified rice is yet to be investigated.
Objective:
To measure the fractional absorption of Ca (FAC) from slaked lime fortified cooked rice.
Design:
We conducted an experimental study using stable isotopes of Ca to measure FAC during a single morning test meal containing rice fortified with slaked lime. Participants (n = 22) were given slaked lime fortified rice 3 times a day for 4 days. On the morning of the fifth day, the participants were served the same amount of rice as previous the 4 days at the breakfast test meal with an accurately measured amount of 44Ca stable isotope oral tracer followed by an intravenous injection of 42Ca. Urine was collected over the next 24 hours in 3 consecutive 8-hour pools. Fractional absorption of Ca was calculated from the measurement of the relative enrichment of the of each administered tracer 44Ca and 42Ca using inductively coupled plasma mass spectrometry.
Results:
The mean Ca concentration in the test meal was 879.5 ± 152.9 µg/g with a coefficient of variance (CV) of 17.2%. Although Ca absorption efficiency decreases with higher calcium intake, the total amount of calcium absorbed from test meal using FAC = 0.391 calculated from the third 8-hour urine pool was 69.0 (CV of 15.6) mg.
Conclusions:
We showed that one-fifth of daily calcium recommendation for women of reproductive age could be met by ingesting ∼200 g cooked slake fortified rice.
Keywords
Introduction
Diet of the Bangladeshi population lacks calcium which results in calcium deficiency. This nutritional compromise is associated with hypertension and eclampsia during pregnancy—a dreadful condition that affects thousands of women in Bangladesh. 1,2 Calcium deficiency among these populations poses a dire threat, contributing to rickets in children, impaired attainment of bone mass during skeletal development in adolescents, and osteoporosis and osteopenia in adults. Calcium deficient pregnant women have an increased risk of hypertensive disorders of pregnancy, intrauterine growth restriction, preterm birth and are more likely to endow their offspring with low calcium storage, initiating a vicious cycle that results in intragenerational and intergenerational effects. 3 Gestational hypertensive disorders, namely preeclampsia and eclampsia, accounts for 24% of all maternal deaths and 2.8% of all deaths in women of reproductive age in Bangladesh. 4 The World Health Organization (WHO) recommends calcium supplementation during pregnancy in calcium-deficient populations. 5 However, the high cost of calcium carbonate tablets renders calcium supplementation in Bangladesh almost impossible. Since calcium-containing foods are also prohibitively expensive for the general population, we have found that fortification of the staple cereal, rice, is an attractive alternative.
In the southern region of Bangladesh, Cox’s Bazar and Chittagong, there is a high prevalence of calcium deficiency, evidenced by the prevalence of calcium-dependent rickets being as high as 2% among children aged below 15 years. 6 During cooking, the use of slaked lime to fortify rice is a common practice in that region. In 2007, a study was conducted to assess the effectiveness of increased dietary intake of calcium in curing mild lower leg deformity in active rickets. In that study, parents of rachitic children were advised to increase calcium intake by fortifying rice using slaked lime, and by increasing consumption of various calcium-rich foods, radiographic improvement was seen in 90% of the affected children. 7 Therefore, there is evidence from the community that slaked lime fortified rice intake improves calcium nutriture. A systematic review has also been published to inform the design of an effective national calcium program. 3 Subsequently, an experimental study was conducted where very good acceptability of slaked lime fortified rice among women and children was found. In that study, calcium content of rice cooked with different concentrations of slaked lime was given, and then the acceptability of fortified rice among women and children was assessed. Results showed that rice’s calcium content increased in a dose-response manner with an increase in slaked lime amount during cooking. Both groups reported the highest overall acceptability. 8
Staple food fortification seems to be a promising way to combat nutrition deficiency. In South-East Asia, rice is the most widely consumed staple food, with daily rice intake being the highest in the world. 3 The picture is also common in Bangladesh, where people consume rice 2 to 3 times a day. In Bangladesh, rice is an essential source of energy and other nutrients for a majority of the population. It has been shown that rice fortification by the addition of calcium from slaked lime during cooking increased the total amount of calcium available for absorption. 8 In addition, per capita rice consumption in Bangladesh is > 300 g/day (> 110 kg per capita annually). 9 This study showed that the most acceptable fortification level (7.5 g lime/500 g uncooked rice) yielded 1.18 g elemental calcium per 500 g uncooked rice, which means that it can be a feasible solution to the problem of calcium deficiency in this setting. 8 In this way, we can get ∼0.236 g elemental calcium/100 g uncooked rice (300 g cooked rice is equivalent to 100 g uncooked rice) at 7.5 g lime concentration. This can contribute to about half of the recommended calcium intake. 8
However, the actual absorption or “bioavailability” of calcium after intake of slaked lime fortified rice is yet to be investigated. It is already evident that traditional fortification of tortillas with lime increases blood calcium level among Mexican women and has been implicated in reducing the incidence of preeclampsia among the indigenous Maya of Guatemala. 10,11 Considering that consumption of lime fortified rice would increase blood calcium levels, as would hopefully be evident from this bioavailability study, we will establish a solid foundation for an inexpensive and effective intervention.
