
Abstract
Background:
Adolescent overweight and obesity (AOO) is a global public health problem and risk for noncommunicable diseases. Understanding context-specific risks is crucial for interventions.
Objective:
Determine the prevalence of AOO in the Indonesian National Health Survey (INHS) 2013, assess the 5-year trend from 2013 to 2018, and identify risks.
Methods:
We selected adolescents aged 10 to 19 years (n = 174 290) from the INHS 2013 and used hierarchical logistic regression to identify gender-specific risks for those aged 15 to 19 years (n = 77 534). Change in AOO was assessed by comparison to INHS 2018 reports.
Results:
The national AOO prevalence increased over 5 years by 48% in young adolescents (13-15 years) and 85% in older ones (16-18 years). High prevalence areas included the urban location of Jakarta (20.9%) and the remote rural region of Papua (19.4%). Overall, AOO risks were being sedentary, male, lower education, married, younger adolescent, and school enrollment, with urban residence and higher wealth being persistent risks for all analyses. Data for depressive symptoms were available for older adolescents whose additional risks were being sedentary, depressive symptoms, and high-fat diet. Male risks were being sedentary and lower education, and female risks were being married, depressive symptoms, high-fat intake, and lower education. Higher intake of fruits and vegetables and fewer sweets did not protect against AOO if a high-fat diet was consumed.
Conclusions:
Adolescent overweight and obesity in Indonesia is rapidly increasing, especially in older adolescents and males, and with gender-specific risks. Customized multisectoral interventions to identify strategies for lifestyle change are urgently needed.
Introduction
Obesity is a global public health concern and contributes to 2.6 million deaths worldwide every year. 1 The prevalence of obesity has escalated in many countries, including those in East and South Asia, where an accelerated rise in body mass index (BMI) has been reported. 2 Furthermore, the coexistence of obesity and malnutrition in many low- and middle-income countries (LMIC) presents a challenging double burden. 3 Moreover, around 10% of young people aged 5 to 19 years are overweight or obese. 4 Specifically, adolescent overweight and obesity (AOO) is considered particularly serious due to its lifelong effects, 5 making it among the top public health challenges of the 21st century. 4
Obesity is associated with significant health risks and comorbidities, such as cardiovascular disease, hypertension, hyperlipidemia, type 2 diabetes, and certain cancers. 1 It is associated with an increased risk of morbidity and mortality, as well as reduced life expectancy. Compared with individuals of healthy weight, life expectancy from age 40 years was 4.2 years shorter in obese men and 3.5 years shorter in obese women. 6 High BMI contributed to an estimated 4 million deaths globally in 2015. 7 Several studies and meta-analyses have found strong associations between BMI and nearly all causes of mortality, an exception being transportation-related accidents. 6 These associations with mortality are stronger at younger ages than at older ones and often exhibit a U-shape with minimum death in the healthy BMI range. 6,8,9 Unfortunately, the past 2 decades have witnessed an increase in AOO and related health issues and health care costs. 10
Indonesia is one of the countries facing the double burden of malnutrition, and with an increasing prevalence of overweight and obesity, and AOO. Household survey data from the Indonesian National Health Survey (INHS) 2013 showed that 18.8% of children and adolescents aged 5 to 12 years were overweight or obese, as were 10.8% of adolescents aged 13 to 15 years, and 7.3% of adolescents aged 16 to 18 years. 10 By 2018, these prevalences had increased to 20% for children aged 5 to 12 years, 16% for adolescents aged 13 to 15 years, and 13.5% for adolescents aged 16 to 18 years. The national prevalence of AOO is expected to increase 2-fold by 2030, as seen in other countries, 1 if attention and interventions are not prioritized.
The etiology of AOO is multifactorial. Interactions between genetic, neuroendocrine, metabolic, psychological, environmental, behavioral, and sociocultural factors are evident. 11 However, the interactions between multifactorial determinants and the prevalence of obesity have rarely been assessed in countries experiencing the diverse challenges of overweight and obesity, malnutrition, infectious diseases, and rapid economic and social transition. A better understanding of the prevalence of AOO, along with its determinants, is crucial for the development of effective prevention strategies and will aid decision-making to optimize and implement a range of policies and strategies. 3 Given that Indonesia is the fourth most populous nation and that 1 in 7 persons with AOO resides therein, solutions from Indonesia may have global implications.
This study aimed to assess the national and subnational prevalence of AOO in Indonesia and to identify determinants by analysis of the 2013 INHS. The results may facilitate policymakers and multiple stakeholders to prioritize and address obesity among Indonesian adolescents and potentially other countries facing similar challenges.
Methods
This study used data from the INHS, known as Riskesdas in Indonesia, for the year 2013. Riskesdas is a nationally representative household health survey conducted every 5 years since 2007 by the National Institute of Health Research and Development, Ministry of Health, Republic of Indonesia. A multistage systematic random sampling method was used to select participants. 12 Details on the methodology of data collection and sampling procedures are provided elsewhere. 10,12 In brief, the INHS 2013 data include 1 027 763 individuals from 294 959 households from all 34 provinces and all 497 districts. 10 The analyses herein were restricted to adolescents as defined by the World Health Organization (WHO) as individuals aged 10 to 19 years. The INHS 2013 included adolescents aged 10 to 19 years and composed of 199 149 adolescents (96 673 females and 102 476 males) from 34 provinces.
The outcomes of this study were the prevalence of AOO in INHS 2013, 10 the 5-year trend in prevalence based on comparison with reports on AOO from INHS 2018, 13 and identification of determinants of AOO stratified by gender. The trend of AOO was assessed by comparison to reported indicators from the INHS 2018 for adolescents aged 13 to 18 years. As indicated in the INHS report 2013, 10 anthropometry data for weight and height on INHS 2013 were obtained from the primary measurement conducted by trained nutritionists. Body weight was measured using a portable digital scale (Fesco brand), and body height was measured using an aluminum portable stadiometer. All anthropometric measurements were assessed for accuracy and precision and reviewed by validators in the field. The demographic variables on gender, date of birth, date of current assessment, and weight and height were entered into WHO AnthroPlus-2007 software to calculate BMI for age z-score. Overweight and obesity were classified as BMI for age >+1SD and >+2SD, respectively, based on the WHO definitions. The AOO was coded as “1,” and normal adolescents (BMI for age +1 to −2SD) as “0” or reference. Adolescents with BMI < −2SD (thinness) or flagged as invalid, that is, −5SD or +5SD, were excluded.
We assessed previously identified 1,14 determinants or risk factors that were gathered with the INHS questionnaires, which were obtained from a face-to-face interview by INHS 2013. As shown in Figure 1, the variables were age, gender, marital status, school enrollment or working status, educational level, family income, mental health (depression), adolescent smoking behavior, lifestyle factors such as sedentary activity, and dietary patterns such as consumption of sweetened beverages and snacks, high-fat diets, as well as fruits and vegetables intake.
