
Abstract
Background:
Globally, the prevalence of child overweight has increased over the past few decades. The largest burden of child overweight is identified among upper-middle-income countries, such as Mexico. Breastfeeding has been identified as one of the key affordable and modifiable maternal health behaviors protecting against child overweight.
Objective:
To examine the association between breastfeeding and child overweight while sequentially controlling for individual, household, and area factors in Mexican children.
Methods:
Secondary data analysis using the 2012 Mexican National Health and Nutrition Survey which included risk factors for overweight on 2089 children aged 6 to 35 months and analyzed data to estimate fixed- and mixed-effects logistic regression models.
Results:
Overall, 9.0% of children were overweight and 71.1% of mothers reported any breastfeeding for ≥ 6 months. We found no evidence for a protective effect of any breastfeeding for ≥ 6 months on child overweight when compared to children who were never breastfed in the fully adjusted model and across all models (model 4, adjusted odds ratio [AOR] [95% CI] = 0.76 [0.31-1.86]). We identified risk factors for child overweight at the individual and area levels, with maternal obesity and offspring high birthweight being significant in the fully adjusted model and across all models (model 4, AOR [95% CI] = 2.26 [1.32-3.85] and 2.83 [1.44-5.56], correspondingly).
Conclusions:
Our results suggest shared obesogenic environment influences from which the overweight-obese maternal-child dyads are emerging in Mexican households. More research is needed to better understand these obesogenic environments grounded on the particular contexts among upper-middle-income countries.
Introduction
The global prevalence of overweight, including obesity, in children aged < 5 years was 5.9% in 2018 with the majority living in upper-middle-income countries, and the overall prevalence is expected to reach 10% by 2025. 1,2 There is strong evidence that risk factors within the first 1000 days (ie, conception through 2 years of age) and beyond contribute to developing child overweight and later-life obesity. 3,4 Scholars have expressed the need of further understanding its etiology and plausible behavioral and biological mechanisms at the individual and higher levels. 4,5 Discerning these underlying biological and contextual mechanisms may help prevent the onset of early-life overweight by informing the development of evidence-based policies and interventions.
Breastfeeding has been associated with short- and long-term positive maternal and child health outcomes. 6 Among breastfeeding benefits, studies mostly conducted in high-income countries (HICs) report a reduction in the risk of child overweight with evidence for a dose–response relationship with breastfeeding duration. 7 -11 Similar studies in low- and middle-income countries (LMICs), including low-, lower-middle, and upper-middle-income countries, such as Brazil and Belarus, have found no evidence for associations. 12 -15 Overall, the protective effect of breastfeeding on child overweight has been explained at the individual level through biological mechanisms such as active feeding and self-regulation, reduction of non-innocuous feeding behaviors by caregivers, and delivery of bioactive factors which contribute in regulating children’s appetite and metabolism. 16 However, this association may be confounded by household- and higher-level factors which may help explain differences in the child bodyweight outcomes by identifying wider social and contextual characteristics.
In Mexico, an upper-middle-income country grouped within the LMICs, 17 the prevalence of overweight, including obesity, in children aged < 5 years was 9.7% in 2012. 18 This has been the highest national point estimate over the past few decades and was higher than the aggregate prevalence among the upper-middle-income countries worldwide and among the Latin American and Caribbean countries in 2012 (6.9% and 7.1%, respectively). 19 Regarding breastfeeding, overall initiation and median duration of any breastfeeding in Mexico remained stable from 2006 (90.4%, 10.4 months) to 2012 (93.7%, 10.2 months). 20 While the prevalence of any breastfeeding for ≥ 6 months in Mexico may be higher when compared to other countries, child feeding practices and weight perceptions rooted in cultural norms and beliefs as well as other higher level factors (eg, household socioeconomic status [SES], urban or rural settings), may play important roles when examining the association between breastfeeding and child overweight. 21,22 Hawkins and colleagues examined individual-, family-, community-, and area-level factors using an ecological systems approach in the United Kingdom and found that breastfeeding duration in addition to risk factors at each of these levels were important determinants of early-life overweight. 7
The aim of this study was to examine the association between any breastfeeding for ≥ 6 months and overweight among singleton children aged 6 to 35 months overall, and according to household SES in Mexico while sequentially controlling for individual, household, and area factors. We hypothesized that children who received any breastfeeding for ≥ 6 months would have a lower risk of overweight compared with children who were never breastfed; that the 3-level factors would be associated with child overweight; and that the protective effect of breastfeeding on child overweight (if there was one) would differ by household SES. This analysis fills a critical gap by including individual, household, and area levels in fixed- and mixed-effects models allowing to identify risk factors while using a 3-level approach. This study contributes evidence-based information to discern early-life risk factors for child overweight and further develop policies and interventions in Mexico.