As slaked lime is inexpensive and accessible and has already been found to be acceptable by women and children through our earlier study, it could be an innovative way to reduce dietary calcium deficiency. Therefore, the aim of our study was to measure the fractional absorption of calcium (FAC) from a test meal of slaked lime fortified cooked rice.
Subjects and Methods
Subjects
Study participants were identified from urban/periurban areas of Dhaka city. All participants were informed about the study and provided informed consent. The project was approved by the Institutional Review Board, icddr, b and the Colorado Multi-Institutional Review Board.
A total of 22 participants completed the study (in studies of bioavailability already published, a sample size of 22 is considered optimum in view of the intensive nature of the study as well as cost of the procedures including the stable isotopes).
We enrolled nonpregnant, nonlactating (NPNL), nonmenstruating healthy women aged 18 to 45 years and body mass index (BMI) 18.5 to 24.9. We excluded those women who were habitual betel nut chewers with lime, severely anemic (Hb% less than 7 g/dL, assessed by HemoCue®) and reported use of dietary supplements that contain > 500 mg of calcium per day and/or use of > 400 IU (10 µg) of vitamin D per day in the last 6 months.
Experimental design
The dual-tracer isotope technique was used to measure calcium absorption (Figure 1). Participants stayed in the study ward of Dhaka Hospital, icddr, b for the duration of the study. On the day of enrollment, anthropometry and socioeconomic status were collected. Then, a baseline serum sample was collected to measure serum calcium, albumin, parathyroid hormone (PTH), and vitamin D. Participants were given slaked lime fortified rice (200 g, cooked) along with lentil soup (70 g) and fried papaya (82 g) 3 times a day for 4 days. Only foods containing a minimal amount of calcium were provided as snacks 2 times a day.
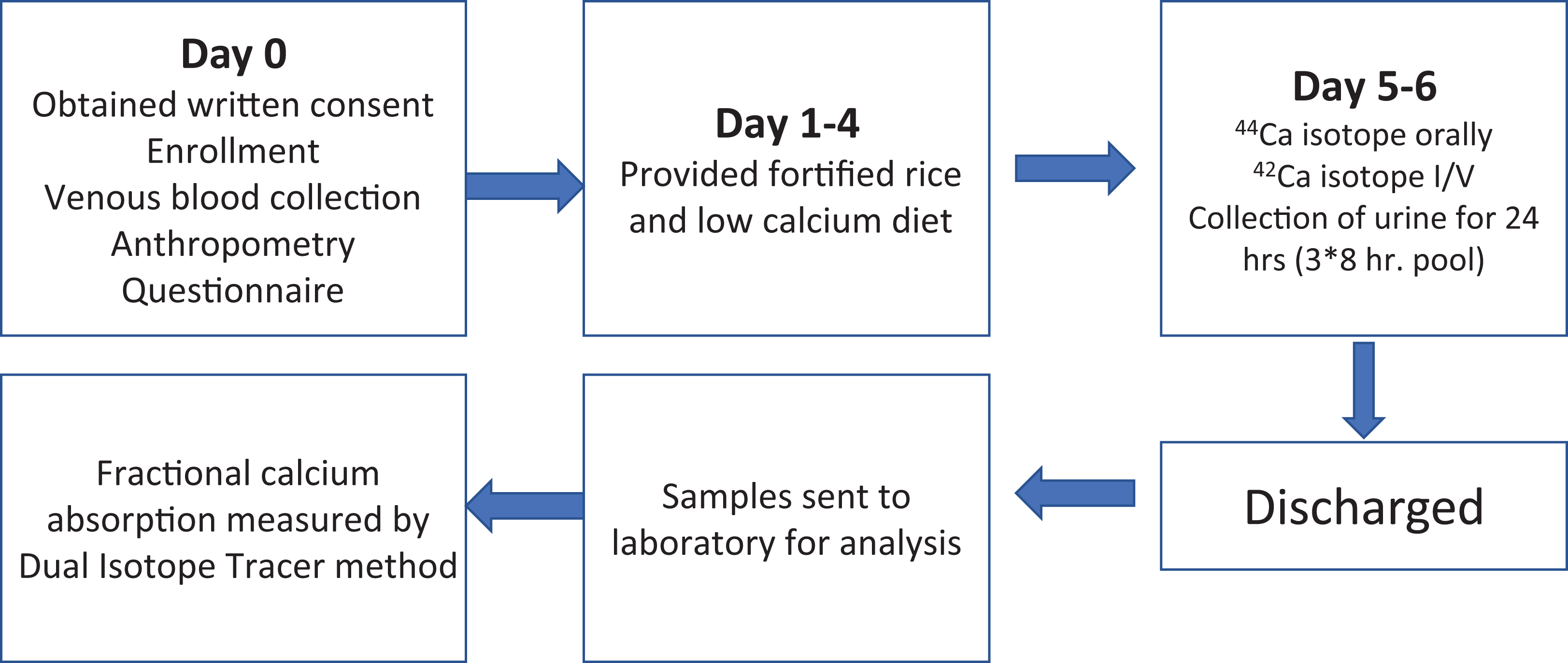
Study design: On the day of enrolment, sociodemographic information, anthropometry, and venous blood were taken. Test meal was given 3 times a day for 4 days and on day 5 isotopes were administered orally with a test meal and intravenously after breakfast; 24 hours (in 3 subsequent 8-hr pools) urine was also collected and sent to University of Colorado School of Medicine for analysis.
Provided food, intake, and leftover were measured using a structured questionnaire in the study ward under the direct supervision of trained Research Assistants to make sure that participants had the controlled diets only.
Several known bottled mineral water brands in Bangladesh were tested for calcium content in Environmental Laboratory, icddr, b. We used only the particular brand that contains calcium less 1 mg/dL. We used this water for washing, cooking, and drinking during the study period.