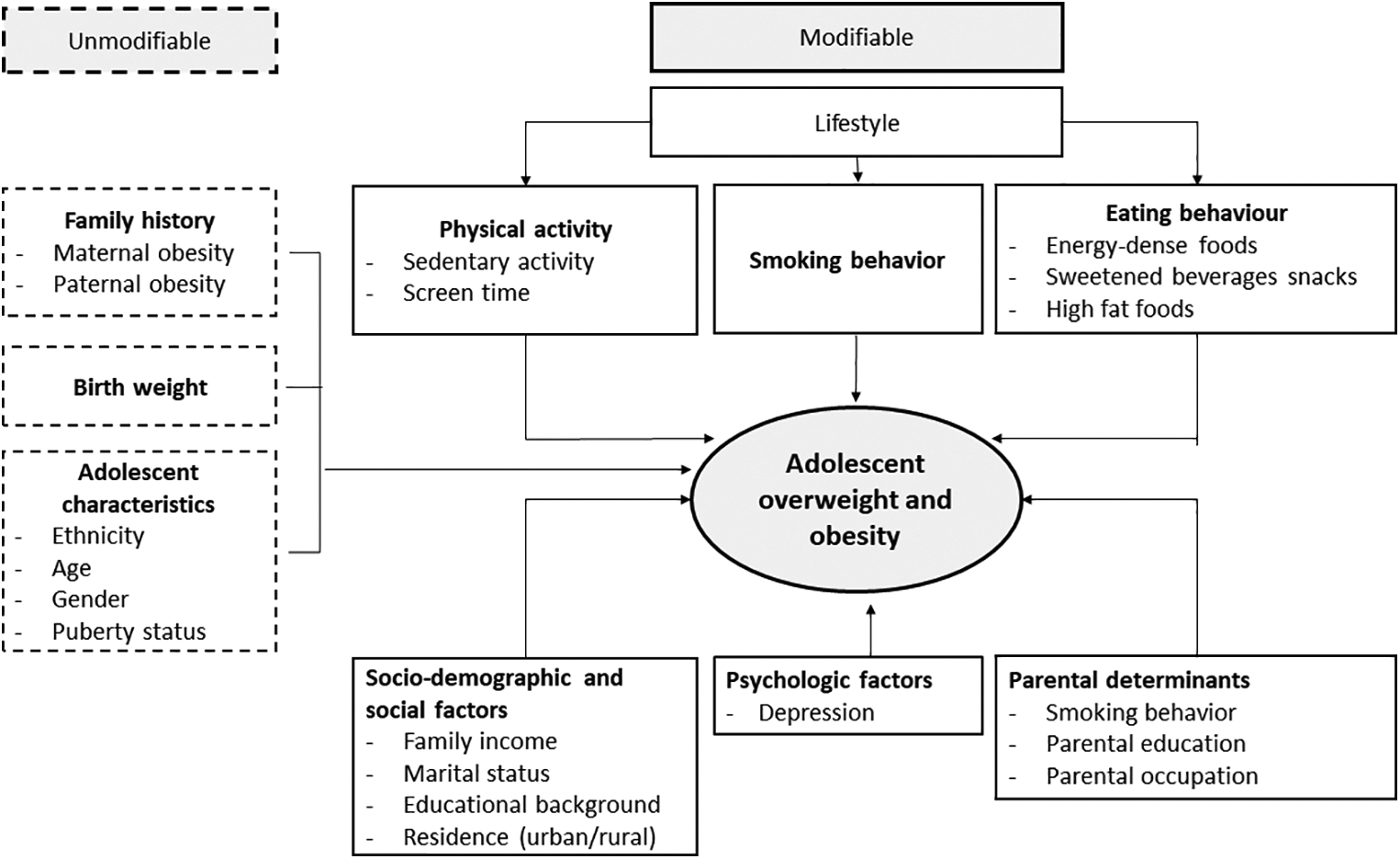
Theoretical framework for determinants driving adolescent overweight and obesity.
Family income was classified into 5 groups: lowest to highest quintile based on the Indonesia Wealth Index. Marital status was grouped into 2 categories: never married and married. Adolescent smoking status was grouped into 2 categories: never smoked and smoking/ex smoker. Education level was divided into 2 groups: 9 years or less and more than 9 years based on education regulations in Indonesia that mandate 9 years of schooling. Depressive symptoms were measured by a mental health questionnaire 15 used for INHS 2013, and persons were classified as depressed if a “yes” response was elicited for any of 3 questions: the participant feels worthless, loss of interest in anything, having suicidal thoughts. Depressive symptom data were available for older adolescents aged 15 to 19 years, but not in younger adolescents (10-14 years). Sedentary activity was measured by a questionnaire based on the reported duration of activities, such as sitting, lying down, watching television, playing games, and reading. 16 The participant was considered sedentary if the total sedentary activities were more than 120 min/d. 17 The residence was divided into rural or urban areas.
The frequency of food or drink consumption was based on respondent recall and categorized by interviewers as either: once or more per day, once a day, 3 to 6 times per week, less than 3 times per month, and never. we further categorized these into 2 groups: we coded as “0” a group comprising less than once per day, once a day, 3 to 6 times per week, less than 3 times per month, and never; and coded as “1” once or more per day. Fruits and vegetables were categorized into consumption of less than 5 portion per day and coded as “1”, and 5 portion or more per day coded as “0.”
Data were analyzed using the Statistical Package for Social Sciences, version 20. Descriptive and multivariable logistic regression analyses were performed. Descriptive analyses provided bivariate association of explanatory and outcome variables for further exploration of key determinants of AOO. Hierarchical logistic regression with survey weights was used to determine the adjusted associations with AOO in the overall group of surveyed adolescents, with available determinants being valid anthropometry data, and stratified by gender, for age, marital status, school enrollment or working status, educational level, residence, mental health, adolescent smoking behavior, and the lifestyle factors of sedentary activity and eating behaviors. Two models were run to assess determinants of overweight/obesity: the crude and adjusted models. The crude model assessed the association between overweight/obesity and each of the lifestyle, psychosocial, eating behavior, individual/social demography, and environmental factors independently, while the adjusted model assessed the association between overweight/obesity for those factors, which were potential confounders (P < .25). The adjusted model with inclusion of psychosocial factors was performed on the age range of 15 to 19 years, while the full adjusted model without inclusion of these factors was done in 10 to 19 years old adolescents.
Sampling probabilities for each household were provided by the Central Bureau of Statistics. These were used to weight observations so that correct population-based inference could be made, given the finite population represented by the survey. 10 Descriptive data were presented as mean and SD; and adjusted odds ratios (aORs) were reported along with their 95% CIs, and a P value of <.05 was considered statistically significant.
Results
The age and anthropometric characteristics of the study population are summarized in Table 1. Among the total of 199 149 adolescents aged 10 to 19 years in the INHS 2013 data set, 193 795 (97.3%) with complete and valid anthropometric assessment had an average age of 14.1 ± 2.8 years and BMI-z score of −0.4 ± 1.3. The prevalence of AOO was 13.2% and was 13.8% for males compared to 12.5% for females. Female adolescents had significantly higher BMI-z scores than males.
Age and Anthropometric Measurements of Indonesian Adolescents Participating in the National Health Survey 2013.
