
Abstract
Background:
Despite the rising double burden of malnutrition, adolescent nutrition has received little attention in Indonesia. Eating and physical activity behaviors established in adolescence are known to track into adulthood and may contribute to chronic diseases in later life. This study aimed to explore the eating behaviors and physical activity of Indonesian adolescents, and their influencing factors.
Methods:
The study, designed as a qualitative study, was conducted in 2 selected districts in Indonesia: Klaten and Lombok Barat. Data were collected through immersion, open and informal discussions, and participant observations with 302 adolescent girls and boys.
Results:
The eating and physical activity behaviors of adolescent boys and girls are influenced by contextual changes in their family lifestyles and environment. The adolescents in this study only conflate physical activity with participation in sport. Even when a wider view of physical activity is cast, their level of physical activity remains low, especially for adolescent girls. Adolescents and their families generally eat 3 meals a day, with schools an important source of food for adolescents. Adolescents skip breakfast at home, and breakfast and lunch are usually purchased and eaten at school. Fewer families cook and families rarely eat together due to increasingly busy lives, increased mobility, and digital connectivity.
Conclusions:
The rapid contextual shifts taking place in Indonesia influence the home, school, and peer environment to shape eating behaviors and physical activity among adolescent boys and girls. Gender-responsive multicomponent school-based interventions have the potential to serve as an important entry point for influencing adolescent nutrition.
Background
In the past few decades, the number of adolescents, defined as persons aged 10 to 19 years, 1 has significantly increased, with an estimate of 1.2 billion worldwide today, and the number is expected to grow to 1.3 billion by 2030. Approximately 90% of adolescents live in low- and middle-income countries (LMIC), 2 and Indonesia alone is home to 45 million adolescent boys and girls. 3
The coexistence of under- and overnutrition, known as the double burden of malnutrition, is on the rise among Indonesian adolescents. The 2018 National Basic Health Research Survey showed that 26% of Indonesian adolescents aged 13 to 15 years were stunted, 9% thin and 16% overweight. The older group of adolescents aged 16 to 18 years showed a similar prevalence, with 27% stunted, 8% thin, and 14% overweight. Notably, the prevalence of stunting and thinness was higher among boys than girls. 4 The ongoing dietary and nutrition transitions, combined with an increasingly sedentary lifestyle, may collectively contribute to the dual burden of malnutrition in Indonesia. Evidence has indicated that poor eating behaviors are ubiquitous in adolescence, with only 3.6% of adolescents aged 15 to 19 years consuming 5 or more portions of fruits and vegetables a day, and 11.2% consuming instant noodles at least once a day. 4
Adolescence is a critical period for the acquisition of health- and nutrition-related behaviors. It is well accepted that eating and physical activity behaviors established in adolescence continue into adulthood 5,6 and may contribute to nutrition-related chronic diseases in later life. 7 -9 The nutritional status of adolescent girls is a strong determinant of low birthweight and the health, nutrition, and well-being of their offspring, 10,11 especially in Indonesia where 1 in 9 girls is married before the age of 18. 3 Growing evidence also suggests that the children of overweight pregnant women are at an increased risk of being overweight and having noncommunicable diseases in later life. 12 -14 Adolescence is therefore an opportune time to intervene to protect, promote, and support the optimal nutrition of both adolescents and the next generation.
Few policies and programs target improved adolescent nutrition in Indonesia. Weekly iron folic acid supplementation for adolescent girls recently began in the country but is still at a nascent stage. Notably, major gaps exist in our understanding of adolescents’ nutrition-related behaviors and the influencing factors.
This study aims to describe the dietary and physical activity behaviors of Indonesian adolescent girls and boys and to understand related influencing factors. Obtaining insights into these behaviors and influencing factors will help design policies and programs to improve adolescent nutrition.
Methods
Study Setting and Participants
This study was conducted in 2 selected districts in Indonesia: Klaten in Central Java Province and West Lombok in Nusa Tenggara Barat Province. The districts were selected having taken into account differences in cultural context, infrastructure, and adolescent nutritional status. Klaten and West Lombok have a population of 1.2 million and 650 000, respectively. Klaten has a higher population density and Human Development Index than West Lombok. Seven study sites were selected from urban, peri-urban, and rural areas in both districts, taking into consideration digital and internet connectivity, the accessibility of high schools, and adolescent population size. 3
Researchers resided in 20 households that were selected purposively in the 7 study sites to ensure a diversity of socioeconomic status. Prior to data collection, the researchers engaged in informal discussions with community members, explaining the nature of the study, and the importance of staying with ordinary families and not being afforded special guest status. The study participants included members of the host households, the immediate neighbors of the host households, local service providers, and a range of other people, mostly those with whom the host households interacted. The researchers interacted with 15 adolescent girls and 11 adolescent boys aged 12 to 19 years old, who lived in the host households, and approximately 860 people across all study sites, of whom 302 were adolescents (115 girls and 187 boys) aged 12 to 19 years.