Methods
The institutional review board of Boston College considered this protocol exempt since it is a secondary analysis of data from the 2012 Mexican National Health and Nutrition Survey (ENSANUT for its acronym in Spanish), which are de-identified and publicly available. ENSANUT 2012 is a cross-sectional study planned and executed by the National Institute of Public Health in Mexico which allowed representativeness of rural and urban areas at national level and among 4 regions. 18 Child feeding data were collected from randomly selected households with children aged 0 to 35 months at the time of the interview (n = 6254). A subsample of children had additional information collected on child anthropometry including birthweight (collected through the birth report or self-reported by the mother when unavailable) and maternal characteristics including anthropometry, tobacco use, parity, delivery mode, and self-reported diabetes. As these factors have all been identified in the literature as key determinants of child overweight, we focused our analysis on this subsample. 4,5,7 We excluded children if they had missing or biologically implausible anthropometry data, were cared for by caregivers or grandmothers rather than children’s mothers, were multiples, and maternal anthropometry were missing. We excluded multiples since they are less likely to be breastfed than singletons. 23 Finally, we further excluded children from analysis by using subpopulation commands if they were aged <6 months since they had not yet reached the exposure-of-interest measure of any breastfeeding for ≥6 months. These exclusion criteria led to our final subsample which included individual, household, and area factors for child overweight on 2089 singleton children aged 6 to 35 months.
We assessed whether our final subsample (n = 2089) differed from the larger sample which included data on breastfeeding and child overweight but were missing relevant data such as child birthweight and maternal anthropometry. We also assessed whether children sampling weights (as provided in the infant feeding dataset) needed to be recalculated. In order to do so, we analyzed data using 2 strategies. First, we generated an indicator variable and ran a logistic regression model comparing those who would be included and excluded in our subset and found no significant differences in the dependent variable (ie, child overweight) nor in all other independent variables used in our models between the 2 groups. Second and following analytical recommendations from ENSANUT experts, we ran frequencies, weighted and unweighted percentages, and means to compare whether the whole infants sample and our subsample were comparable in terms of distribution of the independent and dependent variables. We found no significant differences and these strategies led us to conclude that the exclusions did not lead to discernable biases in the final subset, and it was unnecessary to recalculate the children’s sampling weights.
Measures
Breastfeeding
Our main independent variable was breastfeeding duration. During the child feeding interview, women were asked, “Did you ever breastfeed your child? If so, do you still breastfeed? Did you breastfed yesterday? For how long did you breastfeed?” From this information, we generated a 3-category variable: never breastfed, any breastfeeding for < 6 months, and any breastfeeding for ≥ 6 months. Any breastfeeding was defined as receiving exclusive, predominant, or partial breastfeeding or breast milk through bottles. We decided to use any breastfeeding for ≥ 6 months and not exclusive breastfeeding for 6 months given that the prevalence of the latter in our subsample was small and also to be consistent with other scholars who have used this definition. 12 -15
Individual factors
Child’s age as a continuous variable and sex were included. Birthweight in kilograms was collected through the birth report or self-reported by the mother when unavailable as a continuous variable, and we categorized it into 3 groups: normal 2.5 to 4 kg, low < 2.5 kg, high > 4 kg according to the World Health Organization (WHO) criteria. Delivery mode was reported as vaginal versus cesarean section. Very early introduction of liquids was defined as feeding newborns any type of liquid different than human milk within the first 3 days postpartum. Early introduction of complementary foods was operationalized as feeding children any type of liquid different than breastmilk or water, solid, or semisolid foods < 6 months of age. Maternal age was included as a continuous variable, and employment was conceptualized considering data on having a paid job, the number of hours worked during the past week, and formality. Full-time employment was defined as working ≥ 40 hours per week, and formality was defined as having a paid job with contributory social protection systems. 24,25 Both employment status and formality were combined into a 5-category variable. For maternal education, women were asked which was the last year of formal education that they had completed and was categorized into 4 groups. Women were asked their partner status, which we categorized as having a partner or not. Ethnicity was captured by asking mothers if, according to their cultural background, they self-identified as being indigenous or not and parity by asking how many children they had delivered alive which was included as a continuous variable. Women’s weight and height were measured by trained ENSANUT personnel. From these data, we estimated maternal body mass index (BMI) and classified women as underweight when <18.5 kg/m2; normal weight, 18.5 to 24.9 kg/m2; overweight, 25 to 29.9 kg/m2; and obese, ≥ 30.0 kg/m2 according to the WHO criteria. Finally, women were asked if at some point they had gestational or another type of diabetes and if they were currently using tobacco.