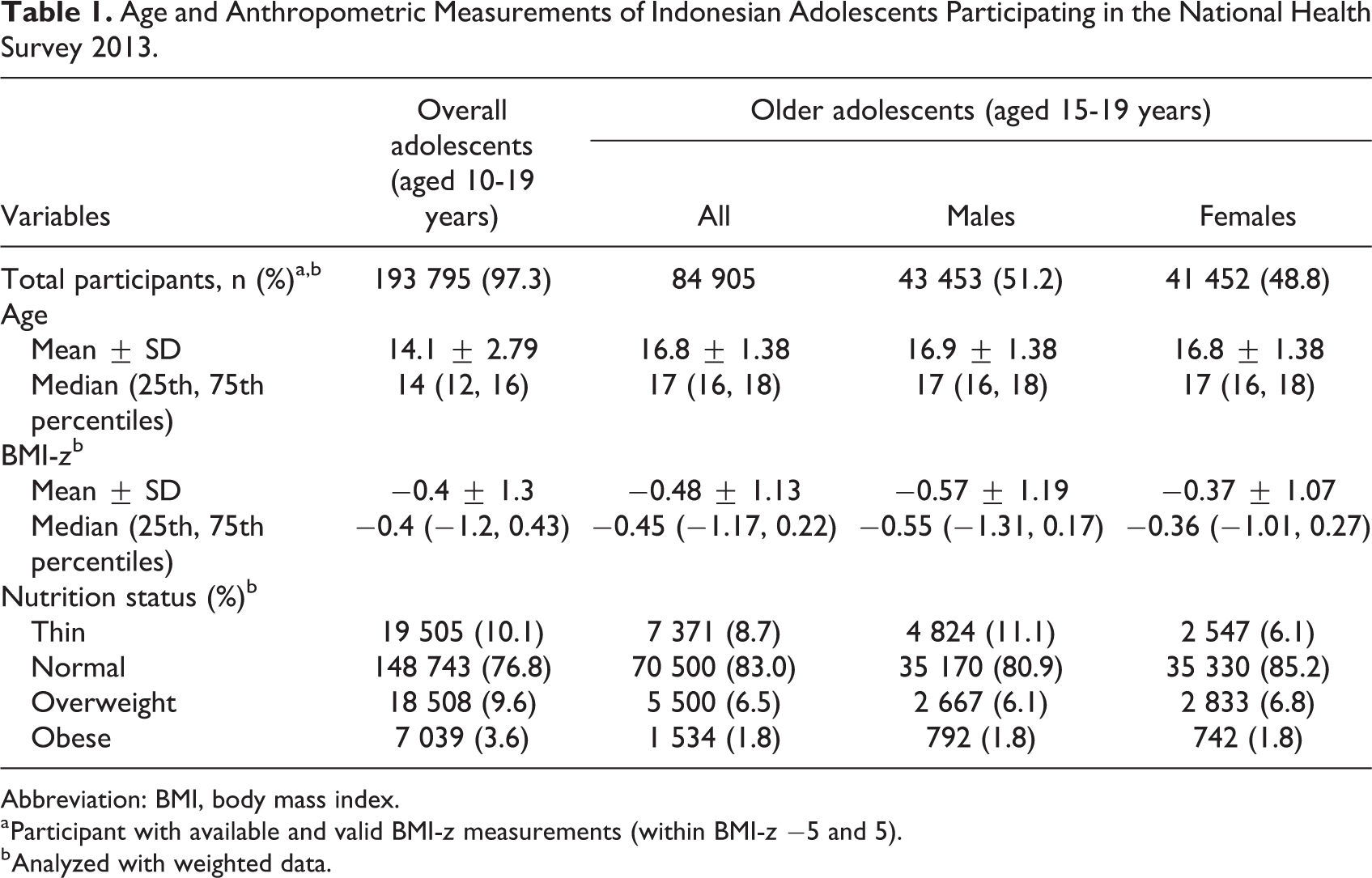
Abbreviation: BMI, body mass index.
a Participant with available and valid BMI-z measurements (within BMI-z −5 and 5).
b Analyzed with weighted data.
Age- and gender-specific analyses by province can be observed in Figure 2. Among the areas with the highest prevalence were Jakarta (20.9%), the capital city and a highly urbanized region, and Papua (19.4%), a remote area with a low human development index. Meanwhile, the lowest prevalence was observed in East Nusa Tenggara province (5.5%), the region with the highest stunting prevalence. 10 The prevalence of young adolescents with overweight and obesity in Jakarta was higher in males, whereas in older adolescents, the prevalence was higher in females. When compared to the report of INHS 2018, the findings indicate that within 5 years, the prevalence of AOO rose 5.2 percentage points (48% increase) in younger age adolescents (13-15 years) and up to 6.2 percentage points (85% increase) in older adolescents aged 16 to 18 years (Figure 3).
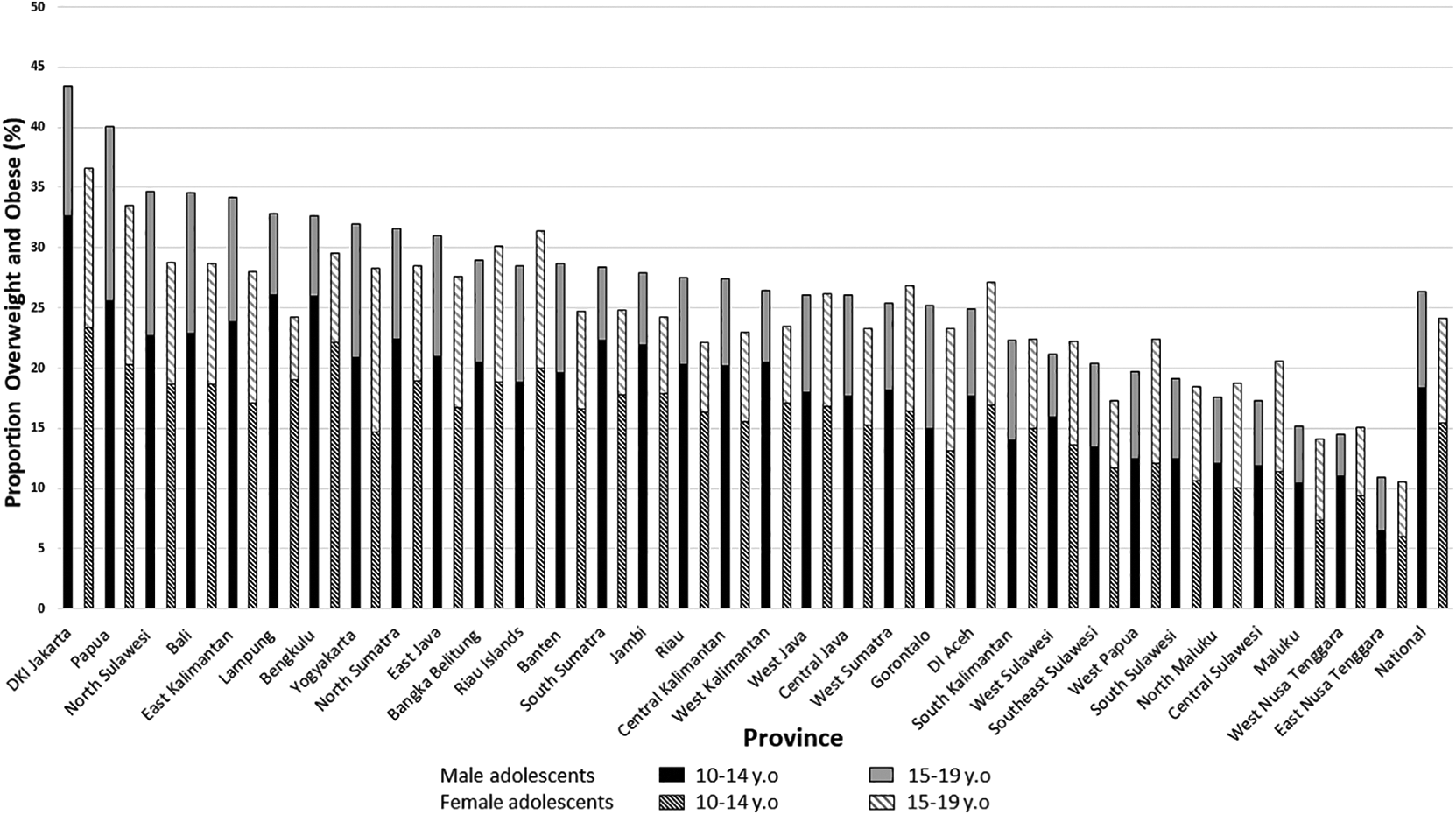
Prevalence of overweight and obesity in Indonesian adolescents by province in 2013 (n = 193 795).