Qualitative Research Approach
This qualitative research was conducted from August to November 2016, applying the internationally recognized Reality Check Approach, 15 which extends the tradition of listening studies 16,17 and beneficiary assessments, 18 with researchers residing with the people whose views are being sought.
The study team comprised 17 field researchers, consisting of 9 male and 8 female trained researchers, with past experience in conducting qualitative research in public health topics. Each researcher had all participated in a data collection training for this study, which emphasized the good practice of reflexivity, understanding, and mitigating bias, maintaining informality and ethical considerations in conducting qualitative research in addition to training on how to collect data through discussions and observations in relaxed forms of interaction with study participants. The trained field researchers lived with the adolescents and their families for 4 days and nights, joining their everyday lives and having iterative, detailed conversations, and intense interactions with people in their own homes and own daily environment to better understand and contextualize their perspectives and experiences. This relaxed form of interaction with the study participants ensures that power distances between researchers and study participants are diminished and provide enabling conditions to gain rich contextual insights into the reality faced by the adolescents, their families, neighbors, and the wider community.
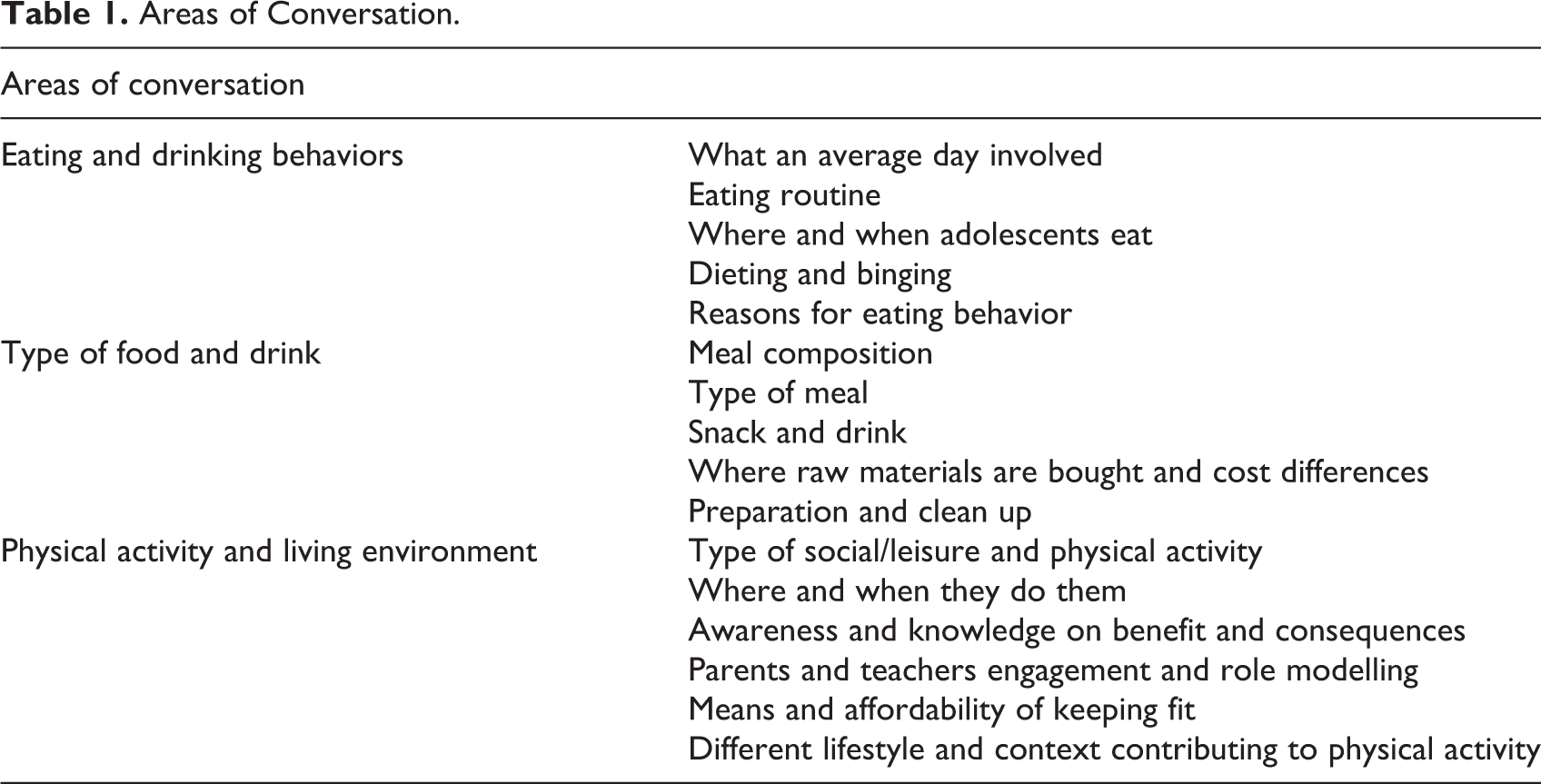
Data were mainly collected through conversations, participant observations and interactions with study participants. Each researcher developed field notes based on the conversation and observation results, and the notes were shared with the research team during the data analysis stage. The immersion approach provides researchers with opportunities to triangulate different methods (conversations, discussions, observations, experiences, and use of visuals, including photographs) and different study participants (adolescents, their families, teachers, and communities) to obtain data. Areas of conversation were developed, which served as a guide to ensuring that conversations, discussions, and observations were purposive (Table 1). No analysis of differences was conducted among field researchers, but quality of data was controlled by intensive sharing of conversations, observations, and experiences among the researchers with the supervisors.
Areas of Conversation.
The study protocol was approved by the ethics review committee of the Institute of Research and Community Service of University Atma Jaya, Indonesia. All field researchers were briefed on ethical considerations before data collection commenced and signed a Code of Conduct on Confidentiality and Child Protection Policy declarations. Informed verbal consent was obtained from all study participants for using their stories and insights for study reports and publications.
Data Analysis