Participants were requested on the fourth day not to take any food after dinner till the next breakfast (on the day of isotope administration). On the morning of the fifth day, the participants were served the exact amount of rice as previous 4 days as breakfast and oral stable isotope of 44Ca, which was prepared at the Pediatric Nutrition Laboratory, University of Colorado School of Medicine, Aurora, CO, United States. After 15 to 30 minutes, each participant received an intravenous (IV) approved injection of 42Ca over 5 minutes by a trained study physician. Following completion of oral isotope administration, all urine was collected in three consecutive 8-hr pools for 24 hours.
Laboratory Methods
Preparation and Administration of isotopes
Preparation of intravenous and oral isotope doses
Enriched 42Ca and 44Ca stable isotopes were obtained from Trace Science International Inc. (Ontario, Canada) as carbonate. Enriched 44Ca was used as the oral tracer and 42Ca as the intravenous (IV) tracer. Calcium carbonate was dissolved by adding drops of concentrated hydrochloride acid to the powder. Oral solution was diluted to 2.5 g elemental calcium/L with Milli-Q triply deionized water and IV solution at 0.4 g calcium/L with 0.45% sterile NaCl. Oral and IV solutions were adjusted to pH 5.0 and 6.0, respectively, with NaOH.
Using sterile techniques and in a biosafety cabinet, the desired amount of IV and oral isotope solutions were filtered through a 0.2 micron into new sterile containers. Calcium concentrations of these solutions were determined by atomic absorption spectrophotometry with correction factor for atomic weight of the isotopes applied.
The desired amounts of IV dose solution were directly transferred into individual sterile 10 mL vials using a sterile syringe and oral dose solutions were directly transferred into individual 11 mL plastic test tubes using an air displacement pipette. Dispensed doses were weighed to the nearest mg and the amount of isotope in each dose was calculated by multiplying weight by concentration of solution. Randomly selected individual IV and oral doses were sent for fungal, sterility, and pyrogen testing. Pyrogen testing was performed at the adult CTRC of University of Colorado Hospital (UCH) and aerobic and non-aerobic sterility and fungal cultures in the Central Lab at UCH.
Administration of Isotopes
After removing the isotopes from the refrigerator, they were placed at the study ward at room temperature for administration in the morning (day 5). After emptying the bladder, the participant began eating breakfast. While was halfway through it, she was given an accurately measured dose of ~25 mg 44Ca as an oral isotope solution throughout the remainder of the meal. A filter paper was kept under her chin, and another held in research assistant’s hand to collect any isotope dose losses during administration. Any losses were analyzed in the lab and subtracted from the amount of dose administered to arrive at the final dose amount given.