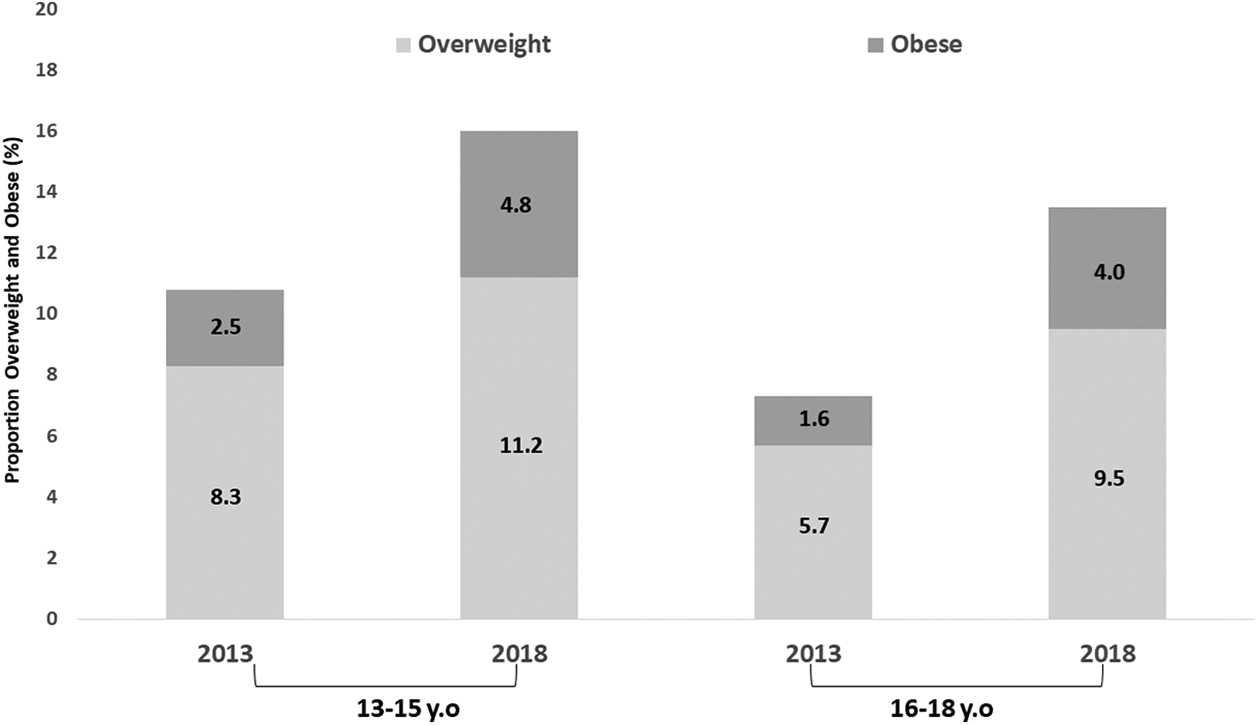
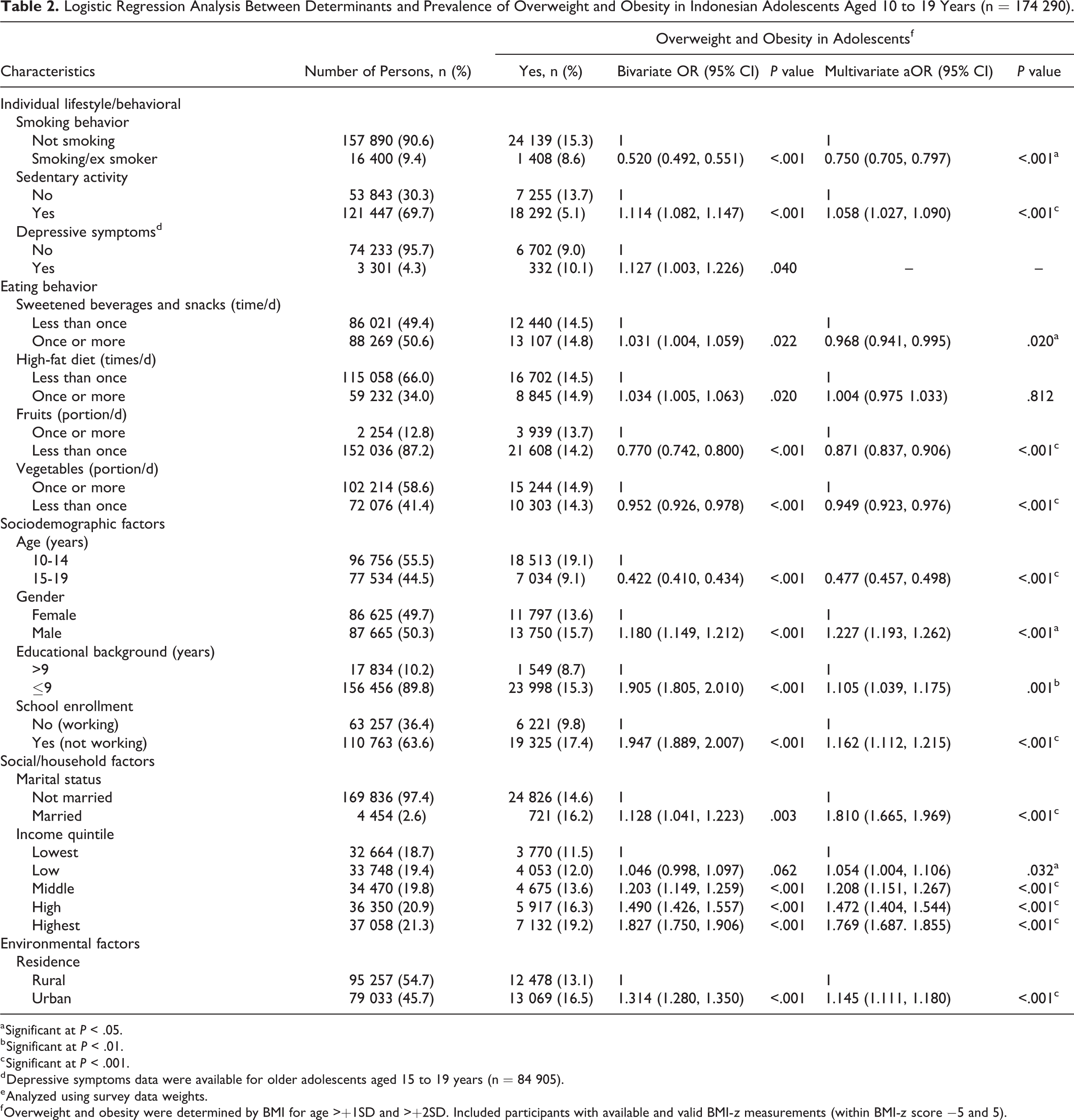
Table 2 presents that among 174 290 (87.5%) adolescents, most were aged 10 to 14 years and categorized as early adolescents (55.5%). More than half were male (50.3%) or lived in rural areas (54.7%), and most reported never being married (97.4%). Although married adolescents were minimal, we included marital status in the regression analyses as the raw number of those married enabled inference. The majority were still at school or not working (63.6%), and most reported education for 9 years or less (89.8%). The income quintiles revealed limited differences between household characteristics of participants.
