
Abstract
Background:
Socioeconomic factors influence diet quality during pregnancy. However, a dearth of evidence about the influence on energy and macronutrients adequacy calls for research.
Objective:
To analyze the association between socioeconomic factors and adequacy rates of energy and macronutrient intakes in pregnant women from Merida, Yucatan, Mexico.
Methods:
During September to December 2019, we applied a socioeconomic questionnaire and three 24-hour dietary recalls to 83 pregnant females resident in Merida, Yucatan. Energy and macronutrient intakes were compared with the estimated trimester-specific energy and macronutrient requirements to calculate adequacies (%). Outcome variables were average adequacy of energy, carbohydrates, total fat, and protein intakes and the main predictors were maternal education, monthly family income, working status, and marital status. Descriptive statistics of adequacy were calculated for each category of predictors. The association between socioeconomic factors and outcome variables was analyzed through simple and multiple linear regression models.
Results:
Adequacy rates of energy and macronutrients decreased as education and familial income levels increased, as well as among unemployed women. Consistently with these results, simple linear regressions showed that years of education, family income, and working status (i.e., women working to earn money), were negatively associated with adequacy rates of energy and macronutrients intakes. When all predictors and covariates were included in a multiple linear regression model, only having a job was significantly associated with adequacy rates. Marital status was not associated with outcomes.
Conclusions:
Women in disadvantaged socioeconomic conditions (unemployed and low levels of education and familial income) show greater energy and macronutrient intakes.
Introduction
Food intake in individuals is the result of complex interactions between physical environmental, biological, and socioeconomic factors. 1 Socioeconomic status includes variables, mainly education, income, and occupation, which together describe living conditions and social inequality among members of a given population. 2 Socioeconomic conditions may influence food intake and diet quality increasing or decreasing the access to foods and promoting individuals to make decisions regarding food choices. 3,4 Pregnant women are not exempt from the influence of socioeconomic conditions on their diet characteristics and nutritional quality.
The influence of socioeconomic factors on food intake and diet quality is particularly relevant during pregnancy given the potential effects not only on mothers’ but also on their offspring’s health and well-being. 5,6 Negative nutritional balance during pregnancy may increase the risk of several adverse birth outcomes including preterm birth, low birth weight, and intrauterine growth restriction, particularly in populations that experience adverse socioeconomic conditions. 7 Furthermore, nutritional excesses may increase the risk for excessive maternal weight gain 8 -10 which, in turn, has been associated with several adverse neonatal outcomes including low Apgar score, hypoglycemia, polycythemia, meconium aspiration syndrome, and large-for-gestational age. 11,12
Studies in several countries and socioeconomic backgrounds have shown that women with higher income and education levels tend to have a healthy dietary pattern, which comprises of the intake of green leafy vegetables, legumes, fruits, milk and dairy products, red meat, and chicken. 13 -18 In the United Kingdom and New Zealand, results from the Avon Longitudinal Study of Parents and Children (ALSPAC) and the Growing Up studies showed that low maternal schooling was related with higher consumption of processed food. 19,20 Marital status also seems to have some influence of food intake during pregnancy; studies undertaken in Ethiopia, Canada, and Brazil show that women with a partner tend to have a high-quality diet. 15,17,21 Most of these studies use principal component analysis (PCA) or diet quality indexes to assess food consumption in pregnant women. Principal component analysis analyzes the association between many foods and identifies the components of population-specific dietary patterns and diet quality indexes score dietary intakes, organized in several components, whose sum or total amount of points quantifies dietary quality.