After a minimum interval of 15 mins, a prepared syringe containing an accurately measured dose of ~5 mg 42Ca isotope was administered into participant's antecubital vein through a secured winged cannula slowly over 10 minutes followed by 2 × 5 mL normal saline rinses in a natural pace. As with the oral dose, any dose losses occurring during administration were collected and analyzed All steps were done under aseptic precautions. There were no adverse events reported during the study period.
Collection, storage, and shipment of slaked lime fortified rice and urine sample
While preparing the rice on the fourth day for 3 meals of the next day (day 5—breakfast, lunch, and dinner), 3 fortified, cooked rice samples were taken in 3 preweighed 60 mL Nalgene containers to measure calcium content and calculated intake of Ca from the test meal.
On the day of oral isotope administration, one baseline spot urine was collected before breakfast. Then the participant urinated directly into the clean urine hat for the next 24 hours. The 24 hour urine collections were pooled in three 8-hr aliquots. All the samples were stored in the −20 °C freezer until shipment.
Upon completion of the sample collection from all of the participants, rice samples, dose losses (during administration), and urine samples were shipped to the Pediatric Nutrition Laboratory of CU Anschutz Medical Campus (University of Colorado) for subsequent sample analysis. All the samples were packaged to be compliant with the regulations for shipping “Exempt Human Specimens” and then shipped to the United States.
Preparation of slaked lime fortified rice, lentil soup, and fried green papaya
Five hundred grams samples of milled, parboiled Miniket rice (the most commonly consumed variety in Bangladesh) were washed and cooked in 750 mL water using a Teflon-coated electric rice cooker (NOVA RC-1501 NOVA, Mumbai, India) at the Food Laboratory of icddr, b Dhaka. To each uncooked 500 g rice sample, 7.5 g slaked lime from a single batch from a local market in the Cox’s Bazar district was added. This specific amount (7.5 g) was used as this amount has been culturally accepted by women and children in a very recent experimental study in Bangladesh. 8
Lentil and fried green papaya were purchased from the local market in a single batch. After washing and rinsing, vegetables and lentils were cooked with garlic, ginger, turmeric, salt, oil, and water and then served.
Ethical Consideration
Ethical approval was obtained from the icddr, b’s Institutional Review Board (PR 19059) and the Colorado Multiple Institutional Review Board. The research staff explained the study procedures verbally, and written informed consent was obtained from each participant before the study. Isotopes were administered by the physicians only. The participants were also stringently monitored (blood pressure and pulse rate) during and for the next 30 minutes of isotope administration for any adverse reaction.
Data Analysis
Isotope analysis and calculations
Calcium isotopes ratios were measured using inductively coupled plasma mass spectrometry (ICP-MS, Agilent 7700x, Santa Clara, CA, USA). The ratio of each administered tracer to 46Ca was measured and enrichment (defined as the amount of the tracer over total amount of Ca) was calculated.
Fractional absorption of calcium (FAC) was determined as the relative recovery of the oral and the IV tracer in each 8-hour pool of the 24-hour urine collection. To calculate the absolute amount of Ca absorbed from the test meal (true calcium absorption, TCA), we multiplied the amount of Ca in the meal by FAC.
Statistical analyses
Data were analyzed by using SPSS version 20.0 software. Continuous variables were examined for normal distribution.
Results
A total of 22 healthy, NPNL and nonmenstruating women were enrolled in this study. The mean (± standard deviation [SD]) age, weight, and height of the 22 women were 26 ± 6.7 years (range: 18-38 years), 50 ± 4.9 kg (range: 39.9-59.1 kg), 150 ± 5.4 cm (range: 143.2-160.3 cm), respectively. Their mean (±SD) BMI was 22 ± 2.1 with a range of 18.4 to 24.9.
Total calcium, vitamin D, PTH, and albumin concentrations were 2.32 mmol/L, 13.75 ng/mL, 7.15 pg/mL, and 4.1 g/dL. These findings are summarized in Table 1. The results of this study show that the study participants were deficient in vitamin D and also had low PTH.