Logistic Regression Analysis Between Determinants and Prevalence of Overweight and Obesity in Indonesian Adolescents Aged 10 to 19 Years (n = 174 290).
a Significant at P < .05.
b Significant at P < .01.
c Significant at P < .001.
d Depressive symptoms data were available for older adolescents aged 15 to 19 years (n = 84 905).
e Analyzed using survey data weights.
f Overweight and obesity were determined by BMI for age >+1SD and >+2SD. Included participants with available and valid BMI-z measurements (within BMI-z score −5 and 5).
Interactions with gender were assessed for selected significant covariates and are presented in Tables 2 and 3. For all adolescents (Table 2), the interaction analysis showed risk factors for AOO were sedentary activity (aOR = 1.06, 95% CI, 1.03-1.15) and high-fat consumption once or more per day (aOR = 1.05, 95% CI, 1.00-1.11). Furthermore, adolescents who were married (aOR = 1.81, 95% CI, 1.66-1.97) and in a higher income quintile, were male (aOR = 1.23, 95% CI, 1.19-1.26), not working (aOR = 1.16, 95% CI, 1.11-1.22), with educational background of less than 9 years (aOR = 1.11, 95% CI, 1.04-1.17), and living in an urban area (aOR = 1.15, 95% CI, 1.11-1.18) were significantly more likely to be overweight or obese. Adolescents who were older (aOR 0.48, 95% Cl = 0.457, 0.498), smoked (aOR 0.75, 95% CI, 0.71-0.80) or consumed fruits less than 1 portion per day (aOR = 0.87, 95% CI, 0.84-0.91), consumed vegetables less than 1 portion per day (aOR = 0.95, 95% CI, 0.92-0.98), and consumed sweetened beverages and snacks once or more per day (aOR = 0.97, 95% CI, 0.94-0.99) were less likely to be overweight or obese.
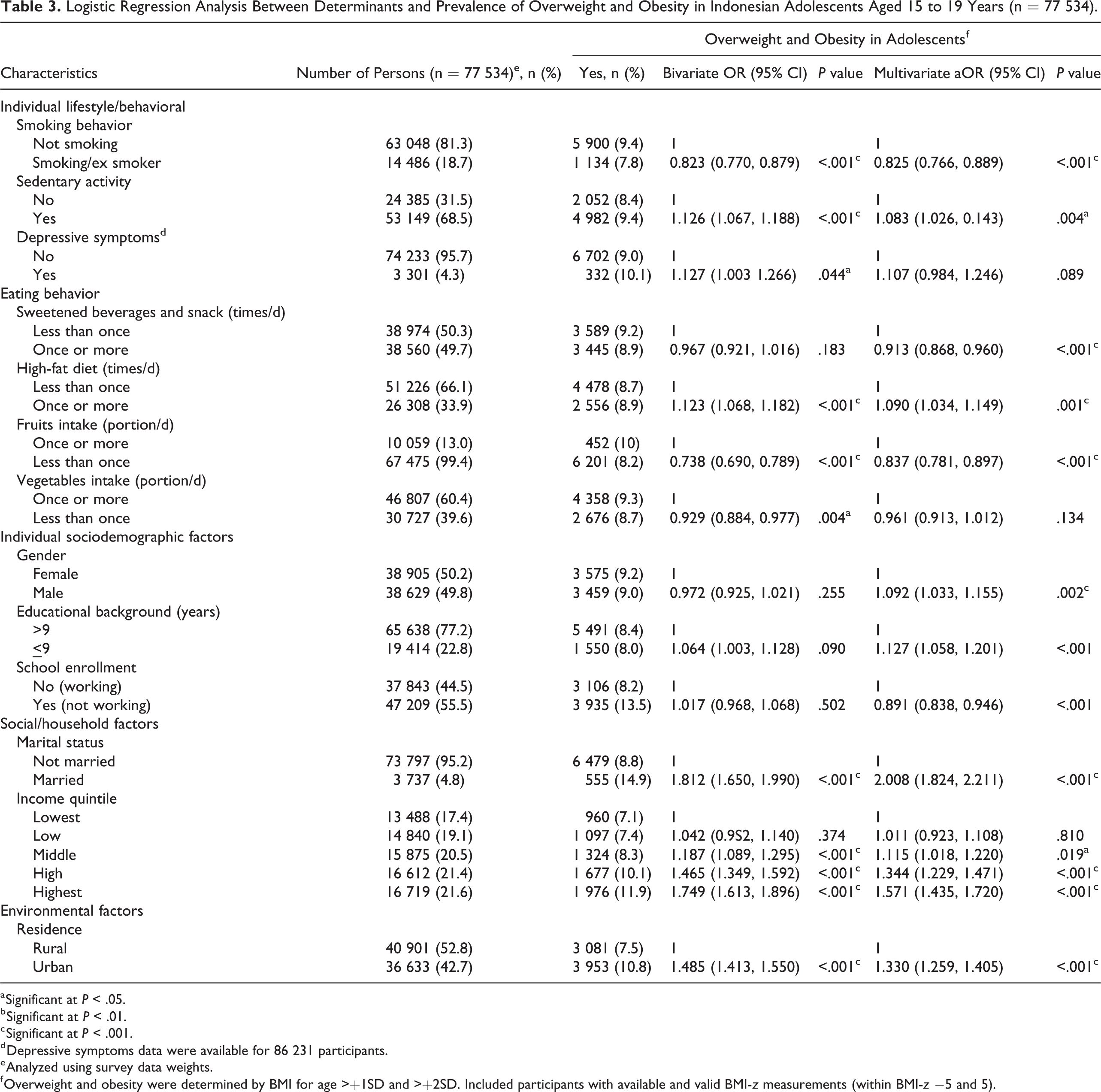
Logistic Regression Analysis Between Determinants and Prevalence of Overweight and Obesity in Indonesian Adolescents Aged 15 to 19 Years (n = 77 534).
a Significant at P < .05.
b Significant at P < .01.
c Significant at P < .001.
d Depressive symptoms data were available for 86 231 participants.
e Analyzed using survey data weights.
f Overweight and obesity were determined by BMI for age >+1SD and >+2SD. Included participants with available and valid BMI-z measurements (within BMI-z −5 and 5).