An interactive, ongoing process for data analysis was applied. Upon completion of each of the 2 rounds of data collection, a collaborative analysis was conducted by the researchers, which involved sharing all conversations, observations, and experiences related to areas of conversation. This process enabled extensive triangulation of information, as the same topics were explored through different researchers, from different people’s perspectives, and from different locations, times, and data collection methods.
Upon completion of the collaborative analysis, emerging narratives were identified, and an analytical framework was established. The framework consisted of 3 stages, namely familiarization (immersion in the findings), identification of themes, and charting (finding emerging connections). 19 The conventional fourth step, “interpretation,” is purposely eschewed to ensure that the study brings forward people’s perspectives instead of the interpretation of the researchers. Multilayered quality assurance was carried out through internal peer reviews, with special concern given to ensuring that the research retained the perspectives of the study participants, and other people with whom the field researchers engaged.
Results
Changing Context
The study participants shared significant recent changes in their contextual environment which had impacted their daily lives. Due to increased cash needs for both regular and periodic expenses, many family members, including the adolescents, seek various formal or informal work opportunities. The adolescents also reported needing their own money for motorbike costs, mobile phone credit, purchasing snack food between meals, smoking, dating, and sports activities. On average, adolescents received daily allowances of Indonesian Rupiah (IDR) 5000 to 15 000 (approximately USD 0.40-1.2). Some parents also shared that adolescents tended to have longer school hours than previous generations. People were more digitally connected but felt that they had less interpersonal communication, interaction, and sense of community. All study households had electricity, and most had access to television, radio, mobile phones, and the internet; only 5 of 26 adolescents did not have their own mobile phones. Improvements in physical infrastructure, especially roads, have also led to greater access to food markets and sports facilities.
Families shared that these changes have caused families to have less quality time together. Fewer families cooked and ate together and participated in sporting activities, particularly in peri-urban areas. Adolescents had less physical activity, spending more time in front of the television, on the internet, and engaging with social media. The rapid increase in building has encroached on open spaces and public sports facilities that were traditionally used for physical activity and has eroded social interaction and community bonding.
Physical Activity of Adolescents
In general, adolescents were observed to be physically inactive. Adolescents viewed physical activity as synonymous with sport or specific exercise and did not recognize walking to school, manual labor, and physical chores as physical activity.