Household factors
Number of children aged < 5 years per household was included as a continuous variable given that scholars have identified a positive association between the number of children aged < 5 years in a household and the odds for child malnutrition. 26 Grandparents living in the same house were identified and included in the analysis given the evidence that they may influence children’s health outcomes including weight status. 27 Socioeconomic status was estimated by ENSANUT through principal component analysis, and we used tertiles categorized as low, medium, and high. Measurement of food insecurity was estimated by ENSANUT using the Latin American and Caribbean Food Security Scale categorizing households into 4 groups which we recategorized into 3 groups by collapsing moderate and severe food insecurity. 18
Area factors
Areas were classified according to population size into urban or rural settings. According to the survey’s design, urban was defined as population size of ≥ 2500 individuals and rural as < 2500 individuals. Mexico was divided into 4 regions: North, Center, Metropolitan (Mexico City), and South. 18 Both area and region factors were combined into a 7-category variable. The rationale for combining these 2 factors was that health-related behaviors and outcomes in Mexico appear to vary not only by region but also by area. 28 From an analytic point of view, this allowed to have a larger number of area factors to perform a 2-level mixed-effects analysis.
Child overweight
Trained ENSANUT personnel measured the child’s height or length in centimeters and weight in kilograms using standardized protocols. We analyzed child anthropometry from raw weight and height or length data provided by ENSANUT using the STATA restricted macro from the WHO growth standards. 29 Our outcome measure was child overweight defined as weight-for-height/length-z-score (WfL z-score), for age and sex, over +2 standard deviations according to the WHO child growth standards median, and we further excluded data flagged as biologically implausible according to the WHO guidelines (WfL-z < −5 or > 5).
Analytical Approach
We conducted a series of analyses to examine the associations between individual, household, and area factors with child overweight. Frequencies and weighted percentages for categorical variables, weighted means for continuous variables, Pearson χ2 tests, and unadjusted logistic regression models were used to examine bivariate relationships. We used step-wise fixed-effects multivariable logistic regression models to assess the association between breastfeeding duration and child overweight. This method allowed us to control for individual, household, and area variables successively as follows: Model 1 examined a bivariate association between breastfeeding and child overweight; models 2 through 4, sequentially, adjusted for individual, household, and area factors. To test whether the effect of breastfeeding duration on child overweight differed by socioeconomic level, we tested the interaction of SES and breastfeeding on child overweight in the fully adjusted model. The interaction was not significant (P > .05), and results are not shown. Additionally, in order to discard a potential dilution of the effect of breastfeeding on child overweight among older children, we ran stratified fully adjusted models by age groups and found no differences (results not shown). We estimated the variance inflation factors for each model to test for high intercorrelations between the independent variables and found no evidence for multicollinearity problems. While model 4 (fully adjusted) included a fixed-effect by area factors allowing to compare the odds ratios for child overweight by regions, it did not account for the multilevel structure in the subset. This means that we have clustered data: one maternal-child dyad per household (level 1, N = 2089) nested within areas regions in Mexico (level 2, N = 7). Multilevel models, also known as mixed-effects models, are specifically designed for data in which observations are nested within a group of reference. Therefore, multilevel modeling accounted for the fact that maternal-child dyads living in households from a given region share a context or frame of reference and that there may be differences between these regions. Consequently, we computed model 5 using a multivariable mixed-effects 2-level logistic regression model to account for area factors variance. Data were analyzed using the statistical package STATA SE version 15.1 (STATA Corporation). Survey commands were used to account for ENSANUT’s probabilistic design, including children sampling weights, primary sampling units, and strata. 18
Results
In our subsample, 71.1% of Mexican children received any breastfeeding for ≥ 6 months, and 9.0% were overweight. According to bivariate analyses, regarding individual factors, children were more likely to be overweight if they were classified as high birthweight compared to those with normal birthweight (unadjusted odds ratio [UOR] = 3.06, 95% CI: 1.65-5.66), if they were introduced with complementary feeding < 6 months (UOR = 1.60, 95% CI: 1.06-2.42), and if their mother was obese compared to normal bodyweight (UOR = 2.23, 95% CI: 1.30-3.81). We found no associations at the household level. Regarding area factors, compared to the north urban region, the south urban, and south rural areas were less likely to have overweight children (UOR = 0.45, 95% CI: 0.25-0.82; UOR = 0.30, 95% CI: 0.15-0.60, respectively; Table 1).