For late adolescents aged 15 to 19 years (Table 3), the risk factors for AOO were related to depressive symptoms (aOR= 1.11, 95% CI, 0.98-1.25), high-fat diet (aOR = 1.09, 95% CI, 1.03-1.15), and sedentary activity (aOR = 1.08, 95% CI, 1.03-0.14). In addition, late adolescents who were married (aOR = 2.01, 95% CI, 1.82-2.21) and in the middle to highest income quintiles (aOR = 1.12, 95% CI, 1.02-1.22; aOR = 1.34, 95% CI, 1.23-1.47; aOR = 1.57, 95% CI, 1.44-1.72 respectively), lived in an urban area (aOR = 1.33, 95% CI, 1.26-1.41), had an educational background less than 9 years (aOR = 1.13, 95% CI, 1.06-1.20), and male (aOR = 1.09, 95% CI, 1.03-1.16) were more likely to have AOO. Several factors related to lower risk of AOO were smoking behavior (aOR = 0.83, 95% CI, 0.77-0.89), consumed fruits less than 1 portion per day (aOR = 0.84, 95% CI, 0.78-0.90), not working (aOR = 0.89, 95% CI, 0.84-0.95), and consumed sweetened beverages and snacks once or more per day (aOR = 0.91, 95% CI, 0.87-0.96).
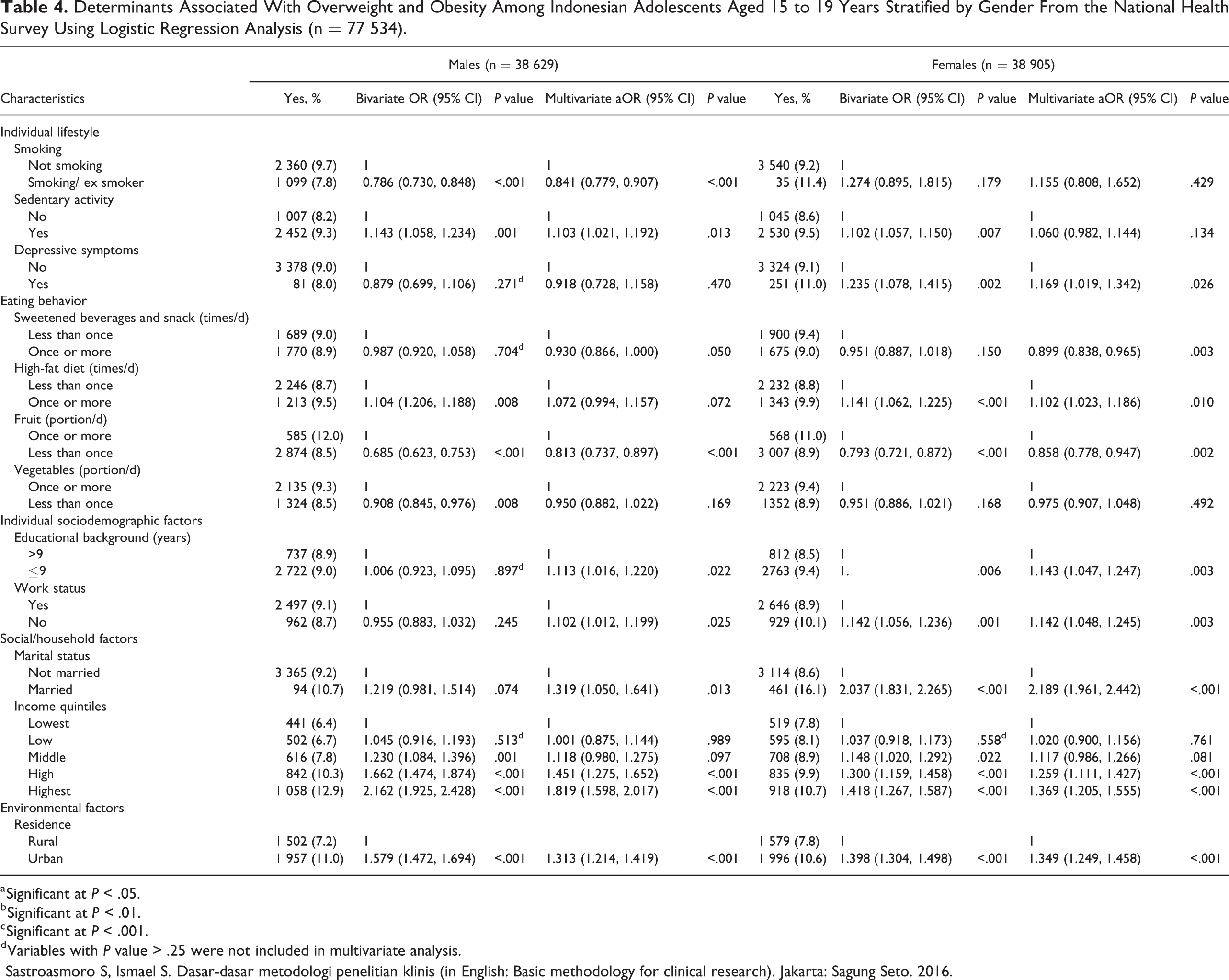
The following factors were associated with increased odds of AOO among males following multivariate adjustment (Table 4): high and highest socioeconomic quintiles (aOR = 1.45, 95% CI, 1.27-1.65 and aOR = 1.82, 95% CI, 1.60-2.02, respectively), sedentary activity (aOR = 1.10, 95% CI, 1.02-1.19), being married (aOR = 1.32, 95% CI, 1.05-1.64), living in an urban area (aOR = 1.31, 95% CI, 1.21-1.42), with school enrollment or not working (aOR = 1.10, 95% CI, 1.01-1.20), and an educational background less than 9 years (aOR = 1.11, 95% CI, 1.02-1.22). Conversely, risk of AOO was significantly less for male smokers or ex smokers (aOR = 0.84, 95% CI, 0.78-0.91), consumed sweetened beverages and snacks once or more per day (aOR = 0.93, 95% CI, 0.87-1.00), and consumed fruits less than 1 portion per day (aOR = 0.81, 95% CI, 0.74-0.90).
Determinants Associated With Overweight and Obesity Among Indonesian Adolescents Aged 15 to 19 Years Stratified by Gender From the National Health Survey Using Logistic Regression Analysis (n = 77 534).
a Significant at P < .05.
b Significant at P < .01.
c Significant at P < .001.
d Variables with P value > .25 were not included in multivariate analysis.
Sastroasmoro S, Ismael S. Dasar-dasar metodologi penelitian klinis (in English: Basic methodology for clinical research). Jakarta: Sagung Seto. 2016.