Physical activity was relatively lower among adolescent girls compared to boys. They were rarely seen playing sports outside, and the mandatory physical education (PE) session at school was often their only physical activity. This was explained by the prevailing view that girls should not be sporty. Adolescent boys said: “No, the girls will never play basketball,” and continued by saying that girls prefer to engage in social media on smart phones instead. In some cases, adolescent girls shared they have problems with obtaining permission from their parents to be outside after dark. Parents were increasingly worried about their daughters’ safety and had introduced stricter rules, ensuring that they returned home before dark. These curfews limited the opportunities for girls to engage in physical activity after school. Teenage girls also did not enjoy sport and being sweaty, because it negatively affected their appearance, which was important to them. On the other hand, the reason that some girls did participate in physical activity was to gain status and prestige by being selected to represent their schools.
Overall, boys were more active than girls and enjoyed community team sports and activities. Their main motivation for engaging in physical activity was social interaction and to improve their physical appearance. However, teenage boys also faced challenges in accessing sport facilities. With open spaces declining, facilities were increasingly charging user fees, which impeded access by lower socioeconomic groups. Working out at the gym was usually confined to boys from middle and higher socioeconomic groups but was gaining in popularity, as it was perceived to be associated with developing a film star body. Adolescent boys often followed the latest trends in sports and activities, including futsal, skateboarding, motorbike freestyling, and hip-hop dancing.
With almost every family owning at least one motorbike, children and adolescents were learning to ride as young as 7 years old and typically owned a motorcycle as they started high school. A mother in rural Klaten shared: “Back in the days we had to sweat it out, now the kids just have motorbikes.” Parents complained that their children demanded motorbikes as a condition for going to high school, and that motorbike ownership had become a status symbol that was often considered more important than education. As a consequence, boys and girls rarely exercised by walking or cycling to school, and adolescent boys spent less time on physical activities, such as football, and more time racing, modifying, and decorating their motorbikes. A motorbike was seen a key asset for dating, the “black magic to get[ting] a girlfriend and wife” as described by an adolescent boy in rural West Lombok.
Physical education sessions are often a mandatory component of the school curriculum in Indonesia. However, the observation results showed that the actual amount of exercise in PE sessions that students do is limited, with sessions often restricted to theory classes in the rainy season instead of the actual exercise. The space for PE sessions, especially in peri-urban schools, is often limited to a small cement school yard.
Adolescent Dietary Behaviors
Adolescents generally ate 3 meals a day but were increasingly eating outside the home. Many adolescents explained that breakfast was usually purchased and eaten at the first break at school and was considered an important social activity in forming and maintaining friendships and peer groups. Lunch was usually a cooked meal purchased from vendors at the school and often included a sweet drink. Adolescents generally spent IDR 5000 to 10 000 (approximately USD 0.40-0.60) a day on meals at school, and preferred fried foods.
Dinner was mainly eaten at home but was seldom eaten as a family. Instead, it was most often eaten in front of the television, displacing the traditional practice of eating together. Some adolescents, especially girls, preferred to buy food and drinks with their peers at school in the late afternoon before dinner time, and had no appetite once they returned home.
Meals at home were mostly bought from vendors or home-cooked by mothers and daughters. However, practicality, affordability, and convenience increasingly affect the eating behaviors of adolescents and their families. Nonworking mothers who had time to cook home meals would prefer to buy ready to eat foods than to cook, owing to the convenience of buying from the affordable mobile food sellers or food stalls. But the situation was different for working mothers, especially from the lower socioeconomic groups who had less resources to buy ready to eat foods. They usually cooked for their families once and found it challenging to prepare breakfast early for their children. In addition, very few homes had a dedicated dining table and chairs, irrespective of their socioeconomic status.
The increased rate of motorbike ownership has also changed access to food, making it easier to access traditional markets, supermarkets, and the mobile vendors commonly found in all but the most remote rural areas. A wider diversity of fresh and processed foods has become available throughout the day.
Home-cooked meals mainly consisted of rice with tempeh (Indonesian fermented soybean cake) or tofu, and small amounts of vegetables (cooked as soup or stir-fried), instant noodles, and flour crackers (with salt and mono-sodium glutamate). Among the lower socioeconomic families, chicken was consumed in small quantities (as shredded chicken in soup), eggs were eaten occasionally, and the consumption of chicken and other meat was usually confined to special occasions. Eating fruit was less common among adolescents. There was little variety in the home menu, even at weekends, with only a few well-off families buying takeaways from restaurants as a weekend treat.