Baseline Anthropometry and Status of Calcium Related Hormones.a
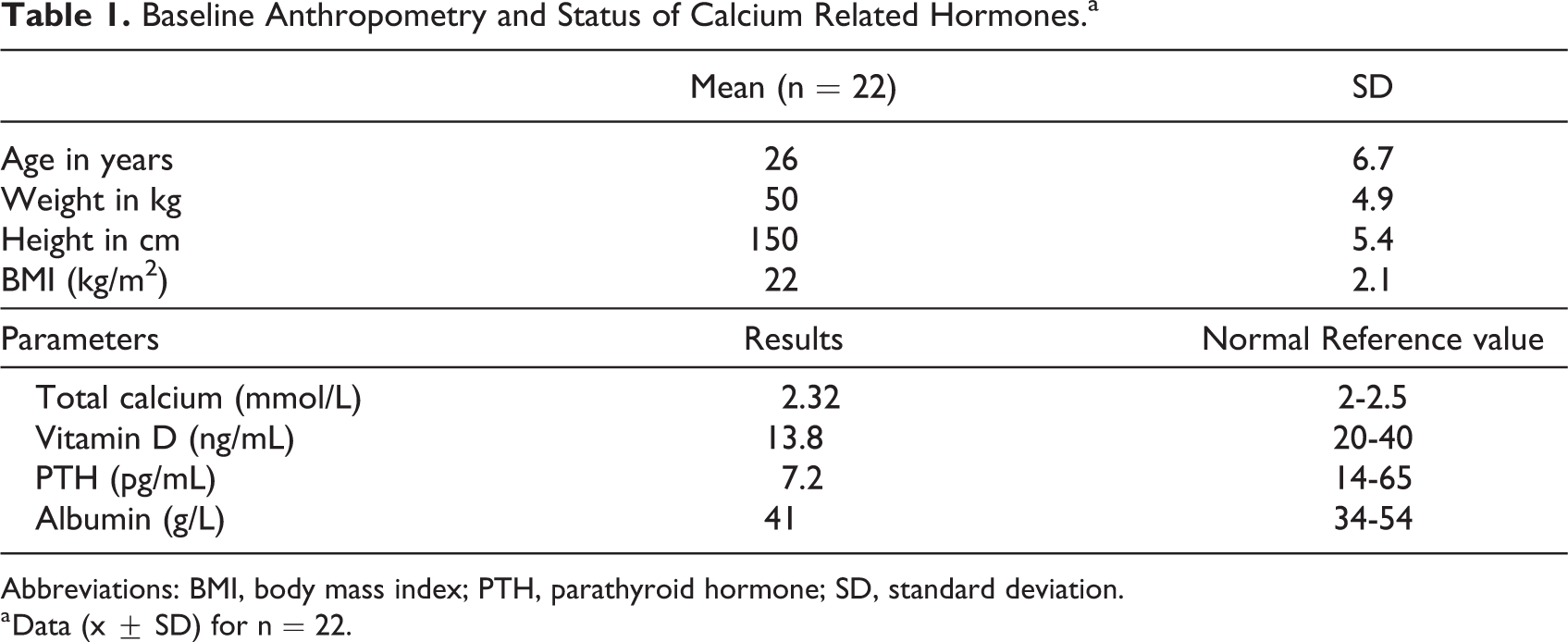
Abbreviations: BMI, body mass index; PTH, parathyroid hormone; SD, standard deviation.
a Data (x ± SD) for n = 22.
The mean dietary calcium concentration of the test meals was 879.5 ± 152.9 µg/g with a coefficient of variance (CV) of 17.2%. When we analyzed the 24-hour urine samples in three 8-hour pools, 0.263, 0.402, and 0.391 FAC were found with CV of 28.5%, 23%, and 22.3%. There was no significant difference between FAC calculated using the second or third 8-hr pool, although both were significantly higher than the second. We used the third pool as this time period represents optimum secreted isotope equilibration in the urine (Table 2). Although calcium absorption efficiency decreases with higher calcium intake, true calcium absorption was significant with 69.0 ± 15.6 mg per meal (Table 2). Therefore, one can acquire around 210 mg elemental calcium a day if slaked lime fortified rice is consumed 3 times a day (3 × 200 g cooked rice).
Calcium Intake and True Calcium Absorption.