Descriptive Statistics (Weighted Percentages With Frequencies and Weighted Means With SD), and Unadjusted Odds Ratios (UOR) With 95% CI of Risk Factors for Overweight, Including Obesity, Among Mexican children Aged 6 to 35 Months.a
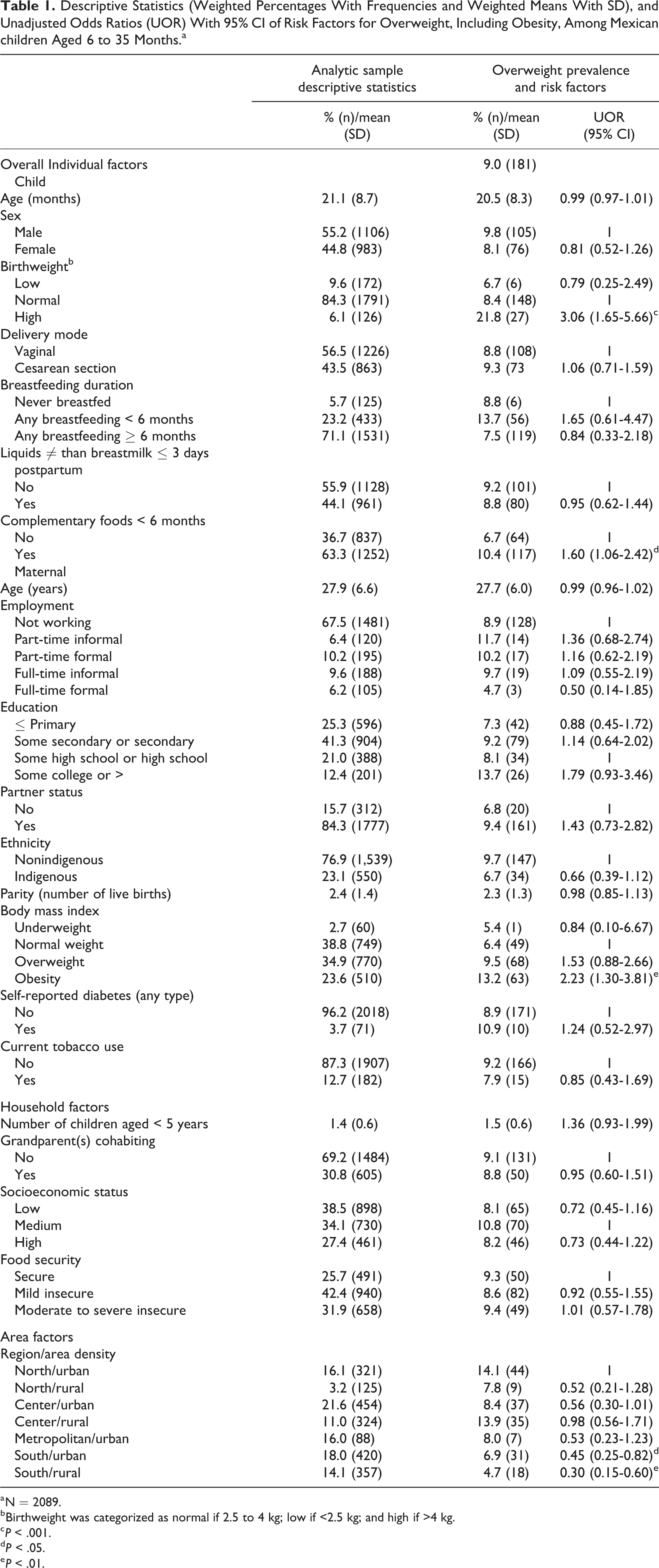
a N = 2089.
b Birthweight was categorized as normal if 2.5 to 4 kg; low if <2.5 kg; and high if >4 kg.
c P < .001.
d P < .05.
e P < .01.