The following factors were associated with increased odds of AOO among females (Table 4): being married (aOR = 2.19, 95% CI, 1.96-2.44), high or highest socioeconomic quintiles (aOR = 1.26, 95% CI, 1.11-1.43 and aOR = 1.37, 95% CI, 1.20-1.55, respectively), an educational background less than 9 years (aOR = 1.14, 95% CI, 1.05-1.25), living in an urban area (aOR = 1.34, 95% CI, 1.25-1.46), having depressive symptoms (aOR = 1.17, 95% CI, 1.02-1.34), and consumed high-fat diet once or more per day (aOR = 1.10, 95% CI, 1.02-1.19). In contrast, AOO among females was significantly less likely for those who consumed sweetened beverages and snacks once or more per day (aOR = 0.90, 95% CI, 0.84-0.96) and consumed fruits less than 1 portion per day (aOR = 0.86, 95% CI, 0.78-0.95).
Discussion
The prevalence of AOO in Indonesia for 2013 was already high. Over 5 years, by 2018, it had increased substantially. The burden of AOO was slightly higher for males than females. Overall, factors associated with an increased risk of AOO included being sedentary, male, lower education, married, younger adolescent, school enrollment or not working, residing in an urban area, and within a family in the top wealth quintiles. Being sedentary and with lower education was a risk factor specific to male adolescents, while depressive symptoms, being married, lower education, and high-fat intake were risk factors specific to female adolescents. Higher intake of fruits and vegetables and fewer sweets did not protect against AOO if a high-fat diet was consumed.
Our study documented a higher AOO burden in male compared to female adolescents. This is consistent with findings in some studies in children and adolescents in Asian countries (eg, China and Japan) and in the Central European region (ie, Poland). 18 -20 However, these differed from findings from England, other Western European countries (eg, Ireland and Luxembourg), and the United States, where higher obesity rates were reported among female compared to male adolescents. 21,22 Lower female AOO may occur because females may pay more attention to foods as a way to influence health and are more likely to perceive themselves as being overweight than males. For example, female adolescents were more likely to report dissatisfaction with their weight. 19 It should be noted that distortion of weight perception may have detrimental influences on the psychological development of adolescents, although it strongly correlates with a desire to lose weight. 19 In a study conducted by Wong et al, 23 it was determined that the factors affecting eating attitudes are gender, body weight, body dissatisfaction, and the expected shape of the body. Toro et al 24 carried out a study in adolescents wherein the highest Eating Attitude Test scores, with high being worse, were obtained from girls, older adolescents, overweight adolescents, adolescents imposing restrictive diets, and people who thought that they were obese and wanted to change their body size.
Adolescent age was identified to be an overall determinant of AOO. Older adolescence was protective against overweight and obesity. Lower odds of being overweight or obese in older adolescents might be explained by increased consciousness of body image and appearance, or by more recent changes in food consumption patterns seen in younger adolescents. 25 It is also of interest that for young adolescents compared to older ones, the risk of obesity (excluding those overweight) was higher. This may be caused by an obesogenic environment or an increase in exposure to advertisements, even at a young age.
We found that length of education, that is, more than 9 years, and school enrollment or not working were protective for AOO, regardless of gender. This confirms other reports that adolescents lacking in education have a higher risk of becoming obese as compared to well-educated ones, perhaps because those who are higher educated may be earlier adopters of healthy food preferences. 1 A study in South Africa 1 found that white African female adolescents who were both more highly educated and with a higher family income did not have increased odds of obesity; however, male adolescents did. School enrollment is also a primary factor in children’s nutrition. This is because most spend ∼6 hours a day, eat at least 1 meal, and perform most of their physical activities at school. 14 The presence of fast-food establishments within 0.1 miles of a school was associated with a 5% increase in obesity rates among students, whereas further distances were not associated. 14 Investment in school-based programs and fast-food policies are, therefore, central to addressing obesity. Moreover, the benefits of female education on maternal and child health outcomes have been well documented. 1
In our study, marriage is a risk factor for AOO in female adolescents, but not in males. In contrast, the South Africa study observed that marriage was a risk factor for obesity in male adolescents. 1 Other studies have also reported a higher risk of obesity in married persons. 26,27 This could be due to married couples spending more time eating together and more frequently consuming less healthy processed or fast food. They may also spend more time being sedentary and watching television and exercising less. Conversely, unmarried individuals may spend more time exercising and eating less, in part to make themselves more attractive. 26 Interventions for married couples could include premarital nutrition education programs, couple-based physical activities, and broader mass communication programs emphasizing healthy eating patterns. 26
Many studies in high-income countries reported that higher socioeconomic status (SES) is associated with a reduced risk of obesity. 28 -31 However, a systematic review of studies in children indicated that 35% of studies found no association between SES and obesity among girls, and 41% found no association among boys. 29 In many the reverse has been shown, that is increased SES is associated with an increased risk of obesity. 1,32,33 This is consistent with findings from our study, which demonstrate an elevated risk of AOO among the higher socioeconomic groups after adjustment for sociodemographics, residence, marital status, lifestyle, and depression. Highly educated female adolescents had significantly increased odds of AOO, like males. It has been noted that as a family’s economic status and earnings improve, they tend to adopt Western lifestyles that include a decrease in physical activity levels. 31,34 Increased wealth can also contribute to poorer food choices, such as increased energy density, bigger portion sizes, more frequent intake of processed foods high in animal fat, sugar, and salt, and reduced intake of fruits, vegetables, and grains. All have been attributed to rising overweight and obesity levels in LMIC. 31,35
A decrease in physical activity and the adoption of a more sedentary lifestyle are major factors in the increased rate of AOO. 1,36 However, we observed that being physically inactive is only part of the problem as inactive female adolescents did not have increased odds of AOO after adjustment for several confounding factors. The previous INHS 2013 report suggested that almost 30% of the Indonesian population was physically inactive. 10 There was a dose-dependent correlation between television watching and being overweight. Those who watched 4 or more hours of television per school day were the most likely to be overweight. In contrast, those reporting less than 1 hour of television watching per day were approximately 1.4 times less likely to be overweight. Those who were inactive were at 1.6 times higher risk of overweight than those who were sufficiently active. 37 Pearson and Biddle 38 conducted a systematic review across all ages that showed a clear association between screen time and unhealthy dietary intake, particularly high consumption of energy-dense snacks and drinks, total energy intake, and fast foods and low intake of fruits and vegetables. Adolescents in Indonesia participated in a number of sedentary behaviors, from television and movie watching to playing video games and reading.
A global analysis of physical activity levels published in The Lancet showed that in 2016, more than 80% of school-going adolescents aged 11 to 17 years did not meet recommendations. Bangladesh and India reported the lowest prevalence of inadequate activity in girls, potentially explained by societal factors such as required domestic and other activities around the home. 39 However, measuring levels of physical activity in children and adolescents can be challenging, especially in younger children. Many studies relied upon self-reported questionnaires or interviews. Although these may be easier, they are less reliable than direct measurements of activity. 31 Younger children might not be able to report their activities appropriately, leading to recall bias.