Schools were an important source of food for adolescents. All high schools in the study had food vendors inside and outside schools often in cramped and overcrowded conditions. Arrangements differed among schools. Some controlled the provision of food within their premises by trying to prohibit students from buying food outside and/or limiting the vendors permitted in or near the school. However, these control measures did not extend to the types of food sold, and thus unhealthy food and beverages were common. The typical food sold at the school was mostly traditional dishes, such as local chicken soup, fried tofu, tempeh, battered vegetables, and sweetened beverages. Sweetened drinks, such as iced tea, instant coffee, chocolate drinks, and condensed milk topped with boiling water, were popular among the adolescents.
Adolescent girls and boys were observed to exercise their own agency in the choice of what and how they eat and drink. With regard to snacking habits, adolescents, especially girls, preferred to eat snacks or light meals with their friends after school. Snacks ranged from traditional cookies or finger food to chicken noodle or meatball soup and assorted sliced fruits with peanut sauce, with adolescents sharing that their overriding consideration in choosing foods was cost and taste. Despite the availability of western food such as pizza and burgers, adolescents preferred traditional foods. For adolescents who were out of school and working, food and drink choices were shaped by what was available at the workplace or from nearby vendors.
Discussion
Insights into the dietary behaviors and physical activity of adolescent girls and boys in Indonesia and the related influencing factors were obtained in this study, including the significant recent environmental and cultural changes that impact the adolescents’ daily lives. Adolescents were found to be eating away from home, purchasing food from vendors, and schools were identified as an important source of foods for adolescents. Adolescents were observed to be inactive, especially girls, which seemed to be influenced by emerging societal norms and peer pressure. A busier life, being more digitally connected, increasing use of motorbikes, and a changing landscape have reduced the time that families and community members spend together, lowered the physical activity levels of adolescents, and resulted in people preferring to buy prepared food from traveling vendors. Increasing mobility has changed access to food, affects the choices people make, and has changed their attitude toward food.
Evidence has shown that the availability of parks and open space is significantly associated with moderate to vigorous physical activity in children and adolescents. 20 -22 The provision of quality public outdoor spaces to support physical activity has been recommended as an important public health strategy; however, most of the studies discussing the quality and features of open spaces and public sport facilities were conducted in high-income countries, 23 -25 and this application in LMIC may need further studies.
The observed influence of leisure time screen use on adolescent physical activity in this study tends to confirm the findings of previous research conducted elsewhere. In the United States, boys aged 9 to 12 years who watched no television were significantly more active than those who watched any television, 26 and parental control of screen time was shown to be associated with higher physical activity and lower sedentary activity. 27,28 Similarly, a significant positive association between screen time and obesity has been reported in children and adolescents. 29 –31
In this study, girls were observed to be less active than boys, due to the emerging norms associated with the perception of femininity. Gender discrimination on physical activities has been widely documented, 32,33 showing that girls’ physical activity is influenced by social and gender norms. 34 Efforts should be made to create equal opportunities and stimulate girls and boys to participate in physical activity, 32 for example, by providing safe sport facilities for girls, and raising awareness of the importance of physical activities for both boys and girls, at schools and in communities. 33
In this study, both adolescent boys and girls regularly practice sport at school. Previous studies have shown that participation in PE increased the odds of adolescents having moderate to vigorous physical activity 35 ; however, the quality of PE classes needs to be enhanced to encourage higher participation by the students. Schools have been identified as an ideal setting for the promotion of adolescent physical activity, and school-based interventions are considered the most feasible and effective way to counter low physical activity, through either curricular or noncurricular activities (after-school sports), including collaboration between school and parents, and to encourage active transport to school. 36 -38 Further research is needed to encourage girls to participate in curricular and noncurricular physical activities and identify strategies to maximize movement and fun. 37,39
Social (family, peers, community), physical (fast-food outlets, convenience stores, school, street vendors), and environmental factors influence the food choices and eating behavior of adolescents. 40 -42 Previous studies have found that family meals during adolescence may have a lasting positive influence on dietary quality and meal patterns in young adulthood. 43,44 Girls were also found to have fewer family meals and lower breakfast consumption than boys; and family functioning, defined as the interpersonal interaction of the family unit, was associated with a higher intake of fruits and vegetables among adolescent girls, and more frequent family meals and breakfasts among adolescent girls and boys. 44 Another study found that family meals had a negative association with the intake of sugar-sweetened beverages among young adults. 43 These studies suggest that supporting good family relationships and interaction, and increasing the frequency of family meals may be important in improving the quality of adolescent diets; however, further studies are needed to understand the barriers and facilitators, including how to increase the awareness of parents of healthy food choices and eating behaviors. 42