Across all the models, we found no evidence for a protective effect of any breastfeeding for ≥ 6 months on child overweight compared to those who were never breastfed. After controlling for individual factors (model 2), child overweight was positively associated with high birthweight (adjusted odds ratio [AOR] = 2.98, 95% CI: 1.58-5.63), high maternal education (some college or more; AOR = 2.17, 95% CI: 1.03-4.57), and maternal obesity (AOR = 2.20, 95% CI: 1.31-3.69). After also adjusting for household factors (model 3) and area factors (model 4), all abovementioned associations were maintained with similar effect size and direction, and no household factors were associated with child overweight. Additionally, in model 4, children were less likely to be overweight when living in the south urban and south rural areas when compared to north urban (AOR = 0.48, 95% CI: 0.24-0.96; AOR = 0.37, 95% CI: 0.16-0.90, respectively). In the multilevel model (model 5), compared to their corresponding reference groups, risk factors for child overweight were high birthweight (AOR = 2.76, 95% CI: 1.70-4.48) and maternal obesity (AOR = 1.99, 95% CI: 1.31-3.03). No other risk or protective factors were identified. Level-2 (7 areas regions) variance was 0.02 (SE 0.04) with an intraclass correlation coefficient of 0.007 (SE 0.01; Table 2).
Models (Odds Ratios and 95% CIs) to Assess the Association Between Breastfeeding Duration and Individual, Household and Area Factors, With Overweight, Including Obesity, in Mexican Children Aged 6 to 35 Months.a
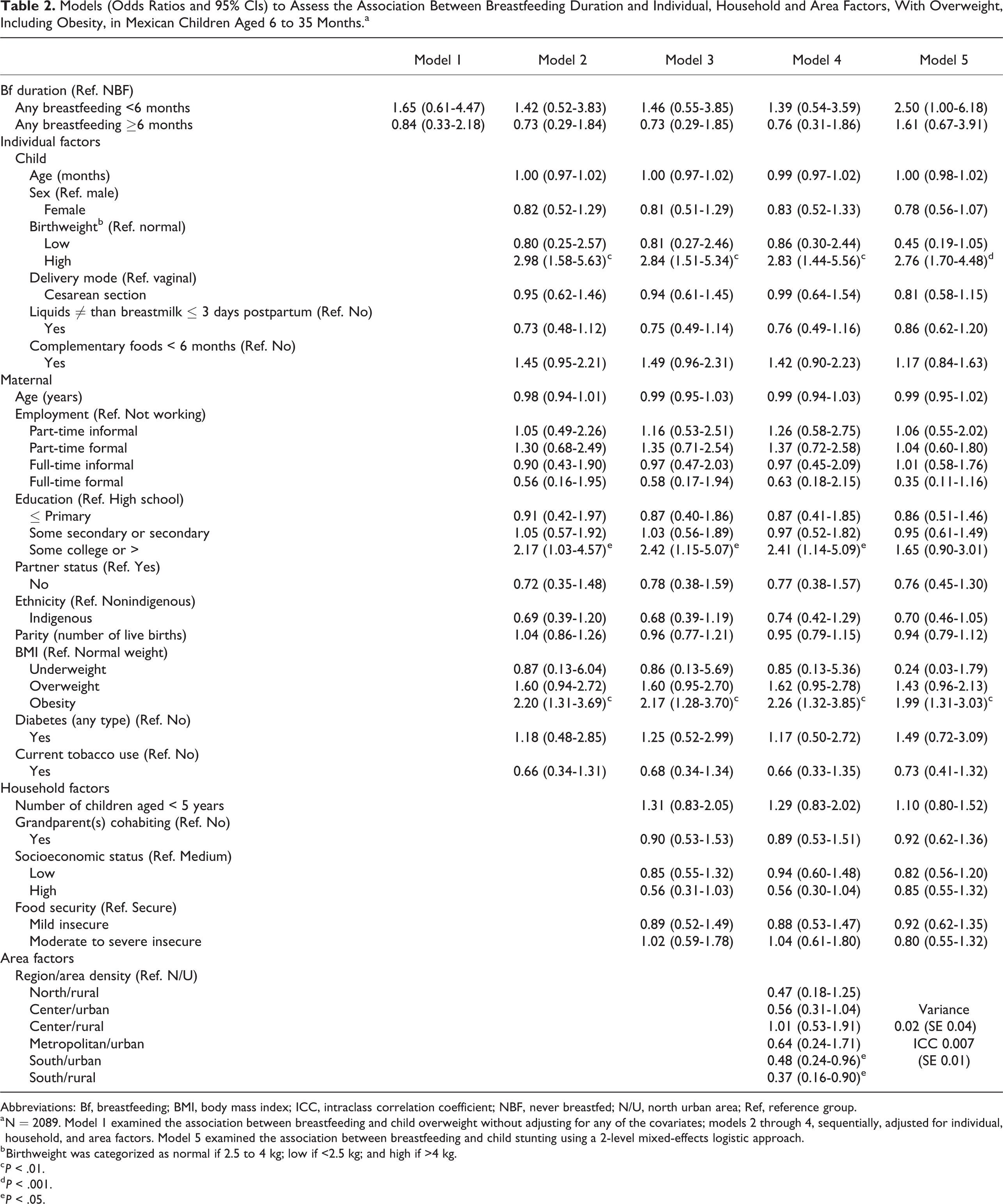
Abbreviations: Bf, breastfeeding; BMI, body mass index; ICC, intraclass correlation coefficient; NBF, never breastfed; N/U, north urban area; Ref, reference group.