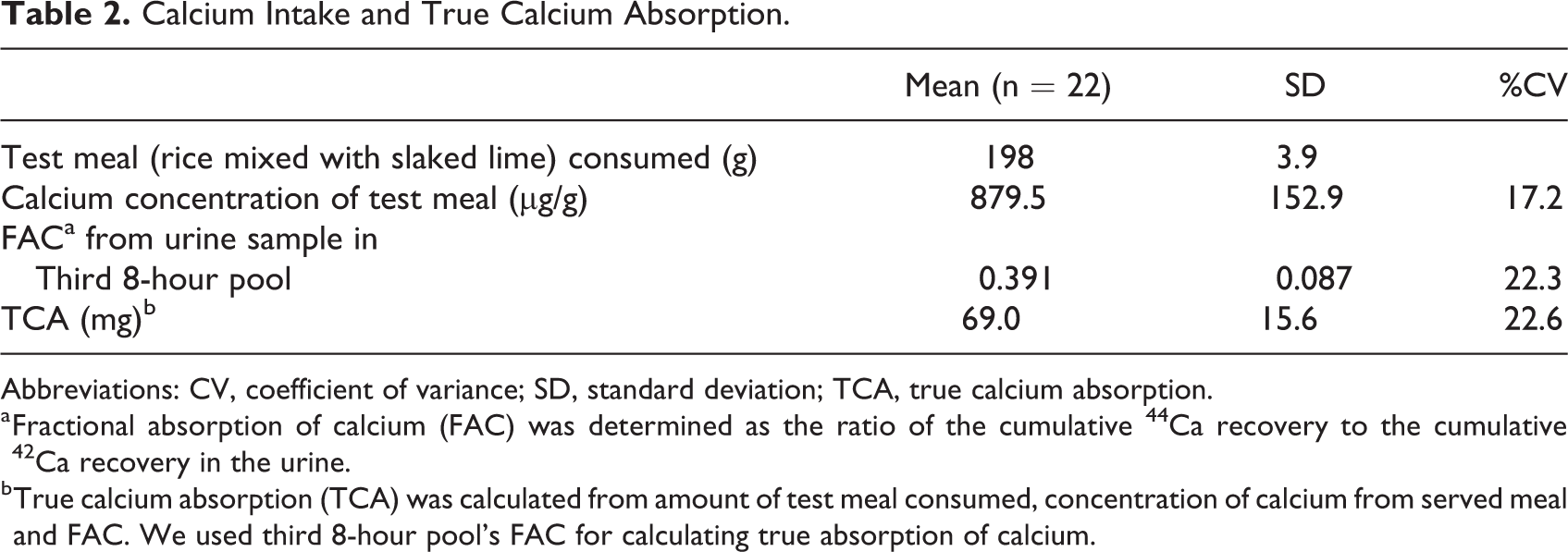
Abbreviations: CV, coefficient of variance; SD, standard deviation; TCA, true calcium absorption.
a Fractional absorption of calcium (FAC) was determined as the ratio of the cumulative 44Ca recovery to the cumulative 42Ca recovery in the urine.
b True calcium absorption (TCA) was calculated from amount of test meal consumed, concentration of calcium from served meal and FAC. We used third 8-hour pool’s FAC for calculating true absorption of calcium.
Mean (±SD) intake of slaked lime mixed rice, fried green papaya, and lentil soup were 198 ± 3.9 g, 69 ± 1.7 g, and 80 ± 2.7 g, while the served amount was 200 ± 1.3 g, 70 ± 0.0 g, and 82 ± 3.0 g per serving (Table 3).
Total Meal Intake (g) and Residuals.a
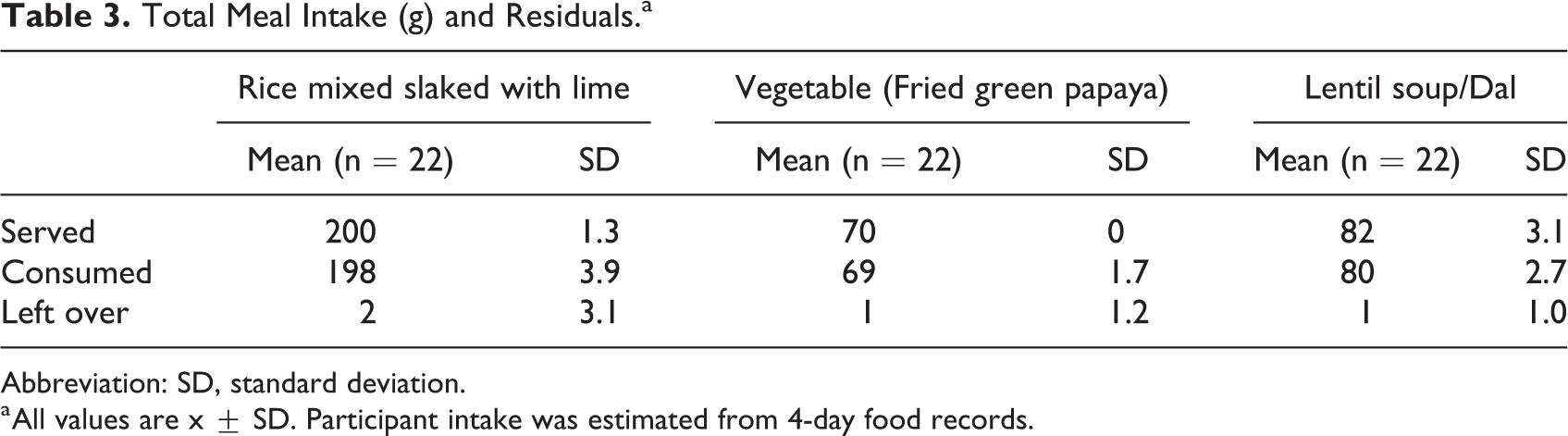
Abbreviation: SD, standard deviation.