Energy and macronutrients adequacy, defined as the relationship between intake and individual requirements and quantified as the rates of covered requirements, is also an important component in the assessment of dietary quality. 22 Adequacy is relatively easy to obtain and allows the assessment of both energy deficiency and excess and how energy intake is distributed between carbohydrates, fats, and proteins in populations. An intake of macronutrients within the adequate distribution range is associated with reduced risk of chronic disease. 23 However, the number of studies that has analyzed the influence of socioeconomic factors on energy and macronutrients adequacy is limited. 24 -26
The analysis of the influence of socioeconomic factors on diet adequacy in pregnant women is relevant in populations found in low- and middle-income nations where inequalities in income and access to education and health services and healthy foods are deep. In their review of 62 studies about dietary intake in pregnant women from low- and middle-income countries in Asia, Africa, the Caribbean, and Central/South America, Lee et al 27 found that in 44% of studies included in the review macronutrient intakes were not within the recommended ranges. Mexico is a country with high socioeconomic inequality among its population; northern and central states show the highest levels of economic growth and well-being, while the southern states have been historically characterized by poor economic development and have the highest levels of poverty and social inequality. 28 The state of Yucatan, located in the southeast of the country, has about 2.3 million inhabitants, distributed among 106 municipalities; 42% of the state’s population live in Merida, its capital. 29 Socioeconomic segregation is a distinctive characteristic of the population of Merida and contributes to noticeable differences in income and access to basic services such as health and education. Socioeconomic disparities in this city have shown their impact on several components of individuals’ phenotype and population’s epidemiological profile. 30,31 Factors experienced by individuals during the early stages of development, including diet during pregnancy, may be playing an important role. In this study, we analyze the association between socioeconomic factors and adequacy rates of energy and macronutrients intake in pregnant women from the municipality of Merida.
Methods
The Study Location
This observational and cross-sectional study was carried out in the municipality of Merida, which includes the capital city and 14 comisarías, small localities near to Merida. Nine localities were selected for this study based on the presence of health units that provide services for pregnant women. All these localities are less than 5 km from Merida, which results in an intense relationship in terms of commerce, employment, and education and health services.
Sample
The sample size was calculated considering that the study had to compare categorical variables using chi-square tests, as well as verify the existence of associations (correlations) between them. To guarantee the existence of at least 5 observations in each combination of categories of the variables, it was required to work with at least 60 sampling units. The final sample consisted of 83 pregnant women older than 18 years of age.
Participants were recruited from 6 public hospitals or health units (3 belonging to Mexican Institute of Social Security and 3 from the Ministry of Health of Yucatan State) with 3 being private institutions. Initially, we met representatives of these institutions to obtain their formal authorization to undertake the study. Then, we organized informative meetings with pregnant women attending their prenatal care checkups. During these meetings, potential participants received detailed information about the aims of the study, their participation, potential benefits, and rights as participants. Those women who agreed to participate provided us with their address and phone number to make an appointment to begin the process of obtaining data. Our inclusion criteria were (1) being pregnant, (2) older than 18 years of age, and (3) resided in the municipality of Merida. We excluded from the analysis women with a medical diagnosis of diabetes and/or hypertension.
Data Collection
Between September and December 2019, we collected data on socioeconomic, pregnancy and diet characteristics, and anthropometric measures of women during 3 household visits. During the first visit, we applied a questionnaire developed in the Laboratory of Somatology at Cinvestav-Merida which obtained information about the women’s age, family composition, marital status, education, occupation and income of all family members, number of offspring, and gestational age. Age was classified into 3 groups at tertile points: (1) 18 to 24 years, (2) 25 to 29 years, and (3)
During our first visit, we measured women’s height and weight and asked them to provide us with their weight prior to pregnancy. We calculated pregestational body mass index (BMI = weight [kg]/height [m2]) and classified women as normal weight (18.5-24.9 kg/m2), overweight (25-29.9 kg/m2), and obese (>30 kg/m2). Pregestational and pregnancy anthropometric data are used in this article only for descriptive purposes.
Two qualified nutritionists applied 24-hour dietary recalls 3 times during a 7-day period, twice during the week and once at the weekend. The surveyors followed the multiple-step method, 32 because of its precision in obtaining data and reducing bias in the reported foods. This procedure consists of 5 steps: (1) to list of all foods consumed in the day, (2) to list forgotten foods, (3) to record schedules and meal times, (4) to obtain meal details, and (5) final review. Standardized kitchen utensils (spoons, cups, plates, and glasses) were used to register food quantities in order to increase the accuracy of consumption measurement. For foods made with more than one ingredient, each ingredient was register, except for fast food, packaged food, and beverages. The 24-hour dietary recalls were analyzed using the software Nutrium to estimate energy (kcal/day) and macronutrient (g/day) intake rates. Energy and macronutrient consumption rates were compared with the estimated trimester-specific energy and macronutrient requirements 33 to calculate adequacies (percentages) for each day of consumption. The energy distribution in macronutrients was based on the recommendation of the Food and Agriculture Organization of the United Nations 33 as follows: 55% for carbohydrates, 30% for fat, and 15% for protein. For descriptive purposes, intake rates of energy and macronutrients were defined according to the percentage of requirement as below normal: <90%, normal: 90% to 110%, and above normal or high: >110%, as proposed by Suverza and Haua. 34 Dietary data were extensively reviewed by a nutritionist to identify possible atypical consumptions and adequacies.