Our study demonstrated that residing in urban areas increases the risk for AOO. This is similar to the results of most countries in which children living in urban areas were more likely to be overweight obese than in rural areas. 32 Indeed, urbanization and globalization are fueling the nutrition transition. 36 The increase in obesogenic urban environments is likely a major driver of the obesity epidemic. 1 Urbanization generally results in the adoption of a more Westernized lifestyle, as described above, which is conducive to obesity and cardiometabolic risk factors. 36 Unhealthy dietary choices increase the risk and prevalence of obesity and are part of the nutritional transition from rural to urban areas. 1
Many studies have assessed the association between sugar-sweetened beverages and body weight, BMI, or body fat content. Results have ranged from a strong association to no association. 14 In our study, adolescents who consumed sweetened beverages and snacks once or more per day did not show an association with the risk of AOO. However, we acknowledge this could be affected by misclassification of sweetened beverages and snack consumption, thereby limiting inferences for sugar consumption. Studies on the association between dietary fat, including fast-food consumption and obesity in children, have also shown conflicting results. 40 Lieb et al 31 reported that from 1980 to 2006, American adolescents increased consumption of fat and carbohydrates by 4% and 15%, respectively, and obesity rates tripled. In our study, consumption of fat that is known to be high in saturated and trans fats was associated with AOO.
Most people who use tobacco begin during adolescence. 41 Globally, over 4.7 million middle- and high-school students currently use tobacco. Some studies found that cigarette smokers weighed less than nonsmokers and that former smokers were of similar weight as nonsmokers. Studies examining the relationship between BMI and smoking in adults show that cigarette smokers had a lower BMI than nonsmokers or “never smokers.” 42 When similar analyses were conducted among young, middle, and older adolescents, the relationship between smoking frequency and lower BMI became stronger over time in males, but less so in females. 43 In this study, we note that the prevalence of smoking in male adolescents was much higher than that for females, and we found an inverse association between smoking behavior and AOO. This association persists in male adolescents after adjustment for age, educational level, marital status, residence, family wealth index, sedentary activity, and eating behavior.
The pathophysiologic mechanisms for the association between smoking and weight are unknown. 43 One explanation may involve changes in glucocorticoid metabolism and psychosocial stress associated with smoking. 43 Nicotine has small metabolic effects and can suppress appetite. 42 In addition, smoking has a reported antiestrogenic effect in young people, which may reduce fat deposition, leading to weight loss. However, it is important to note that the impact of smoking on body weight may dissipate over time. Long-term smokers are heavier than never, or former smokers, and high-frequency smokers are more likely to be obese than other smokers and nonsmokers. It has been proposed that long-term smoking interferes with glucose tolerance, insulin sensitivity, and insulin resistance and leads to hyperinsulinemia. 44 Studies of smoking to reduce weight in young people 45,46 suggest more harmful and few, if any, beneficial effects. Indeed, the adverse effects on metabolic and hormonal changes due to smoking contribute to multiple noncommunicable diseases. As such, smoking in adolescence is a risk factor for developing abdominal obesity among both genders and for overweight in women in adulthood. The prevention of smoking during adolescence is important to promote healthy weight and to decrease morbidity related to abdominal obesity. 43
Our study also confirmed the association between obesity and depressive symptoms in adolescents, especially in females. This increased vulnerability to both depression and obesity suggests a possible bidirectional association. Possible mechanisms include behavioral and lifestyle factors as well as biological and genetic factors. 47 Adolescents who are depressed may change their appetite, dietary, and sleep patterns, which can affect psychomotor retardation, anxiety, or somatization 48 and influence weight gain or loss. Adolescents are more inclined to favor carbohydrate-rich food, which may provide pleasure or comfort and can increase sedentary activity and affect sleeping disorders. These factors increase the risk of obesity. Subsequently, obese adolescents may experience stigmatization, poor body image, and low self-esteem, which exacerbate their vulnerability to depression. 49 A meta-analysis of prospective studies found that the association between obesity and depression was greater in adolescents than other ages, particularly for females. 50 Marmorstein et al 51 reported an association of greater depression with obesity primarily for adolescent females. They found that obese female adolescents were at higher risk for depressive symptoms in adulthood and that female adolescents with depressive symptoms were at higher risk of obesity in adulthood. Mannan and colleagues 47 found that more females were dissatisfied with their bodies, regardless of their actual weight, whereas males were dissatisfied when objectively overweight. Adverse life events, such as bullying, as well as reduced self-esteem, can produce stress, which may, in turn, increase the risk of obesity and depressive symptoms in adolescent females more than in males. 49
An understanding of the determinants of AOO is critical to developing the best policies and strategies for intervention. There is an urgent need to evaluate population-based interventions for obesity, including changes to environmental determinants. Such efforts must be based on a detailed scientific understanding of the multiple interlinked risk factors. Prevention of AOO is essential and likely more effective compared to its treatment and related complications. However, preventive and health protection programs for young children and adolescents are lacking and require attention. 52 This is especially important, given that AOO is a high risk for noncommunicable diseases later in life. Future analyses should define the attributable fraction of AOO for other adverse health and psychosocial conditions to help determine priorities for intervention.
The major strength of the present study is a large number of participants and adjusted analyses for multiple covariates. A limitation relates to the cross-sectional design that precludes the inference of directionality and causality. As this was secondary data analysis, several key determinants were not part of the primary data collection, including total energy and fat consumption, birth weight, pubertal status, ethnicity, obesity in the family, and smoking behavior in the family. Data for sweetened beverages and high-fat diet were based on reported frequency of daily consumption, not by measuring amounts consumed. These data should be collected in future surveys focused on AOO.
Conclusions
The prevalence of overweight and obesity among Indonesian adolescents has rapidly risen over the past 5 years, especially in older adolescents and males, and with gender-specific risks. This increase is potentially linked to specific determinants, such as being sedentary, male, lower education, married, younger age, school enrolment or not working, residing in urban areas, higher family wealth, and more frequent consumption of fatty foods.
Common and different risks exist for males and females. A sedentary lifestyle and lower education were specific risk factors for male adolescents, while depression, being married, and high-fat intake were specific to female adolescents. Higher intake of fruits and vegetables and fewer sweets did not protect against AOO if a high-fat diet was consumed. Educational attainment more than 9 years was a protective factor for overweight and obesity in both males and females. There is urgent need for customized gender-specific multisectoral interventions and trials to identify strategies for lifestyle change. Our findings call for more customized prevention efforts and a multisectoral strategy to reduce the risk of obesity and associated disorders.
Footnotes
Acknowledgments
The authors thank the National Institute for Research and Development and the Ministry of Health for their approval to utilize the national data set that was provided to Atmarita. The authors also thank Wanda Lasepa, Atikah, and Hanifa, who helped the authors arrange the administrative work for this study.
Authors’ Note
RA, F, M, A, and AHS conceptualized the study. F, M, and RA cleaned and analyzed the data. RA, A, F, M, and AHS reviewed the tables and figures. RA, F, and M drafted the manuscript. RA, A, KAS, S, WL, and AHS reviewed the draft manuscript. RA coordinated the team and was responsible for making the final decision on the manuscript. All authors read and gave the final approval to the paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the Directorate of Research and Community Services, Universitas Indonesia through Q1Q2 grant no. NKB-0233/UN2.R3.1/HKP.05.00/2019. This study was also funded by the Ministry of Research, Technology and Higher Education of the Republic of Indonesia (no. 1/E1/KP.PTNBH/2019 and 234/PKS/R/UI/2019.
Highlights
The increase in overweight and obesity in Indonesian adolescents is alarming, especially in younger adolescents and males. These findings call for innovative and customized interventions, particularly for dietary shifts and lifestyle changes.