This study also demonstrates that schools are an important source of food for adolescents. The school environment, including the regulation of food vendors and the types of food available, plays a major role in shaping adolescent eating behavior at school. 41 Adolescents perceive that food availability at school is a key factor in influencing their consumption, 41 and a limited selection of healthy food options on offer at school is a barrier to healthy weight gain, 32 suggesting the need to apply regulations on the sale of healthy foods and beverages at school premises. School policies which prohibit or restrict the sale of unhealthy food and sweetened beverages are associated with lower consumption of these foods. 45 Hence, policies to promote healthy foods and beverages need to be applied to all foods and beverages sold inside and outside the school premises. Although such restrictions are in place, access to healthy food and clean, free drinking water needs to be ensured. 45
School-based interventions, which provide additional physical activity sessions, such as integrating physical activity into the classroom or integrated classes about healthy foods, nutrition or physical activity, have been shown to be effective in encouraging adolescents to adopt a healthy lifestyle. 46,45 School nutrition programs, such as short in-class activity breaks, have been shown to increase the physical activity of school-age children and adolescents, and the provision of school breakfast can address short-term hunger, alleviate poor concentration, and provide an avenue to positively influence student eating behavior. 45 School-based programs designed as multicomponent education-based interventions delivered by teachers, and particularly those that involve parents, have also been shown to be highly effective, as parents and caregivers are considered to be key influencers on adolescent eating and physical activity behaviors. 46,47 The influence of peers, especially for girls, needs to be considered when designing a school-based intervention. Further studies may be needed to determine how peers influence healthy eating behavior and physical activity, and whether there are differences in the influence of peers in the social groups of adolescent boys and girls.
Few studies have examined the eating behaviors and physical activity of adolescent girls and boys in LMIC through qualitative research methods. A few limitations should be considered when interpreting the results of this study. First, the specific context and characteristics of the study locations may limit the generalizability of the findings. Second, adolescent girls’ voices were heard less than those of boys, as there were fewer opportunities to communicate with adolescent girls outside their homes due to the restrictions imposed on them, especially after dark. Third, it was not always possible for the researchers to accompany them to school and to be immersed in their school life. Fourth, in some locations, the diversity of conversations with adolescents was limited because it was difficult for the researchers to find adolescents hanging outside their houses to engage with.
Conclusions
This study highlights how the rapid contextual shifts taking place in Indonesia influence the home, school, and peer environment to shape eating behaviors and physical activity among adolescent boys and girls. Gender-responsive multicomponent school-based interventions, which integrate physical activity and nutrition education and strengthen school nutrition policies governing healthy food and beverages options, may be an important entry point for improving adolescents’ health and nutritional status. Informed by this assessment, further research is ongoing to explore and assess the range of potential policy and program levers to address this emerging priority issue.
Footnotes
Authors’ Note
H.T. and A.R. conceptualized the study and reviewed the analysis and interpretation; P.R-.C. and R.S. led the data collection, analysis, and interpretation, with oversight by D.J.; A.R. and J.H.R. wrote the first draft of the manuscript; all authors provided critical revisions of the manuscript; all authors read and approved the final manuscript. All data generated or analyzed during this study are available from the corresponding author on reasonable request. Verbal consents were obtained from the study participants to use their stories and insights for study reports and publication. Verbal informed consent was obtained from study participants to ensure they were fully aware and endorsed their views being shared, while also aligning with the methodology of maintaining an informal and relaxed approach. A more formal approach of obtaining written consent would have changed the dynamics between the study participants and researcher and could have potentially impacted the research findings. This more informal approach of obtaining verbal informed consent was approved by the ethics committee. Information was not shared and was kept confidential if consent was not obtained. All researchers involved in data collection signed a declaration that they had received people’s verbal consent to share insights into the collaborative analysis process. No individual names are included in this manuscript, nor are there location details or photos. All data (written and visual) were coded to protect the identity of individuals, their families, and communities. The study received ethics approval No. 793/III/LPPM.PM.10.01/08/2016 from the Institute of Research and Community Service of University Atmajaya, Indonesia. All field researchers were briefed on ethical considerations before data collection commenced, and signed Code of Conduct on Confidentiality and Child Protection Policy declarations. Consent was obtained from the parent or legal guardian of participants under the age of 16.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by The Government of Canada, the Canadian UNICEF Committee, and the 25th Team for the project “Addressing MNCH gaps to create scalable investments for the future” implemented by the UNICEF Indonesia Country Office.