Data Analyses
Descriptive statistics of maternal sociodemographic characteristics and energy and macronutrients intake are presented for the total sample. Mean and standard deviations (SD) of energy and macronutrients adequacy were calculated for each category of independent variable; Student t tests were used to compare dietetic adequacy between categories of marital and working status, and one-way analysis of variance tests we applied to compare dietetic parameters between categories of education level and familial income. The relationship between socioeconomic factors and diet characteristics was analyzed through simple and multiple linear regression models. Outcome variables were average adequacy of energy, carbohydrates, total fat, and protein intake. The main independent variables were family income (numerical), women’s years of education (numerical), marital status (categorical), and working status (categorical). Since obesity may alter food behavior, multiple linear regression models were also adjusted for the presence of prepregnancy excess body weight (BMI > 24.9 kg/m2). Several diagnostic tests were applied to determine the regression models validity. All models met the assumptions of normality of residuals, homogeneity of variance, and the variance inflation factor. Data entry and analysis were made with Stata/IC 11.1 for Windows statistical package (StataCorp LP, 2010). The significance level for statistical tests was α = 0.05.
Ethical Clearance
This study was approved (057/2019) by the Bioethics Committee for the Study of Human Beings of the Centre for Research and Advanced Studies of the National Polytechnic Institute (Cinvestav-IPN) of México. Participant women signed consent forms during the first household visit.
Results
The age of participant women ranged from 18 to 40 years (Mean = 27.6 years, SD = 5.2; Table 1). The mean of total years of education was 13.1 (SD = 3.7) and 42% finished university or held a technical qualification. Most of the participants (89%) reported having a partner at the moment of the study and 59% reported having a job. Monthly family income ranged from MXP 3200 to 63 000 (US$169 to US$3330) with a median of MXP 15 000 (interquartile range [IR] = MXP 7650-22 000) (Median = US$793, IR = 404-1163). Working women had more years of education (Mean = 15, SD = 0.56 vs Mean = 11, SD = 0.42; P < .001) and familial income (Median = MXP 18 500, IR = 14 000-24 000 vs Median = MXP 8825, IR = 6000-16 000, P < .001) than nonworking women. The mean gestational age was 22.6 (SD = 8.3) weeks and 53% and 31% of women were in the second and third trimesters of pregnancy, respectively.
Sociodemographic and Pregnancy Characteristics of Participant Women.a
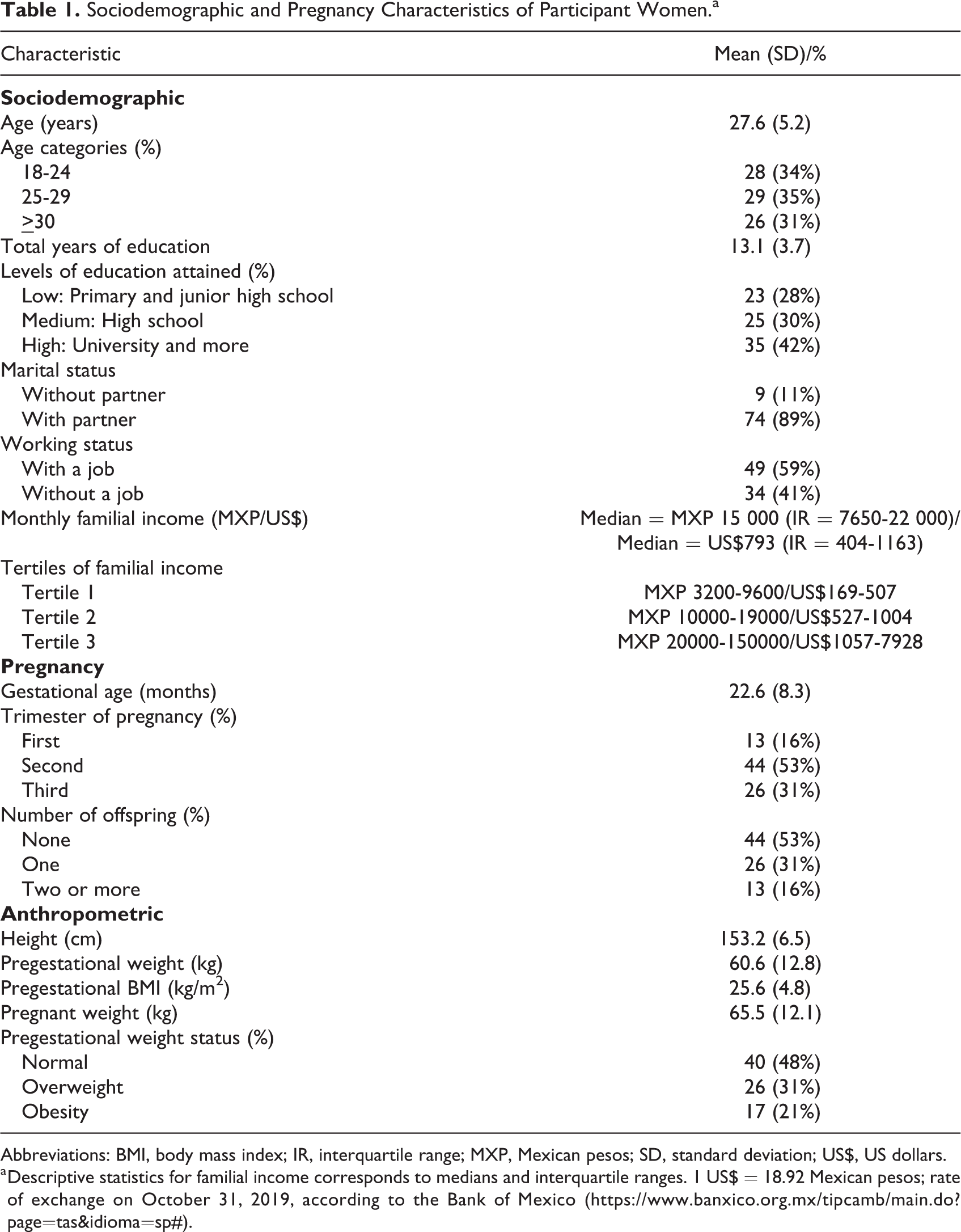
Abbreviations: BMI, body mass index; IR, interquartile range; MXP, Mexican pesos; SD, standard deviation; US$, US dollars.