a N = 2089. Model 1 examined the association between breastfeeding and child overweight without adjusting for any of the covariates; models 2 through 4, sequentially, adjusted for individual, household, and area factors. Model 5 examined the association between breastfeeding and child stunting using a 2-level mixed-effects logistic approach.
b Birthweight was categorized as normal if 2.5 to 4 kg; low if <2.5 kg; and high if >4 kg.
c P < .01.
d P < .001.
e P < .05.
Discussion
Among singleton children aged 6 to 35 months in Mexico in 2012, 71.1% were breastfed for ≥ 6 months and 9.0% were overweight. We found no evidence for a protective effect of any breastfeeding for ≥ 6 months on child overweight, overall or by household SES, when compared to children who were never breastfed. Consistent with the literature, we found that child high birthweight and maternal obesity were risk factors for child overweight across bivariate, multivariable, and multilevel models. 4,7
We hypothesized that children who received any breastfeeding for ≥ 6 months would have a lower risk of overweight compared with children who were never breastfed. We found no evidence for the hypothesized association and found no differential effect of breastfeeding on child overweight by SES. Our results coincided with findings from studies in LMICs, such as Brazil and Belarus, where no evidence was found for these associations. 12 -15,30 One plausible explanation for the lack of an association between breastfeeding and child overweight in LMICs may be that children in these countries were already at higher risk of overweight, including obesity, due to lower access to health care, obesogenic environments, cultural and social systems, and lack of policies (or nonenforcement of existing policies) that would help prevent overweight within the first 1000 days of life and beyond. 1 It may also be plausible that despite high rates of any breastfeeding for ≥ 6 months, norms and beliefs among Latin American and Caribbean countries, including Mexico, tend to favor heavier children, with common practices that often complement breastfeeding with other liquids and foods to achieve higher bodyweights. 21,22 While children in LMICs may be incrementally exposed to diverse cultural or contextual obesogenic factors as they age (eg, unhealthy complementary foods and adoption of obesogenic diets), studies in HICs have shown that breastfeeding for 6 months confers benefits, independent of other possible obesogenic factors, past this early period. 9,10,11 In HICs, there may be unaccounted exposures most likely related to healthier dietary patterns food systems and environments. Besides including breastfeeding duration and other child overweight-related variables, including these unaccounted exposures may better explain why some children are at lower risk of developing overweight across diverse country income levels. 31,32 These higher level data or norms and beliefs data around breastfeeding and bodyweight were not available in our subsample.