a All values are x ± SD. Participant intake was estimated from 4-day food records.
Discussion
In the present study, calcium absorption from cooked rice was measured using dual tracer stable isotopes, which is the most accurate and precise method for determining calcium absorption from diet. 11,12 -14 Without lime treatment, rice is not a good source of calcium. Mean calcium concentration of cooked rice without fortification was 76 mg/kg, whereas it was 614 mg/kg when fortified with 7.5 g slaked lime/500 g uncooked rice. 8 In this present study, we determined 0.39 FAC by the dual isotope technique using the third 8-hour urine pool. The FAC for the NPNL and nonmenstruating women in our study was higher than postpartum lactating (0.238 ± 2.9) and nonlactating (0.25 ± 3.3) women and never pregnant (0.173 ± 3.3) women. 15 Similar results were found among nonlactating (0.153 and 0.176) and lactating (0.225 and 0.192) women when oral isotope was given in milk with high and low calcium meal prior to administration of isotopes accordingly. 16,17
Low- and middle-income countries (LMICs), especially Sub-Saharan Africa and Southeast Asia, are mostly prevalent in calcium deficiency with intake figures around 200 mg/day, whereas it is 600 to 800 mg/day in high-income counties (HICs). 13 Calcium-rich diets, including dairy products, are costly in Bangladesh, making less intake of food derived calcium. In Bangladesh, 47% of high-income women did not meet the WHO’s lowest recommended dietary allowance (RDA) (400-500 mg/d), and 63% of low-income women had intakes below 200 mg/d. 14 Therefore, the dietary intake difference between LMICs and HICs is obvious, and supports approaches such as food fortification to improve calcium intake in LMICs. 18
According to National Micronutrients Status Survey serum calcium and prevalence of vitamin D deficiency (< 50 nmol/L) among NPNL reproductive-age women in Bangladesh was 8.9 mg/dL (95% confidence interval: 8.4-9.3) and 71.5%. It is to be noted that mean serum calcium did not vary considerably by region or by quintiles of socioeconomic or food security status, which specifies extensive, severe vitamin D deficiency in Bangladeshi women. 19 Our present study showed similar mean serum calcium of 8.5 mg/dL and 95.4% vitamin D deficiency among NPNL women.
Parathyroid hormone is regarded as a reliable marker of inadequate calcium availability and bone loss is directly or indirectly linked to its overproduction. 20 Lack of vitamin D reduces the intestinal absorption of calcium and subsequent fall in extra-cellular fluid, thus an increase in PTH level secretion occurs from parathyroid gland. However, secondary hyperparathyroidism may occur in only half of the patients with hypovitaminosis D and the other half doesn’t have an adequate PTH response resulting in functional hypoparathyroidism. 21 There are some conditions associated with low serum PTH level such as Malnutrition-Inflammation-Cachexia syndrome, markers of malnutrition and inflammation, metabolic syndrome calcium-based binders, oxidative stress, calcium-rich diets, advanced age, higher calcium concentration in dialysate bath, diabetes mellitus, peritoneal dialysis, and Caucasian race. 22 -24 The result of this study shows the study participants are chronically Vitamin D deficient and also have relatively low PTH in the face of hypocalcemia for many participants. This may be due to concurrent magnesium insufficiency, which is associated with impaired PTH secretion and responsiveness. However, several calcium absorption studies showed an increase of FAC from 3% to 6.7% when high dose of vitamin D (4000-50000 IU/day) was administered. 25
In Bangladesh, calcium supplements during pregnancy may serve as a successful preventive measure in a population where 47% of women receive 4 or more antenatal care (ANC) visits. 26 However, even if they receive ANC, calcium supplementation (calcium lactate) that has been delivered from the government level during antenatal and postnatal care seems to have only 12% bioavailability. 27 Unfortunately, the high cost of calcium carbonate (40% bioavailability) tablets renders calcium supplementation in Bangladesh almost impossible. 27 Therefore, we tried an alternate way to supplement calcium.