a Descriptive statistics for familial income corresponds to medians and interquartile ranges. 1 US$ = 18.92 Mexican pesos; rate of exchange on October 31, 2019, according to the Bank of Mexico (https://www.banxico.org.mx/tipcamb/main.do?page=tas&idioma=sp#).
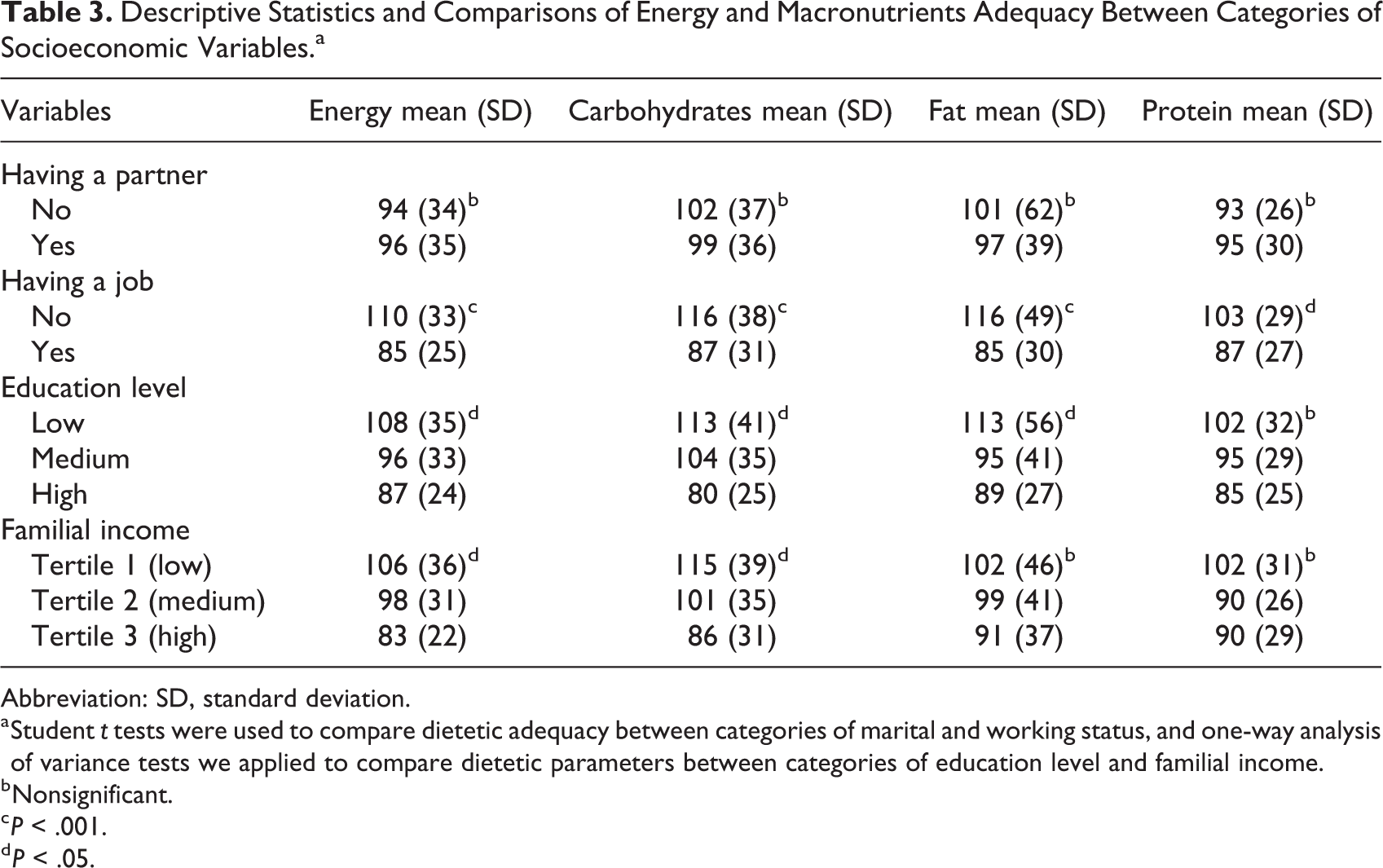
Descriptive statistics of energy and macronutrients intake and adequacy rates are presented in Table 2. The means of adequacy rates for energy and macronutrients fell between the recommendable ranges in the overall sample. However, 45% of women did not meet their energy requirements (below 90% adequacy) and 57% exceeded their intake of carbohydrates (above 110% adequacy). Adequacy rates of energy, carbohydrates, and fat significantly decreased as education and familial income levels increased (Table 3). Women with a job at the time of the study showed 25%, 29%, 31% and 16% points less in energy, carbohydrates, total fat, and protein adequacy rates, respectively, than women without a job. Women with and without a partner showed similar adequacy rates. These findings were consistent with results obtained in simple linear regressions.
Descriptive Statistics of Energy and Macronutrients Intake and Adequacy Rates of Pregnant Women.
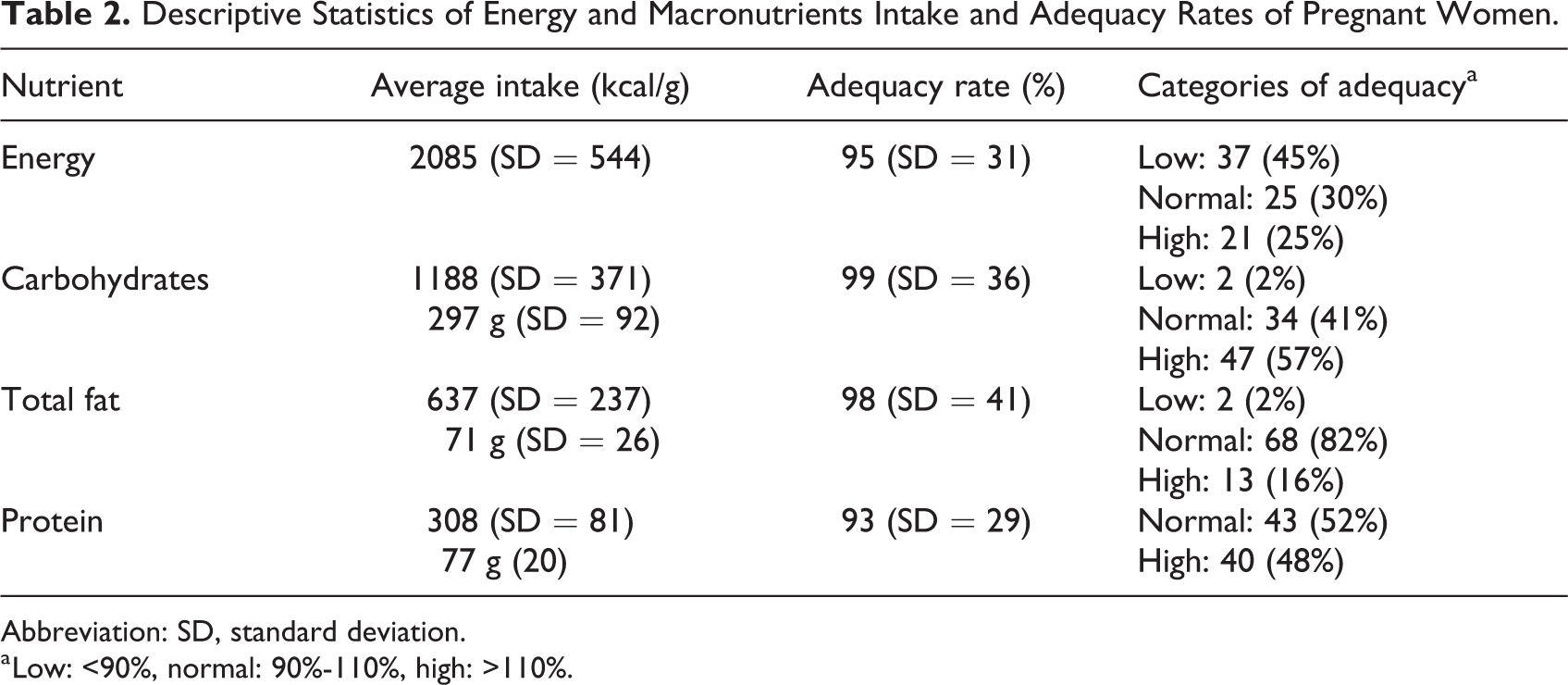
Abbreviation: SD, standard deviation.
a Low: <90%, normal: 90%-110%, high: >110%.
Descriptive Statistics and Comparisons of Energy and Macronutrients Adequacy Between Categories of Socioeconomic Variables.a
Abbreviation: SD, standard deviation.
a Student t tests were used to compare dietetic adequacy between categories of marital and working status, and one-way analysis of variance tests we applied to compare dietetic parameters between categories of education level and familial income.
b Nonsignificant.
c P < .001.
d P < .05.
Simple linear regression analyses showed that having a job was associated with decreases in adequacy rates of 21%, 24%, 26%, and 13% in energy, carbohydrates, lipids, and proteins intake, respectively (Table 4). Family income was negatively associated with adequacy rates of energy and carbohydrates intake, but effects were substantially lower (−0.3% and −0.4%, per each MXP 1000 increase in family income, respectively). Each additional year of education was associated with decreases of 2% to 3% in adequacy rates of energy, carbohydrates, and lipids intake. When all socioeconomic variables and prepregnancy excess body weight were included in a multiple linear regression model (not presented in tables), we found that having a job was significantly associated with higher adequacy rates of energy (B = −15.31 [SE = 6.83], P < .05) and lipids (B = −25.22 [SE = 10.83], P < .05) rates. The rest of sociodemographic predictors were not associated with the outcome variables.
Associations Between Adequacy Rates and Socioeconomic Variables, Through Simple Linear Regression Models.