Secondly, we hypothesized that individual, household, and area factors would be associated with child overweight. While we found evidence for associations at the individual and area levels, we did not identify any risk or protective factors at the household level. Across all models, our results coincided with previous findings showing strong associations between maternal obesity and offspring high birthweight with child overweight. 4,7 Possible explanatory mechanisms may be shared genetics and obesogenic environments as well as epigenetics. In Mexico, the environment has become increasingly obesogenic in the past decade. According to our literature review, previously identified obesogenic factors of particular interest to early-life overweight in Mexico are a low breastfeeding-enabling environment and high intake of sugar-sweetened beverages (SSB). 33 -35 While we cannot discern whether child overweight in this analysis could be attributed to the abovementioned factors, it is worth pointing these out as plausible risk factors for further research. In a recent assessment of the breastfeeding environment in Mexico, guided by the “Becoming Breastfeeding Friendly” toolbox, scholars concluded that actions are urgently needed to protect and support breastfeeding and to develop pertinent policies and interventions. 35 Regarding SSBs and despite recent efforts to reduce its intake in Mexico, such as the implementation of an excise tax in 2014, interventions and other strategies are needed to reduce its intake during early-life. 36 In regard to region, children living in southern Mexico, either rural or urban, were less likely to be overweight. A plausible explanation of the lower likelihood of child overweight in the southern region may be the high proportion of undernutrition in this area. In 2012 nationwide, 13.6% of children aged < 5 years were stunted, while in the southern region, the prevalence peaked to 19.2%. 18 In addition, this is the poorest region in Mexico and has the highest concentration of indigenous population who are at higher risk of any form of undernutrition but lower risk of overweight overall. 18
By using the ENSANUT 2012, we were able to examine diverse individual, household, and area factors as well as use diverse analytical approaches. 37 One of the strengths of ENSANUT is that child and maternal anthropometric data were not self-reported but measured by trained personnel using age-pertinent standardized protocols. 18 This allowed us to estimate z-scores according to the WHO’s multicenter study, which included growth data from breastfed children in HICs and LMICs. 29
One of our main limitations is that ENSANUT cross-sectional design allows to solely describe associations where statistical evidence was found, and we cannot rule out reverse causation. Breastfeeding data were collected at the time of the interview with children’s age ranging from 0 to 35 months. We could not use breastfeeding as a continuous variable, and we had to exclude children aged < 6 months from analysis since they had not yet reached the exposure-of-interest criteria of any breastfeeding for ≥ 6 months. We relied on maternal recall of child feeding practices with some cases still breastfeeding and others reporting retrospective data from weeks up to 2.5 years. Scholars who have studied respondent’s recall bias on retrospectively collected breastfeeding data suggest that studies exploring breastfeeding practices be conducted either prospectively or within < 1 month following weaning. 38 We acknowledge that respondent recall bias on breastfeeding practices is likely present. Another important limitation is that we could not discern between children who were exclusively fed at the breast or those receiving breastmilk in bottles. Studies have found that exclusive breastfeeding confers the strongest protection against early overweight mainly explained through child suckling and energy self-regulation, actions not present when bottle feeding. 39 Regarding child birthweight, some mothers provided the birth record to ENSANUT interviewers which allowed collecting the weight at birth as reported by the health care facility; however, when unavailable, the mother self-reported their offspring birthweight which may have been subject to recall bias. In our analysis, we included all available risk factors previously identified in the literature; however, there were no available data on other factors that have also been associated with early overweight such as child antibiotic exposure, paternal BMI, and prenatal or pregnancy tobacco exposure (we used tobacco use at the time of the survey as a proxy for prenatal or pregnancy exposure), 4 probably leading to underspecified models.
In conclusion, according to our results, efforts should be aimed prenatally toward supporting women’s healthier lifestyles to prevent obesity and offspring high birthweight. While we found no evidence for a protective effect of any breastfeeding on child overweight, we recommend that postnatal efforts aim toward the promotion of positive maternal health behaviors, including breastfeeding given the strong associations with many other health outcomes. 16 Given previous analysis of the Mexican environment, at policy level, support is needed to improve the obesogenic and breastfeeding environment by raising national awareness of the benefits of breastfeeding, finding solutions to support breastfeeding initiation and continuation for working women particularly for those informally employed, and enabling food systems that provide affordable and accessible innocuous food and potable water. 24,33,35 Child overweight in Mexico and in other upper-middle-income countries has been rising significantly over the past few decades and is a public health concern 2 ; thus, it is imperative to continue research which helps identify early-life risk factors to inform evidence-based policies and interventions in order to prevent the onset of overweight as early as possible.
Footnotes
Authors’ Note
APC conceptualized the study, curated datasets, analyzed and interpreted data, and drafted the manuscript. MVC and SSH critically revised all analyses, data interpretation, and reviewed the manuscript. All authors approved the final version of the manuscript.
Acknowledgments
The authors would like to acknowledge the contribution of Dr. David T. Takeuchi, Dr. Sonia Hernández-Cordero, and Dr. Ida Caterina García-Appendini in critically reviewing this analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.