Calcium absorption depends on the amount of calcium present in the food. It is evident from a Mexican study where the addition of calcium in corn tortilla during lime treatment increases calcium concentration and total calcium absorption. The total amount of calcium absorbed per treatment was higher in lime treated home corn flour (98.10 mg ± 21.7) than in lime treated commercial corn flour (59.9 mg ± 23.7, P ≤ .001) and corn flour with no lime treatment (3.78 mg ± 0.9, P ≤ .001). 11 In our previous study, we also found increased calcium concentration in a dose-response manner. Mean calcium concentration of cooked rice fortified with 0, 2.5, 5.0, 7.5, and 10 g slaked lime per 500 g uncooked rice was 76, 206, 428, 614, and 811 mg/kg, respectively (P < .001, by independent t test). 8
Although the percent absorption of calcium is inversely proportional to the amount of calcium in a food or meal, the actual amount of absorbed calcium will generally be higher with higher intake. The calcium content is multiplied by the absorption percentage of the given food to calculate the estimated true calcium absorption in the intestine. 28 Our study found 69.0 mg calcium per meal (200 g rice, 70 g lentil soup, and 82 g fried green papaya) when participants consumed rice fortified with 7.5 g slaked lime. According to the present study result, one can absorb around 200 mg of calcium calcium with consumption of the same amount of rice (3 meals per day); this provides about one-fifth of daily calcium recommendation. Therefore, lime fortified rice would be a good source of calcium and may help prevent calcium deficiency among populations surviving on staple food as rice.
Many food-based interventions such as homestead gardening intervention, provision of ready-to-use-supplementary food with locally available ingredients, wide-scale cultivation of small fish, and educational training have already been implemented in Bangladesh 29 -32 to prevent calcium deficiency. Nonetheless, these initiatives’ sustainability is a concern; rather, home fortification seems to be an effective, affordable, and less expensive alternative way. This deficiency can simply be prevented by adding locally sourced calcium (slaked lime) to rice cooking. 3 The habitual intake of lime-treated tortillas has already contributed to increasing calcium intake among Mexican women and preventing bone loss and osteoporosis. 3 It has also been implicated in indigenous Maya in Guatemala and in Ethiopia since 1980 and demonstrated low incidence of preeclampsia among those populations. 10 The additional intake of lime during cooking rice has also decreased the prevalence of rickets in Bangladesh. 7 Since rice is a staple food in Bangladesh and is consumed by the vast population, it could be an innovative solution in reducing calcium deficiency in Bangladesh.
We acknowledge that a stable isotope method for measuring calcium absorption from a single diet/meal does not address the long-term effects of calcium on bone health. Therefore, further study on bone mineral density and biochemical markers of bone metabolism may help to predict the overall bioavailability of dietary calcium. Additionally, other micronutrient deficiencies, including especially of Vitamin D, must also be addressed.
Strength and Limitation of the Study
We have conducted this study under direct supervision of research staff for 5 days to maintain the controlled diet that they consumed. The sample size of the study is also adequate enough to measure true calcium absorption of calcium from food. It would be more helpful if we could also keep a control group without slaked lime fortification.
Footnotes
Authors’ Note
Data described in the manuscript, code book, and analytic code will be made available upon request to the corresponding author.
Acknowledgments
This research study was funded by Swedish International Development Agency (Sida), grant number GR-01455. icddr, b acknowledges with gratitude the commitment of Sida to its research efforts. icddr, b is also grateful to the Governments of Bangladesh, Canada, Sweden, and the United Kingdom for providing core/unrestricted support.
Author Contributions
NNN was the Principal-investigator of the project and responsible for development of concept, project conception, study oversight, data collection, reporting of the study results, and prepared the first draft. SD has contributed to the research plan and statistical analysis. NFK has contributed to the study design, lab analysis, and provided expert opinion; and JL, JW, KAM, and RA have contributed to the research plan, data collection, and procedures during the study period. JL, JW, and NFK were responsible for isotope analyses. MMI was responsible for research design and overall supervision of the project. TA contributed to the study design, development of concept, and reviewed the draft. All authors read, reviewed, and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by Swedish International Development Cooperation Agency (Sida).