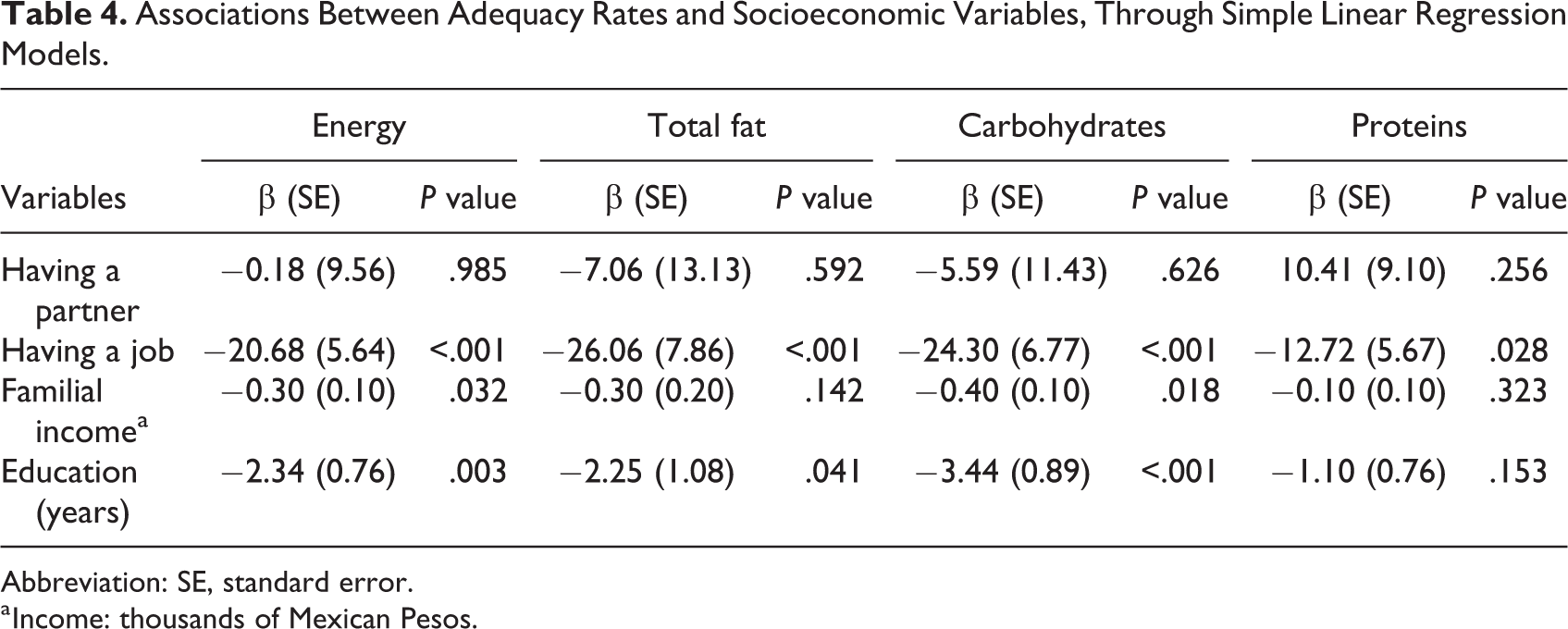
Abbreviation: SE, standard error.
a Income: thousands of Mexican Pesos.
Discussion
In this sample of Yucatecan women, we found that working status (i.e., women working to earn money), years of education, and family income were negatively associated with energy and macronutrients adequacy rates during pregnancy. Women experiencing more disadvantageous socioeconomic conditions, that is, lower levels of education and family income and unemployment, show greater energy and macronutrient intakes.
Energy and macronutrient intakes of pregnant women in this study are comparable with intakes of women residing in low- and middle-income countries from Asia, Africa, and Latin America, including Mexico. 27 On the other hand, women in our sample show, on average, an intake of 60 kcal/day of energy and 15 g/day of total fat less than women from developed countries, including the United States, Canada, the United Kingdom, Denmark, Norway, Australia, and Japan. 35 However, women participating in our study show a slightly greater intake of carbohydrates than women from these developed countries (297 vs 269 g/day). Overall, these differences and likenesses may reflect the effect of macro-level socioeconomic disparities that influence availability, access, and selection of food choices and shape dietary patterns in populations. 36
We found that energy and macronutrients adequacy rates decreased as the levels of education and familial income increased, which is consistent with the results obtained by Blumfield and collaborators 35 in their systematic review of studies with pregnant women from developed countries. In our sample, energy intake in the lowest level of education was 2374 kcal (SD = 589), 2068 kcal (SD = 563) for the medium, and 1906 kcal (SD = 482) for the highest. Corresponding values by tertiles of familial income were tertile 1: 2284 kcal (SD = 557), tertile 2: 2136 kcal (SD = 548), and tertile 3: 1841 kcal (SD = 443). Women in the highest levels of education and income tended to be near to the lower limit of the normal range of energy and macronutrient adequacy. In contrast, adequacy rates of carbohydrates of women in the lowest levels of education and income were above the upper limit of the normal range. The negative association found in this study between education, income, and energy and macronutrient intakes through simple linear regressions is consistent with what has been found in nonpregnant women, adult men, and children from different populations. 37 -41
Working status of women was also associated with nutritional adequacy in our sample of pregnant women. Adequacy rates for energy and total fat were significantly higher in nonworking mothers than in working mothers. Differences in energy and macronutrients intakes between these two groups correspond to 242 kcal/day and 15 g/day of fat. Additionally, we found that the proportion of women with high adequacy of energy intake (>110%) was greater in nonworking women than in working women (38% vs 16%). Adequacy rates of working mothers closely resemble those of women with the highest levels of education and income. Few studies have analyzed the influence of working status on diet quality during pregnancy. 19,42 In the ALSPAC, Northstone, Emmett, and Rogers 19 found that working pregnant women tended to have a health-conscious dietary pattern, which was characterized by the high consumption of salads, fruit, rice, pasta, oat, fish, fruit juices, and nonwhite bread. In the Study of Food Intake and Eating Behavior during Pregnancy undertaken in Brazil during 2006 to 2007, Hoffmann et al 42 found that being a working woman was associated with the consumption of a more varied dietary pattern, while nonworking women showed a restricted pattern which is characterized by a higher consumption of energy-dense foods.
The higher levels of formal education and familial income found in working women allow us to suggest that this group experience better socioeconomic conditions, which could make them more likely to access and select less energy-dense foods including fruits, vegetables, and grains, which would contribute decreasing the energy and macronutrient adequacy rates. Marital status was not associated with nutritional adequacy rates in this sample, which may be explained by the fact that a minor proportion (n = 9, 11%) of participant women reported not having a partner at the moment of the study.
Our results indicate that the energy intake of an important proportion (45%) of women in this sample was lower than recommended, as has been reported in pregnant women residing in urban contexts in Mexico 43,44 and countries that experience better socioeconomic conditions. 35 In this regard, Dufour et al 45 have proposed that deliberate changes in physical activity during pregnancy, particularly more time allocated to energy-saving activities and less time to more energy-demanding activities, may be an important way to meet energy demands during pregnancy. Blumfield et al 35 also proposed that energy homeostasis during pregnancy can be achieved by relative reductions in the women’s basal metabolic rate as have been reported in some populations 46,47 and by women’s weight status at the beginning of pregnancy. In this respect, some studies have reported that women who enter pregnancy with higher values of BMI tend to have less healthy dietary patterns during pregnancy 14,48 -50 ; though few studies have focused on nutritional intakes and adequacies in relation to prepregnancy BMI. 51,52 Overall, these results suggest that physiological adaptations experienced by women during pregnancy may buffer low energy intake during pregnancy driven by socioeconomic factors.
Limitations
The percentage of women with high level of education (42%) and the median of monthly familial (MXP 15 000 [US$793]) indicate that the sample of this study tend to overrepresent the population of medium socioeconomic level from the municipality of Merida, thus our results should interpreted only in the context of the sample. More research that includes the more disadvantaged socioeconomic groups in this geographical region is needed. Also, the small sample size limited us to include other important socioeconomic variables in the analyses.
Conclusions
This study found energy and macronutrient inadequacies (deficiencies and excesses) in this sample of pregnant women from Merida, Yucatan, Mexico. Women under disadvantageous socioeconomic conditions, namely, those with lower levels of education and family income and without a job, show greater energy and macronutrient intakes. From a public health point of view, these findings are important in delineating the groups at risk in terms of their socioeconomic circumstances.
Footnotes
Acknowledgments
The authors thank their colleagues who participated in the fieldwork and research, especially Graciela Valentin, Niky Searle, Patricia Kantun, Gabriela Solís, and Erika Karter, who made anthropometric measurements and applied dietary recalls to women. The authors also thank the authorities of institutions where participant women were recruited: the IMSS, the Ministry of Health of Yucatan, the Maternal Connection psychoprophylactic center, the Mothers Love center, and to the authorities in Cholul, Chablekal, San José Tzal, Oncan, and Dzununcan. The authors thank all the women who participated in this study, for trusting us, allowing us to enter their homes, and giving us the necessary time to obtain all the information.
Author Contributions
DRV, HA, and FD: Conceptualized the research project; JLB: Supervised the sample size calculation and the statistical analyses of the data. HA: Wrote the first draft of the manuscript and all coauthors read, revised, and added intellectual content to the manuscript. MTCB: Collaborated in the project development, and for this article read, revised, and added intellectual content.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.